Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
Doi:10.1053/j.ajkd.2006.12.014
Aspirin Treatment Is Associated With a Significantly Decreased Risk of Staphylococcus aureus Bacteremia in Hemodialysis Patients With Tunneled Catheters Martin Sedlacek, MD,1,2 John M. Gemery, MD,1,2 Ambrose L. Cheung, MD,2Arnold S. Bayer, MD,3,4 and Brian D. Remillard, MD1,2Background: Hemodialysis patients with tunneled catheters are at increased risk of bacteremic Staphylococcus aureus infections. In vitro and in vivo studies showed that aspirin has direct antistaphy-lococcal effects by inhibiting expression of ␣-toxin and matrix adhesion genes through activation ofsigma factor B stress-induced operon. We hypothesized that long-term treatment with aspirin maydecrease the frequency of S aureus bacteremia in such patients. Methods: We retrospectively analyzed electronic medical records for a variety of clinical parameters,
including catheter dwell times, blood culture results, and aspirin use in our dialysis population. Results: A total of 4,722 blood cultures were performed in 872 patients during more than 476
patient-catheter-years. There was a lower rate of catheter-associated S aureus bacteremia in patientstreated with aspirin versus those not treated with aspirin (0.17 versus 0.34 events/patient-catheter-year,P ϭ 0.003), whereas no such difference was observed for other bacteria. This association was dosedependent, seen mostly with the 325-mg aspirin dose. Using the Cox proportional hazard method, riskto develop a first episode of S aureus bacteremia decreased by 54% in patients using aspirin(confidence interval, 24 to 72; P ϭ 0.002). Aspirin was associated with decreased risk of: (1) a firstepisode of methicillin-resistant S aureus bacteremia and (2) metastatic complications during the firstepisode of catheter-related S aureus bacteremia. Conclusion: These data are consistent with our clinical hypothesis that aspirin has a clinically useful
antistaphylococcal effect in the dialysis population. Am J Kidney Dis 49:401-408. 2007 by the National Kidney Foundation, Inc.INDEX WORDS: Hemodialysis; tunneled catheter; catheter infection; catheter sepsis; bacteremia; Staphylococcus aureus; methicillin-resistant Staphylococcus aureus; aspirin; salicylic acid. Theincidenceofbacteremiahasincreasedin lococcal effects mediated by salicylic acid, its
major biometabolite. Salicylic acid inhibits the
of increased rates of serious Staphylococcus
expression of 2 key S aureus virulence genes
aureus infection in this Long-term
involved in endovascular pathogenesis (␣-toxin
hemodialysis patients experience an annual inci-
[hla] and fibronectin-binding adhesin [fnbA])
dence of S aureus bacteremia of 3% to Useof tunneled dialysis catheters is a major riskfactor for developing such blood-borne infec-
From the 1Dartmouth-Hitchcock Medical Center, 2Dart-
tions in hemodialysis patients. Despite Kidney
mouth School of Medicine, Lebanon, NH; 3UCLA School of
Disease Outcomes Quality Initiative (KDOQI)
Medicine; and 4Harbor-UCLA Medical Center, Torrance,
clinical practice guidelines recommending the use
Received June 21, 2006; accepted in revised form Decem-
of permanent vascular access for dialysis, the preva-
lence of hemodialysis catheter use in the United
Originally published online as doi:10.1053/j.ajkd.2006.12.014
States is increasing and approaching 30% of all
Support: A.S.B. is supported by NIH grant AI-39108, andA.L.C. is supported by NIH grant AI-37142. Potential con-
increasing antibiotic resistance patterns among
S aureus strains, new approaches for the preven-
Address reprint requests to Martin Sedlacek, MD, Divi-
tion and treatment of catheter-related S aureussion of Nephrology, Dartmouth-Hitchcock Medical Center,One Medical Center Dr, Lebanon, NH 03756-0001. E-mail:martin.sedlacek@hitchcock.org
In vitro investigations, as well as in vivo
2007 by the National Kidney Foundation, Inc.
studies of experimental infective endocarditis in
rabbits, showed that aspirin has direct antistaphy-
American Journal of Kidney Diseases, Vol 49, No 3 (March), 2007: pp 401-408
through activation of genetic pathways involving
4. Medication use, including aspirin, was determined by
the major stress response operon, sigma factor
reviewing computerized medication lists, office notes,
These aspirin-mediated effects on sigma factor
admission notes, and discharge summaries. The focusof our study was treatment with aspirin and other
B were observed at concentrations normally
medications during the events leading to catheter
achieved by standard clinical dosages of aspirin
failure, which we arbitrarily defined as treatment for
a minimum of 4 weeks before catheter removal.
role in S aureus virulence by facilitating the
Outpatient medication lists for long-term dialysis
attachment and propagation of S aureus within
patients were updated routinely on a monthly basisper unit policy. Omission of a medication from a
the vascular system, we hypothesized that aspi-
medication list was not counted as a discontinuation
rin may be effective clinically in decreasing the
unless clearly documented in a physician’s note.
incidence of S aureus bacteremia in such high-
Because the pharmacological effects of aspirin in the
risk patient groups as hemodialysis patients with
body may last for weeks, we considered discontinua-
tion of aspirin treatment only if it was documented tohave occurred at least 4 weeks before catheter removal. Data were organized into aspirin-treated and non–
aspirin-treated groups. The aspirin group was subdi-
We retrospectively studied all patients who underwent
vided further into an 81-mg/d and 325-mg/d category
hemodialysis at our main dialysis unit and a satellite dialysis
according to the most common dosage used in the
unit during a 10-year period from 1995 to 2005. Our hospital
is a tertiary-care medical center offering dialysis in northern
5. Patient demographic data and medical diagnoses
New Hampshire and eastern Vermont, serving a population
obtained from discharge summaries, admission notes,
of about 400,000 people. The medical center uses a propri-
and office notes. The same data sources were used to
etary central electronic record system for medical records
determine the incidence of metastatic infections as
and billing. This system contains the complete records of all
endocarditis, osteomyelitis, and septic arthritis in
radiological and surgical procedures; all laboratory, pathol-
patients with S aureus bacteremia.
ogy, and microbiology data, including data from our dialysis
Catheter-associated bacteremia was defined as 1 or more
unit; and office and admission notes, discharge summaries,
positive blood culture result in a patient with a tunneled
and medication lists. All patients who were dialyzed through
catheter. Because other sources of infection or contamina-
a tunneled catheter during the study period were included in
tion could not be excluded in retrospect, all blood culture
our investigation. All tunneled catheters were placed by the
results obtained in the presence of a tunneled catheter were
interventional radiology service at our main hospital using
included in our study. Blood cultures obtained after catheter
standard aseptic protocols, and nearly all catheter removals
removal were excluded. We did not require evidence of
were performed by the same service. Temporary catheters
catheter tunnel infection (eg, purulent drainage and ery-
were excluded because of the high variability in circum-
thema of the access site), although this frequently was
stances of placement, greater risk of infection, and difficulty
present. A subsequent episode of bacteremia was considered
tracking them. For patients with tunneled catheters, no
a new event only if the first catheter had been removed and
difference was made between “acute” and “chronic” dialysis
replaced by a new catheter in the interim (tunneled catheters
because this distinction often is arbitrary, depending mainly
that are a suspected source of bacteremia usually are re-
on administrative factors, and is determined in part by
moved in our practice, and negative culture results usually
patient survival from catheter infection.
are required before a new tunneled catheter is placed).
We collected the following data from the electronic medi-
Repeated events in the same patient were included for the
purpose of estimating overall rates of catheter-associated
1. Dates of catheter insertion and removal, from which
bacteremia, but were excluded in multiple logistic regres-
catheter dwell times were calculated.
sion and Cox proportional hazard analyses. We used the
2. Reason(s) for catheter removal (obtained from radiol-
latter statistical methods to estimate overall and time-
dependent risks of a patient to develop the first episode of
3. Results of all blood cultures performed in patients
catheter-associated S aureus bacteremia. The interval be-
with a tunneled catheter in place. All data were
tween catheter insertion and removal constituted the fol-
obtained from the electronic medical record system
low-up interval. The end point for the analysis was catheter
with 1 exception: blood cultures from our satellite
removal associated with S aureus–positive blood culture
dialysis unit in another hospital were processed at the
results. Censoring events were catheter removal for any
local in-house microbiology laboratory, and results
other reason, not related to S aureus bacteremia. Poisson
were obtained by review of hard copy dialysis charts.
regression with log link was used to compare infection rates.
Catheter tip cultures were collected separately when
Fisher exact test and unpaired Student t-test were used as
available. Blood cultures were performed when the
appropriate to compare clinical parameters of the aspirin-
usual signs and symptoms suggestive of infection
treated and non–aspirin-treated groups. Statistical signifi-
were present. The number of blood cultures obtained
cance was defined as P less than 0.05. Statistical analysis
was performed using Statview 5.0.1 and JMP 6.0.3 software
Aspirin and Staphylococcus aureus Bacteremia
(both from SAS Institute, Cary, NC). This retrospective
infections and repeated episodes. Gram-positive
study was approved by our local institutional review board
bacteria accounted for the majority of bacteremic
committee for the protection of human subjects.
episodes, with staphylococci the most common
pathogens isolated from blood cultures. There wasa significantly lower rate of catheter-associated
We identified 872 patients during the 10-year
study period with a total of 1,853 tunneled cath-
bacteremia in patients using aspirin (0.17
eters placed and who accumulated more than 476
versus 0.34 events/patient-catheter-year in non–
patient-catheter-years. During this time, 4,722 blood
aspirin-treated patients; P ϭ 0.003). No such differ-
cultures were performed. The overall incidence of
ence was observed for other bacterial isolates, in-
bacteremia was 7.2 episodes/100 patient-catheter-
cluding coagulase-negative staphylococci. When
months, with an incidence of S aureus bacteremia
all positive blood culture results were considered,
of 2.1/100 patient-catheter-months and an inci-
no statistically significant difference between pa-
dence of S aureus endocarditis of 0.16/100 patient-
tients receiving or not receiving aspirin was found.
catheter-months. The principal reason for catheter
In addition to blood cultures, 369 catheter tip
removal was suspected infection (19%), followed
cultures were performed, 53 of which grew
by poor catheter blood flow (14%) and presence of
S aureus. If positive catheter tip culture results
a mature permanent vascular access (14%). Other
were considered as indirect evidence for S aureus
reasons for catheter removal included patient death,
bacteremia and added together with bona fide
transplantation, change to peritoneal dialysis
blood cultures, the result was statistically more
therapy, recovery of renal function (5%), inadver-
significant: 83 instances of S aureus bacteremia
tent removal, puncture, fracture, uncontrollable
(0.36 event/patient-catheter-year) were observed
bleeding after insertion, and manufacturer recall.
in the non–aspirin-treated group versus 45 (0.18
Of note, the fate of only 8 of 1,853 tunneled
event/patient-catheter-year) in the aspirin-treated
catheters (Ͻ0.5%) remained unaccounted for.
lists unselected microbiological data for
If repeated episodes of S aureus bacteremia in
the 10-year study period that include polymicrobial
the same patient were excluded, the difference
Table 1. Number of Episodes and Rates of Catheter-Associated Bacteremia in a 10-Year Period From 1995 to 2005 Note: Multiple bacterial isolates and repeated episodes were included in this table. Fungal isolates and bacterial species
found fewer than 5 times during the 10-year study period were omitted.
*Significant difference by Poisson regression. Table 2. Association Between Aspirin Dose and Rates of Catheter-Associated S aureus and MRSA Bacteremia
ءSignificant difference by Poisson regression.
was even more significant: 64 first episodes ofS aureus bacteremia (0.57 event/patient-catheter-year) in patients not administered aspirin versus
Table 3. Patient Characteristics and Distribution of
28 first episodes (0.23 event/patient-catheter-
Covariates for the Cox Proportional Hazard Analysis
year) in patients treated with aspirin (P Ͻ 0.001).
We further examined the association between
aspirin dosage and rate of S aureus bacteremiaThe lowest rate of S aureus bacteremia
was found in patients treated with the 325-mg
dose. Comparing only patients administered 81
mg of aspirin versus patients not administered
aspirin, the difference in rates of S aureus bacte-
remia was not statistically significant (0.22 ver-
sus 0.34 event/patient-catheter-year; P ϭ 0.26).
Catheter-associated bacteremia with methicillin-
resistant S aureus (MRSA) occurred less fre-
quently than with methicillin-sensitive S aureus.
However, the 325-mg dose of aspirin was associ-
ated with a lower number of catheter-associated
MRSA bacteremia than the 81-mg dose because
during the 10-year study period, only 1 such
lences of different risk factors for patients in the
aspirin-treated and non–aspirin-treated groups.
As anticipated, coronary artery disease, periph-
eral vascular disease, history of stroke, hyperten-
sion, and diabetes mellitus were more prevalent
Note: Values expressed as mean Ϯ SD or number
in patients treated with aspirin, who were on
average 10 years older than patients not treated
Abbreviations: ACE, angiotensin-converting enzyme;
*Statistically significant difference between aspirin-
Using Cox proportional hazard analysis, we stud-
treated and non–aspirin-treated groups by means of Fisher
ied risk factors for developing a first episode of
exact test or unpaired Student t-test, as appropriate. Aspirin and Staphylococcus aureus BacteremiaTable 4. Risk of a First S aureus Bacteremia Episode
statistically significant effect was found with the
in 872 Dialysis Patients With a Tunneled Catheter by
81-mg dose. Using multiple logistic regression
Using Cox Proportional Hazard Analysis
analysis, risk of S aureus bacteremia signifi-
cantly increased in patients with diabetes melli-
tus (relative risk, 2.2; CI, 1.3 to 3.6; P ϭ 0.002)and decreased by the presence of COPD (relative
contrary to results of the Cox analysis, warfarin
had no significant impact. Aspirin decreased the
risk of developing a first episode of MRSA
bacteremia by 65% (CI, 9 to 87; P ϭ 0.03). The
risk of developing metastatic infection with a
first episode of S aureus bacteremia decreased by
an estimated 78% in patients treated with aspirin,
although the CI was very large (3 events with
aspirin versus 11 events without aspirin; CI, 7 to
tunneled catheters associated with S aureus
bacteremia, obtained using the Kaplan-Meier
method. Grouping by aspirin treatment resulted
in 2 divergent graphs, with the risk of catheter
failure caused by S aureus infection significantlyincreased in the non–aspirin-treated group (P Ͻ
Abbreviations: ACE, angiotensin-converting enzyme;
*Statistical significance in Cox proportional hazard model. DISCUSSION
catheter-associated S aureus bacteremia
Our data constitutes one of the largest studies
The presence of diabetes mellitus increased the
of dialysis catheter–associated bacteremia. The
odds, whereas the presence of chronic obstruc-
incidence of catheter-related bacteremia in our
tive pulmonary disease (COPD) decreased the
population is within the previously reported range
odds of developing a first episode of S aureus
bacteremia. Aspirin was statistically the most
Incidences of S aureus bacteremia and S aureus
significant factor and decreased the odds of devel-
endocarditis in our population are similar to
oping a first episode of S aureus bacteremia by
54% (confidence interval [CI], 72 to 24; P ϭ
tip cultures and differential central and peripheral-
0.002). No other cardiovascular medication in
blood cultures were not performed systemati-
our analysis had a significant effect. Interest-
cally, our study definition of catheter-associated
ingly, the risk of a first episode of S aureus
bacteremia is not identical to the definition of the
bacteremia increased in patients treated with
Hospital Infection Control Practices Advisory
warfarin, while being unaffected by treatment
a peripheral-blood culture, which is the focus of
Multiple logistic regression analysis yielded a
our study, is particularly likely to be associated
similar result: risk of ever developing a first
with a catheter-related blood-borne infection in
episode of catheter-associated S aureus bactere-
mia decreased by 60% in patients using aspirin
tured from the tip of a suspect catheter only, but
(CI, 75 to 33; P Ͻ 0.001). In addition, stratifica-
blood cultures either were not obtained or re-
tion of the analysis according to different aspirin
mained negative, the risk of S aureus bacteremia
doses confirmed that the decreased odds to develop
is very high and treatment often is recom-
S aureus bacteremia was associated mainly with
use of the 325-mg dose of aspirin, whereas no
tip cultures in a separate analysis. Because inclu-
Figure 1.
of tunneled catheter failureassociated with S aureus bac-teremia. The failure plot wasobtained using the Kaplan-Meier method. Tics representcensoring of catheter removalunrelated to S aureus bactere-mia. Log-rank test was used tocalculate P.
sion of patients with multiple episodes of bacte-
disease, thus not allowing to assess for changes
remia is a potential source of bias, we performed
data analysis considering only first episodes of
In our study, no difference in number of epi-
sodes of bacteremia was found with pathogens
The principal result of our study is that treat-
other than S aureus, particularly coagulase-
ment with a daily 325-mg dose of aspirin is
negative staphylococci. This observation is con-
associated with significantly less S aureus bacte-
sistent with the putative importance of down-
remia in at-risk patients with tunneled dialysis
modulation of ␣-toxin production by aspirin in
catheters. Of particular importance, we observed
its protective effects because coagulase-negative
a similar association with MRSA, a notoriously
staphylococci possess a sigma factor B operon,
difficult-to-treat subgroup of S aureus infection.
but no ␣-toxin homologue. Consistent with the
Aspirin dosage appeared to be pivotal because
notion that the putative antistaphylococcal ef-
the statistical effect derived only from the 325-mg
fects of aspirin are not related to its antiplatelet
regimen, whereas the 81-mg “baby aspirin” dose
properties are: (1) the 325-mg, but not the 81-
mg, dose was associated with decreased risk of
Although the antistaphylococcal effects of as-
S aureus bacteremia, although both these dose
pirin were studied extensively in the laboratory
regimens exert equivalent antiplatelet ef
setting, there exists little prior clinical data to
(2) the antiplatelet agent clopidrogel was not
such effects in humans. A study of embolic
protective; and (3) prior studies confirmed the
complications of patients with endocarditis found
antistaphylococcal effects of salicylic acid itself,
a decreased rate of embolic events in patients
with native valve infections who were on long-
Colonization is the initiating event of catheter-
term aspirin treatment (11% versus 47%), al-
associated Nasal carriage of S au-
though the numbers were too small to be conclu-
reus is recognized as an endogenous source for
initiating bacteremic infection,and it is known
infective endocarditis with aspirin was found to
from prospective studies that the interval be-
be beneficial in 1 study involving 9 patients,
tween catheter placement and staphylococcemia
but this result was not confirmed in a randomized
can be very short, with 23% of episodes of
trial by Chan et Of note, only 25% to 30%
catheter-related bacteremia occurring less than
of patients in this trial had a S aureus infection
and aspirin was added to already established
conceivable that aspirin decreases colonization
Aspirin and Staphylococcus aureus Bacteremia
vitro studies of aspirin did not show either a
measure of the putative prophylactic benefit of
growth-inhibitory or bactericidal impact at
aspirin against S aureus bacteremia: delayed on-
Therefore, it seems unlikely that rapidly develop-
Diabetes mellitus previously was recognized
ing resistance to aspirin’s antimicrobial effects will
as a risk factor for S aureus bacteremia in dialysis
occur in the future. Our findings strongly support
patients, also confirmed in our studyA potential
the need for a prospective analysis of aspirin treat-
explanation for the reduced risk of catheter-
ment in hemodialysis patients and other popula-
associated S aureus bacteremia in patients with
tions at increased risk of staphylococcemia.
COPD could be more frequent antibiotic use andhence decreased S aureus carriage in this patient
REFERENCES
group. A greater incidence of S aureus bactere-
1. Foley RN, Guo H, Snyder JJ, Gilbertson DT, Collins
mia was reported in patients with cardiovascular
AJ: Septicemia in the United States dialysis population,1991 to 1999. J Am Soc Nephrol 15:1038-1045, 2004
2. Kessler M, Hoen B, Mayeux D, Hestin D, Fontenaille
numbers of bacteremia in this patient group
C: Bacteremia in patients on chronic hemodialysis: A multi-
treated with aspirin, emphasizes the potential
center prospective survey. Nephron 64:95-100, 1992
clinical importance of its antistaphylococcal ef-
3. Rayner HC, Besarab A, Brown W, Disney A, Saito A,
fects. In addition, aspirin is recommended for
Pisoni RL: Vascular access results from the Dialysis Out-comes and Practice Patterns Study (DOPPS): Performance
dialysis patients by the 2005 KDOQI guidelines
against Kidney Disease Outcomes Quality Initiative (K/
because of its beneficial cardiovascular ef
DOQI) Clinical Practice Guidelines. Am J Kidney Dis
A major limitation of our study resides in its
retrospective and observational nature, with the
4. Leeb M: A shot in the arm. Nature 431:892-893,
impossibility to eliminate bias resulting from
5. Kupferwasser LI, Yeaman MR, Nast CC, et al: Sali-
changes in practice patterns. However, we be-
cylic acid attenuates virulence in endovascular infections by
lieve our data to be robust because a single
targeting global regulatory pathways in Staphylococcus
geographic area with no competing dialysis cen-
aureus. J Clin Invest 112:222-233, 2003
ter was queried, a centralized electronic medical
6. Needs CJ, Brooks PM: Clinical pharmacokinetics of
record system was used, and close to 100%
the salicylates. Clin Pharmacokinet 10:164-177, 1985
7. Doulton T, Sabharwal N, Cairns H, et al: Infective
catheter follow-up was achieved. In addition, the
endocarditis in dialysis patients: New challenges and old.
number of observations was large. The design of
our study with inclusion of all blood cultures in
8. Marr KA, Sexton DJ, Conlon PJ, Corey GR, Schwab
all patients with tunneled catheters minimized
SJ, Kirkland KB: Catheter-related bacteremia and outcome
selection bias. Potential noncompliance with daily
of attempted catheter salvage in patients undergoing hemodi-alysis. Ann Intern Med 127:275-280, 1997
aspirin treatment regimens raises the possibility
9. Hoen B: Infective endocarditis: A frequent disease in
of misclassifications of patients between the non–
dialysis patients. Nephrol Dial Transplant 19:1360-1362,
aspirin-treated versus aspirin-treated groups.
Thus, our study may still have underestimated
10. Mermel LA, Farr BM, Sherertz RJ, et al: Guidelines
the clinical antistaphylococcal effect of aspirin in
for the management of intravascular catheter-related infec-tions. Clin Infect Dis 32:1249-1272, 2001
11. Gosbell IB: Diagnosis and management of catheter-
related bloodstream infections due to Staphylococcus aureus.
than 100 years, is widely used, and is available
without prescription. Conversely, conven-
12. Peacock SJ, Eddleston M, Emptage A, King A, Crook
tional antibiotics have been available for only
DW: Positive intravenous line tip cultures as predictors ofbacteremia. J Hosp Infect 40:35-38, 1998
much shorter periods, require prescription for
13. Schunemann S, Werner GS, Schulz R, Bitsch A,
use, and were associated with relatively rapid
Prange HW, Kreuzer H: Embolische Komplikationen bei
development of bacterial resistance. That we
bakterieller Endokarditis. Z Kardiol 86:1017-1025, 1997
still observe an impressive negative associa-
14. Taha TH, Durrant SS, Mazeika PK, Nihoyannopoulos
tion of aspirin treatment with S aureus bactere-
P, Oakley CM: Aspirin to prevent growth of vegetations andcerebral emboli in infective endocarditis. J Intern Med
mia in at-risk patients may be testimony to the
mechanism of action of this agent being differ-
15. Chan K-L, Dumesnil JG, Cujec B, et al: A random-
ent from traditional antibiotics. Of note, in
ized trial of aspirin on the risk of embolic events in patients
with infective endocarditis. J Am Coll Cardiol 42:775-780,
19. Breen JD, Karchmer AW: Staphylococcus aureus
infections in diabetic patients. Infect Dis Clin North Am
16. Patrono C, Coller B, FitzGerald GA, Hirsh J, Roth G:
Platelet-active drugs: The relationships among dose, effec-
tiveness, and side effects. The Seventh ACCP Conference on
ical Practice Guidelines for Cardiovascular Disease in
Antithrombotic and Thromboltic Therapy. Chest 126:S234-
Dialysis Patients. Am J Kidney Dis 45:S1-S153, 2005
17. Kluytmans JAJW, Wertheim HFL: Nasal carriage of
21. Kupferwasser LI, Yeaman MR, Shapiro SM, et al:
Staphylococcus aureus and prevention of nosocomial infec-
Acetylsalicylic acid reduces vegetation bacterial den-
sity, hematogenous bacterial dissemination, and fre-
18. Little MA, O’Riordan A, Lucey B, et al: A prospective
quency of embolic events in experimental staphylococcus
study of complications associated with cuffed, tunneled haemo-
aureus endocarditis through antiplatelet and anti-
dialysis catheters. Nephrol Dial Transplant 16:2194-2200, 2001
bacterial effects. Circulation 99:2791-2797, 1999
Cervicogenic headaches: a critical reviewScott Haldeman, DC, MD, PhDa*, Simon Dagenais, DCba Department of Neurology, University of California, Irvine, Medical Center, 101 The City Drive South, Orange, CA 92868, USA b Research Division, Southern California University of Health Sciences, 16200 East Amber Valley Drive, Whittier, CA 90609-1166 Received December 22, 2000; revised January 8, 20
Warning the public about medical murder and the organ trade in Canada Marked for Murder at the University Health Network (Toronto) Organs cannot be “donated” in situations of entrapment. Those fully conscious patients who realize they have been kidnapped by a hospital never agree to their predicaments. Instead they desperately try to escape. Likewise, no one in a coma ever signs his
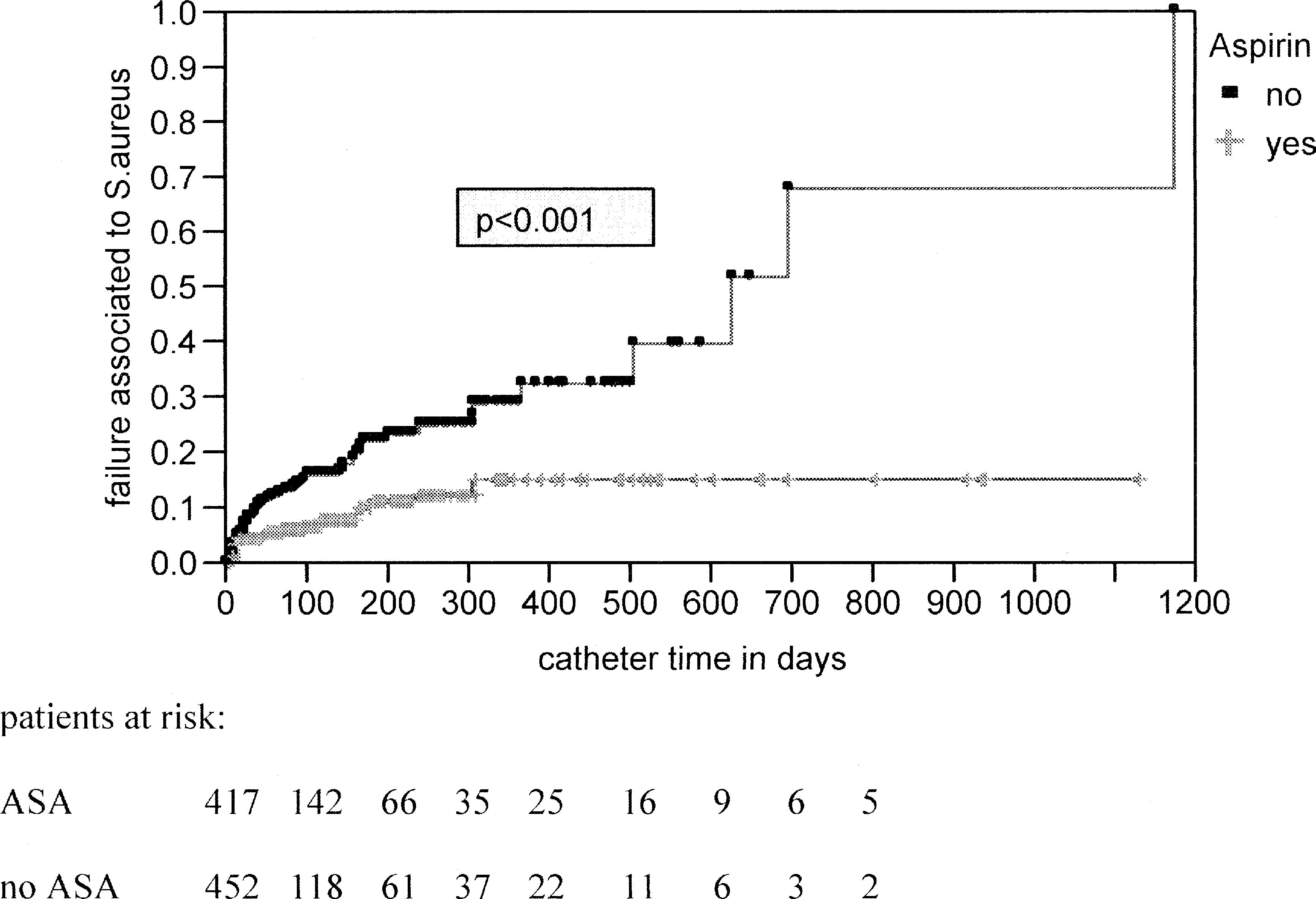 Figure 1.
Figure 1.