Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
Caahs.com.ar
Open tension-free Lichtenstein repair of inguinal hernia:use of fibrin glue versus sutures for mesh fixation
P. Negro • F. Basile • A. Brescia • G. M. Buonanno • G. Campanelli • S. Canonico •M. Cavalli • G. Corrado • G. Coscarella • N. Di Lorenzo • E. Falletto • L. Fei •M. Francucci • C. Fronticelli Baldelli • A. L. Gaspari • E. Gianetta • A. Marvaso •P. Palumbo • N. Pellegrino • R. Piazzai • P. F. Salvi • C. Stabilini • G. Zanghı`
Received: 4 December 2009 / Accepted: 11 July 2010 / Published online: 30 July 2010Ó Springer-Verlag 2010
intensity was assessed by a visual analog scale (VAS; 0 [no
To investigate pain and other complications
following inguinal hernioplasty performed by the Lich-
One hundred and seventy-one patients received
tenstein technique with mesh fixation by fibrin glue or
sutures and 349 received fibrin glue. During the early
postoperative phase, 87.4% of patients in the fibrin glue
Five hundred and twenty patients were enrolled
group and 76.6% of patients in the sutures group were
in this 12-month observational multicenter study and
complication-free (P = 0.001). Patients who received
received either sutures or fibrin glue (TissucolÒ/TisseelÒ)
fibrin glue were also less likely to experience hematoma/
based on the preference of the surgeon. Pain, numbness,
discomfort, recurrence, and other complications were
P = 0.001). The mean pain score was significantly lower
assessed postoperatively and at 1, 3, 6, and 12 months. Pain
in the fibrin group than the sutures group (2.5 vs. 3.2,
Azienda Ospedaliera Universita` degli Studi di Roma
Azienda Ospedaliera, Universitaria San Giovanni Battista,
Azienda Ospedaliera Vittorio Emanuele, Catania, Italy
Azienda Ospedaliera Santa Maria, Terni, Italy
Azienda Ospedaliera San Andrea, Rome, Italy
Azienda Ospedaliera Universita` San Martino di Genova,Genoa, Italy
G. M. BuonannoAzienda Ospedaliera San Giuseppe Moscati, Avellino, Italy
A. MarvasoP.O.S. Anna Rizzoli, A.S.L. Napoli 2, Lacco Ameno, Italy
G. Campanelli Á M. CavalliUniversita` dell’Insubria di Varese, I.R.C.C.S. Multimedica,
Ospedale Generale di Zona San Giuseppe Sambiasi, Nardo, Italy
Seconda Universita` degli Studi di Napoli, Naples, Italy
Ospedale Santi Carlo e Donnino, Pergola, Italy
P.O. Unico Villa Malta, A.S.L. Salerno, Sarno, Italy
A.O. Policlinico Umberto, Viale del Policlinico, 190,00133 Rome, Italy
G. Coscarella Á N. Di Lorenzo Á A. L. Gaspari
Dipartimento di Scienze Chirurgiche,Universita` di Roma Tor Vergata, Rome, Italy
P \ 0.001). At 1 month, significantly fewer patients in the
with TissucolÒ/TisseelÒ fibrin glue (Baxter Healthcare,
fibrin glue group reported pain, numbness, and discomfort
Deerfield, IL, USA) as a means of mesh fixation in hernia
compared with patients in the sutures group (all P \ 0.05).
repair have shown promising results [, –,
Fibrin glue patients also experienced less intense pain (0.6
The Lichtenstein technique is a standard procedure for
vs. 1.2; P = 0.001). By 3 months, the between-group dif-
open tension-free inguinal hernia repair performed using
ferences had disappeared, except for numbness, which was
prosthetic meshes to strengthen the inguinal canal posterior
more prevalent in the sutures group. By 12 months, very
wall Postoperative quality of life and the rate of
few patients reported complications.
postoperative complications are dependent on the type of
Tissucol fibrin glue for mesh fixation in the
mesh and method of fixation [, as well as metic-
Lichtenstein repair of inguinal hernia shows advantages
ulous surgical technique. Importantly, hernia can recur
over sutures, including lower incidence of complications
with the Lichtenstein technique if mesh overlap around the
such as pain, numbness, and discomfort, and should be
hernia orifice is inadequate [Therefore, high-quality
considered as a first-line option for mesh fixation in
fixation methods should be used to properly secure the
mesh until it is incorporated into the patient’s own tissue. The purpose of our study was to investigate the frequency
Inguinal hernia Á Tension-free hernia repair Á
and severity of postoperative pain and other complications
Human fibrin glue Á Tissucol/Tisseel Á Mesh fixation Á
when prosthetic mesh is fixed by using fibrin glue com-
pared with conventional sutures in inguinal hernioplastyperformed by the Lichtenstein technique.
The increasing use of mesh procedures in inguinal herniasurgery has led to a substantial decrease in the incidence of
hernia recurrence. As a result, surgeons (and, increasingly,their patients) are now focused on other measures reflecting
This was a prospective observational study carried out in
the success of hernia repair. The prevalence of postopera-
16 centers across Italy with extensive experience in hernia
tive pain syndromes after open and laparoscopic proce-
surgery. Male or female patients aged over 18 years of age
dures has been reported to be as high as 30% and some
with a primary unilateral uncomplicated inguinal hernia
analyses estimate that 12% of patients feel themselves
suitable for Lichtenstein repair were eligible for enrolment.
to be restricted in their daily activities because of pain.
Exclusion criteria included femoral or incarcerated hernia,
Clinical studies have shown that both recurrence and
the need for other abdominal procedure, body mass index
chronic pain after endoscopic hernia repair are influenced
(BMI) C 35 kg/m2, diabetes, immunological or coagula-
by the type of mesh implanted and its method of fixation
tion disorders, warfarin or clopidogrel therapy, steroid
[–]. The ideal mesh fixation should produce no structural
therapy for long-term pain control, hypersensitivity to
damage and be biocompatible in order to reduce the risk of
aprotinin, history of drug/alcohol abuse, and psychiatric
hematoma and seroma Conventionally, the mesh
disorders. Patients received either sutures or fibrin glue for
prosthesis is secured by either sutures or staples. Despite
mesh fixation based on the preference of the operating
the ‘‘tension-free’’ nature of these hernioplasties, sutures
and staples may strangulate muscle fibers, compress
Ethics committee approvals were obtained from the
regional nerves, or give rise to a lesion, leading to inca-
participating institutions and informed consent was sought
Complications associated with sutured mesh fixation
following open groin hernia repair have prompted surgeons
to evaluate methods of atraumatic fixation, such as the useof human fibrin glue. Fibrin glue is a biodegradable
adhesive combining human-derived fibrinogen and throm-bin that replicates the last step of the coagulation cascade.
A polypropylene mesh was trimmed to fit the floor of the
It has been used in a variety of surgical fields for its
inguinal canal, and its apex was sutured to the pubic
effectiveness, excellent local tolerability, and relative lack
tubercle using a No. 3–0 Prolene suture. The same con-
of adverse effects and contraindications. Its adhesive and
tinuous suture was used to join the lower border of the
hemostatic properties have been demonstrated in a number
mesh to the free edge of the inguinal ligament, after an
of experimental studies and clinical trials []. Studies
opening was made into its lower edge to accommodate the
spermatic cord. The continuous suture was extended up just
520 patients, with the fixation of mesh achieved with either
medial to the anterior superior iliac spine. Interrupted
fibrin glue (349 patients) or sutures (171 patients). Baseline
Prolene sutures were used to suture the two cut edges of the
demographic and clinical characteristics were similar
mesh together around the spermatic cord. The inferomedial
between the treatment groups (Table Our study inclu-
corner of the mesh was attached, overlapping the pubic
ded 484 (93%) male and 36 (7%) female patients with a
tubercle. The mesh was anchored to the conjoined tendon
mean age of 55 years (range 18–90); 70% of patients were
by interrupted sutures (Prolene 3–0). The external oblique
workers or active pensioners. The mean (±SD) VAS pain
aponeurosis was closed using absorbable sutures (Vicryl
intensity score in the preoperative phase was 2.9 (±2.0),
with no significant difference between the study groups.
In 288 (55%) of patients, inguinal hernias were right-
sided, 223 (43%) had left-sided hernias, and 9 (2%) hadbilateral hernias, giving a total of 529 hernias. At surgery,
Fibrin glue alone was sufficient for polypropylene mesh
hernias were classified according to the European Hernia
fixation, without the need for additional sutures. Fibrin glue
Society (EHS) criteria ]: 164 (32%) were L1, 191 (37%)
was applied using either a needle or a spray applicator.
L2, 5 (1%) L3, 65 (13%) M1, 100 (19%) M2, and 3 (1%)
Surgeons were permitted to use either application method,
Of the 520 patients, 470 (90%) completed follow-up
visits at 1, 3, 6, and 12 months. Fifty patients discontinued
the study, 33/349 (9%) from the fibrin glue group and 17/171 (10%) from the sutures group. Of these 50 patients, 24
The prevalence of inguinal pain, numbness, and discomfort
did not attend follow-up visits, one withdrew due to
were assessed at hospital discharge until 1 month post-
adverse events, one died (cardiac arrest), and 24 discon-
surgery (to determine early postoperative outcomes) and at
1-, 3-, 6-, and 12-month follow-up visits (to determine themedium- to long-term outcomes) via structured interviews
with clinical report forms. A visual analog scale (VAS) wasused to gauge patient pain intensity, ranging from 0 = no
Surgery parameters were similar between the treatment
pain to 10 = worst pain. Recurrence due to technical
groups, with the exception of the mean operating time,
errors, hematoma, ecchymosis, other complications (e.g.,
which was significantly shorter in patients receiving fibrin
seroma, infection), use of analgesia and antibiotics, and
glue compared with those receiving sutures (55.6 vs.
time to return to normal activity were assessed. The eval-
61.2 min, P \ 0.001) (Table ). Fibrin glue was applied
uators were not blinded to treatment. At the time of oper-
using a needle in 52% of patients and a spray device in
ation, surgeons assessed the ease of use of fibrin glue
46% of patients (data missing for 2% of patients). In the
application through a score ranging from 1 = very easy to
fibrin glue group, 67% of patients received 1 mL glue, 23%
received 2 mL, and 6% received 5 mL (data missing for4% of patients). The mean VAS score for the ease of fibrin
glue application was 1.8 ± 0.8, indicating a high level ofease among surgeons when using Tissucol.
Descriptive statistics were calculated. Differences betweenthe study groups in terms of the proportions experiencing
postoperative pain, numbness, discomfort, and recurrencedue to technical errors were analyzed by the Chi-squared
During the early postoperative phase (at hospital discharge
test. Continuous variables such as pain intensity and time
until 1 month postsurgery), 305/349 (87.4%) of patients in
to return to normal activity were analyzed by the Mann–
the fibrin glue group and 131/171 (76.6%) of patients in the
sutures group were free of complications (P = 0.001;Table Patients in the fibrin glue group were also lesslikely to experience hematoma (1.7 vs. 8.2%) and ecchy-
mosis (8.6 vs. 15.2%) than patients in the sutures group(both P = 0.001).
The mean VAS score for the intensity of pain reported
by patients was significantly lower in the fibrin group
Operations took place from January 2007 to January 2008.
compared with the sutures group (2.5 vs. 3.2, P \ 0.001).
Tension-free repair of inguinal hernia was performed in
The use of analgesics in the postoperative period was
COPD chronic obstructivepulmonary disease; VAS visual
similar between groups, with around 64% requiring pain
two cases of direct hernias in the fibrin group at the 3-
month assessment. In both cases, the fibrin glue had been
Fewer patients in the fibrin glue group reported numb-
sprayed and recurrence was attributed to procedural errors,
ness than in the sutures group (12.3 vs. 23.4%, P = 0.003).
i.e., inadequate size of the polypropylene mesh.
Discomfort was reported in 46.5% of patients, with no
Figure summarizes the percentage of patients who
differences evident between groups. Six complications
were suffering from numbness before and after surgery. At
occurred: two fever cases (one in each study group), two
1 month, significantly fewer patients in the fibrin glue
scrotal hematoma cases (one in each study group), one
group reported pain, numbness, and discomfort compared
seroma (sutures group), and one case of abdominal pain
with patients in the sutures group (all P \ 0.05; Table ;
(fibrin glue group). More patients in the sutures group
Fig. ). The fibrin glue group patients also experienced less
received antibiotics than in the fibrin glue group (85.4 vs.
intense pain (mean VAS score 0.6 vs. 1.2; P = 0.001;
65.6%, P \ 0.001). No significant difference between
Fig. ). Fewer than 1% of patients required analgesia. By
groups was noted with regard to the length of hospital stay.
3 months, these between-group differences had disap-peared, with the exception of numbness, which continued
to be more prevalent in the sutures group than in the fibringlue group (13.7 vs. 4.1%, P \ 0.001; Fig. ).
As shown in Table , there were no recurrences due to
The prevalence of complications continued to decrease
technical complications throughout the study, except for
throughout the follow-up period, as expected, with no
Table 3 Postoperative complications at hospital discharge and other variables
Objective examination, no. of patients (%)a
Postoperative hospital stay, mean ± SD (days)
All P-values were derived from Chi-squared testing, except pain intensity, which were derived from Mann–Whitney U testing
SD standard deviation, VAS visual analog scale ranging from 0 (no pain) to 10 (worst pain), NSAIDs non-steroidal anti-inflammatory drugsa Some patients had more than one complication; data were missing for 13 patients
between-group differences evident at 6 and 12 months
continued to be significantly more prevalent in the sutures
follow-up. By 12 months, very few patients in either study
group, but the between-group differences in all of the other
group reported pain, numbness, or discomfort (Table
outcome measures had disappeared. Complications con-tinued to decrease in both study groups throughout the12-month follow-up period, such that only a handful of
This prospective, observational, multicenter study com-
Our findings are largely consistent with the published
pared fibrin glue versus conventional sutures for mesh
studies of Tissucol versus sutures for mesh fixation in
fixation in the Lichtenstein repair of inguinal hernia.
Lichtenstein hernia repair ]. A controlled study by
The mean operating time was reduced by around 9% in
Hidalgo et al. [assessed mesh fixation using fibrin
the fibrin glue study group relative to the sutures group
sealant compared with sutures in 55 patients with bilateral
(P \ 0.001) and the mean VAS score for the ease of fibrin
inguinal hernias, in whom mesh fixation was undertaken
glue application was 1.8 (possible score 1–10, with
with sutures on the right hernia and with glue on the left
10 = most difficult), indicating a high level of ease among
hernia. Similar overall outcomes were reported in both
surgeons when using Tissucol. Patients in the fibrin glue
inguinal regions, but there was less postoperative pain and
group were also less likely to experience early local hem-
less inflammatory reaction associated with fibrin-fixed
orrhagic complications (e.g., hematoma, ecchymosis) than
hernia repairs. Two patients reported pubic pain at
6 months, but were free of pain by 12 months; no other
At 1 month assessment, patients in the fibrin glue study
early or late complications were observed. In an uncon-
group reported significantly less pain, numbness, and dis-
trolled study, Canonico et al. assessed the use of fibrin
comfort compared with patients in the sutures group. There
sealant in 80 patients who had undergone sutureless Lich-
were no differences in the days of sickness absence
tenstein repair of primary unilateral hernia, with Tissucol as
between the two study groups. At 3 months, numbness
a means of mesh fixation. No complications were observed
Table 4 Complications experienced during the 12-month follow-up period
34 (19.9%) 14 (4.1%)*** 23 (13.7%) 10 (3.0%)
All P-values were derived from Chi-squared testing, except pain intensity and days of sickness absence, which were derived from Mann–Whitney U testing
VAS visual analog scale ranging from 0 (no pain) to 10 (worst pain); SD standard deviation
**** P = 0.028 versus sutures group One seroma, one unspecifiedà Two scrotal hematomas, one seroma, one fever, one sporadic dysejaculation
Fig. 1 Percentage of patientssuffering from numbness beforeand after surgery
over 12 months. More definitive conclusions about the
compared the 12-month rate of disabling complications
effectiveness of fibrin glue in reducing the rate of postop-
(chronic pain/numbness/groin discomfort) following mesh
erative complications following Lichtenstein repair comes
fixation with Tissucol or sutures in patients with inguinal
from the TIMELI (TIssucol/TIsseel for MEsh fixation in
hernia undergoing Lichtenstein repair []. At 12 months,
LIchtenstein hernia repair) study. This international, con-
the prevalence of C1 disabling complication was signifi-
trolled, randomized, patient- and evaluator-blinded study
cantly lower in the Tissucol group than in the sutures group
Fig. 2 Pain intensity asassessed by the visual analogscale (VAS) score before andafter surgery
(8.1 vs. 14.8%; P = 0.034) [Less numbness and groin
accompanied by reduction in postoperative inguinal pain.
discomfort were also noted in the Tissucol versus sutures
Consequently, fibrin glue should be considered as a first-
group (P = 0.019; P = 0.049); only 3/316 patients (0.94%)
line option over sutures for mesh fixation in inguinal hernia
experienced recurrence (one Tissucol, two sutures).
The notion that fibrin glue fixation is associated with
less postoperative pain versus suturing is quite conceivable
The authors declare that they have no conflicts
considering the procedural differences between the twoapproaches. Suturing the upper edge of the prosthetic meshto the internal oblique aponeurosis results in markedretraction of the external oblique aponeurosis, subcutane-
ous fat, and skin as the needle passes. In contrast, minimaltissue retraction is necessary with fibrin glue fixation. More
1. Bay-Nielsen M, Perkins FM, Kehlet H (2001) Pain and functional
soft tissue retraction naturally leads to greater contusion
impairment 1 year after inguinal herniorrhaphy: a nationwide
and short-term pain. Therefore, consistent with our results,
less soft tissue contusion and associated postoperative pain
2. Aasvang E, Kehlet H (2005) Surgical management of chronic
pain after inguinal hernia repair. Br J Surg 92:795–801
seems probable with fibrin glue fixation compared with
3. Katkhouda N, Mavor E, Friedlander MH, Mason RJ, Kiyabu M,
Grant SW, Achanta K, Kirkman EL, Narayanan K, Essani R
In terms of study weaknesses, our study was not ran-
(2001) Use of fibrin sealant for prosthetic mesh fixation in lap-
domized or blinded and no formal power calculations were
aroscopic extraperitoneal inguinal hernia repair. Ann Surg233:18–25
undertaken. Patients were allocated to sutures or fibrin glue
4. Junge K, Rosch R, Krones CJ, Klinge U, Mertens PR, Lynen P,
by the operating surgeon as per routine practice; however,
Schumpelick V, Klosterhalfen B (2005) Influence of polygleca-
both study groups were similar in terms of clinical and
prone 25 (Monocryl) supplementation on the biocompatibility of
demographic characteristics at baseline. The relatively
a polypropylene mesh for hernia repair. Hernia 9:212–217
5. Amid PK (1997) Classification of biomaterials and their
small study population limits the generalization of the
related complications in abdominal wall hernia surgery. Hernia
findings, and the 12-month follow-up period is too short to
provide meaningful information on chronic pain or hernia
6. Campanelli G, Champault G, Pascual MH, Hoeferlin A, Kings-
recurrence with mesh fixation by fibrin glue versus sutures.
north A, Rosenberg J, Miserez M (2008) Randomized, controlled,blinded trial of Tissucol/Tisseel for mesh fixation in patients
Nonetheless, in summary, our study suggests that using
undergoing Lichtenstein technique for primary inguinal hernia
fibrin glue to fix mesh in inguinal hernia repair results in
repair: rationale and study design of the TIMELI trial. Hernia
significantly less pain, numbness, and discomfort than
fixation with sutures during the early postoperative period
7. Canonico S, Santoriello A, Campitiello F, Fattopace A, Corte
AD, Sordelli I, Benevento R (2005) Mesh fixation with human
(at hospital discharge until 1 month postsurgery). This is a
fibrin glue (Tissucol) in open tension-free inguinal hernia repair:
period that many would regard as the most critical period in
which patients experience the most negative impact on the
8. Katkhouda N (2004) A new technique for laparoscopic hernia
repair using fibrin sealant. Surg Technol Int 12:120–126
9. Lau H (2005) Fibrin sealant versus mechanical stapling for mesh
Mesh fixation with fibrin glue in open tension-free
fixation during endoscopic extraperitoneal inguinal hernioplasty:
Lichtenstein hernia repair is a simple technique that is
a randomized prospective trial. Ann Surg 242:670–675
10. Alfieri S, Di Miceli D, Doglietto GB (2007) Prophylactic ilioin-
of Tisseel for mesh fixation in patients undergoing Lichtenstein
guinal neurectomy in open inguinal hernia repair. Ann Surg
technique for inguinal hernia repair: the TIMELI trial. Hernia
13(Suppl 1). Abstract presented at the 4th Joint Meeting of the
11. Canonico S (2003) The use of human fibrin glue in the surgical
American Hernia Society (AHS) and the European Society Her-
operations. Acta Biomed 74(Suppl 2):21–25
nia (EHS), Berlin, Germany, 9–12 September 2009
12. Ferna´ndez Lobato R, Garcı´a Septiem J, Ortega Deballon P,
16. Amid PK (2004) Lichtenstein tension-free hernioplasty: its
Martı´n Lucas FJ, Ruı´z de Adana JC, Limones Esteban M (2001)
inception, evolution, and principles. Hernia 8:1–7
Tissucol application in dermolipectomy and incisional hernia
17. Gilbert AI, Graham MF, Voigt WJ (1999) A bilayer patch device
for inguinal hernia repair. Hernia 3:161–166
13. Zieren J, Castenholz E, Baumgart E, Mu¨ller JM (1999) Effects of
18. Miserez M, Alexandre JH, Campanelli G, Corcione F, Cuccurullo
fibrin glue and growth factors released from platelets on
D, Pascual MH, Hoeferlin A, Kingsnorth AN, Mandala V, Palot
abdominal hernia repair with a resorbable PGA mesh: experi-
JP, Schumpelick V, Simmermacher RK, Stoppa R, Flament JB
(2007) The European Hernia Society groin hernia classification:
14. Olmi S, Erba L, Bertolini A, Scaini A, Mastropasqua E, Conti M,
simple and easy to remember. Hernia 11:113–116
Croce E (2005) Use of fibrin glue (Tissucol) for mesh fixation in
19. Hidalgo M, Castillo MJ, Eymar JL, Hidalgo A (2005) Lichten-
laparoscopic transabdominal hernia repair [in Italian]. Chir Ital
15. Campanelli G, Hidalgo M, Hoeferlin A, Rosenberg J, Champault
G, Kingsnorth A, Miserez M (2009) Randomized controlled trial
607 14th Street, NW, Suite 800 Washington, D.C. 20005 Tel: (202) 783-6040 Fax: (202) 783-6031 Email: slieberman@rfem.com Steven Lieberman Mr. Lieberman was born in New York City and admitted to the Bar of the State of New York in 1985 and the Bar of the District of Columbia in 1993. He is also admitted to practice before the United States Supreme Court; the United States Cour
HALLAZGOS Y REFLEXIONES A UN MES DE ATENCION DE LA LINEA “ABORTO: MAS INFORMACION, MENOS RIESGOS” Es necesario hablar de aborto sin eufemismos ni moralinas. El aborto ya fue: Uno por cada minuto que pasa. El aborto nos inscribe a todas las mujeres en una experiencia común. Según el Ministerio de Salud, en promedio, todas las mujeres pasamos por dos procesos de aborto durante nuestra
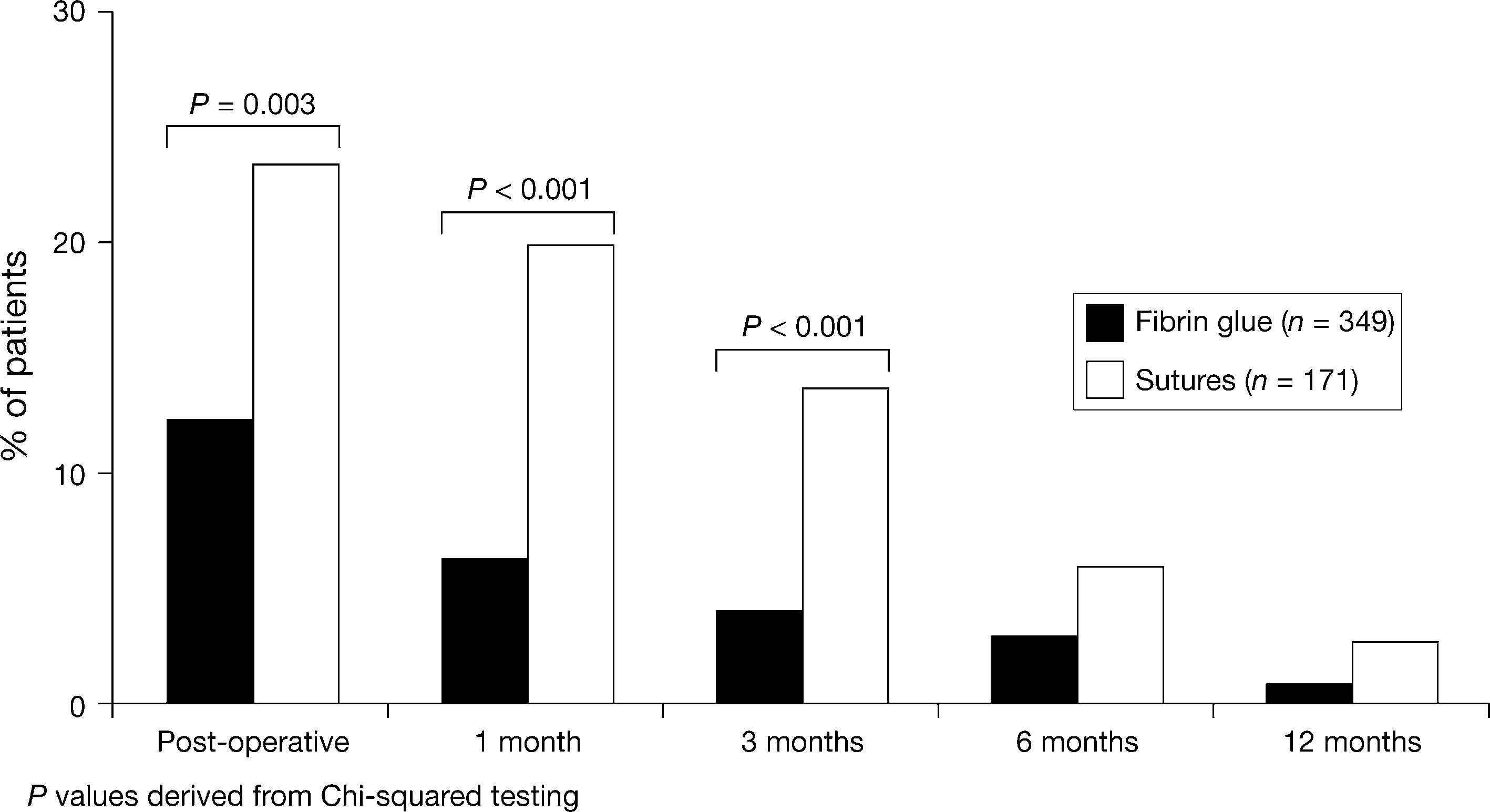 Table 4 Complications experienced during the 12-month follow-up period
34 (19.9%) 14 (4.1%)*** 23 (13.7%) 10 (3.0%)
All P-values were derived from Chi-squared testing, except pain intensity and days of sickness absence, which were derived from Mann–Whitney U testing
VAS visual analog scale ranging from 0 (no pain) to 10 (worst pain); SD standard deviation
**** P = 0.028 versus sutures group One seroma, one unspecifiedà Two scrotal hematomas, one seroma, one fever, one sporadic dysejaculation
Fig. 1 Percentage of patientssuffering from numbness beforeand after surgery
over 12 months. More definitive conclusions about the
compared the 12-month rate of disabling complications
effectiveness of fibrin glue in reducing the rate of postop-
(chronic pain/numbness/groin discomfort) following mesh
erative complications following Lichtenstein repair comes
fixation with Tissucol or sutures in patients with inguinal
from the TIMELI (TIssucol/TIsseel for MEsh fixation in
hernia undergoing Lichtenstein repair []. At 12 months,
LIchtenstein hernia repair) study. This international, con-
the prevalence of C1 disabling complication was signifi-
trolled, randomized, patient- and evaluator-blinded study
cantly lower in the Tissucol group than in the sutures group
Table 4 Complications experienced during the 12-month follow-up period
34 (19.9%) 14 (4.1%)*** 23 (13.7%) 10 (3.0%)
All P-values were derived from Chi-squared testing, except pain intensity and days of sickness absence, which were derived from Mann–Whitney U testing
VAS visual analog scale ranging from 0 (no pain) to 10 (worst pain); SD standard deviation
**** P = 0.028 versus sutures group One seroma, one unspecifiedà Two scrotal hematomas, one seroma, one fever, one sporadic dysejaculation
Fig. 1 Percentage of patientssuffering from numbness beforeand after surgery
over 12 months. More definitive conclusions about the
compared the 12-month rate of disabling complications
effectiveness of fibrin glue in reducing the rate of postop-
(chronic pain/numbness/groin discomfort) following mesh
erative complications following Lichtenstein repair comes
fixation with Tissucol or sutures in patients with inguinal
from the TIMELI (TIssucol/TIsseel for MEsh fixation in
hernia undergoing Lichtenstein repair []. At 12 months,
LIchtenstein hernia repair) study. This international, con-
the prevalence of C1 disabling complication was signifi-
trolled, randomized, patient- and evaluator-blinded study
cantly lower in the Tissucol group than in the sutures group
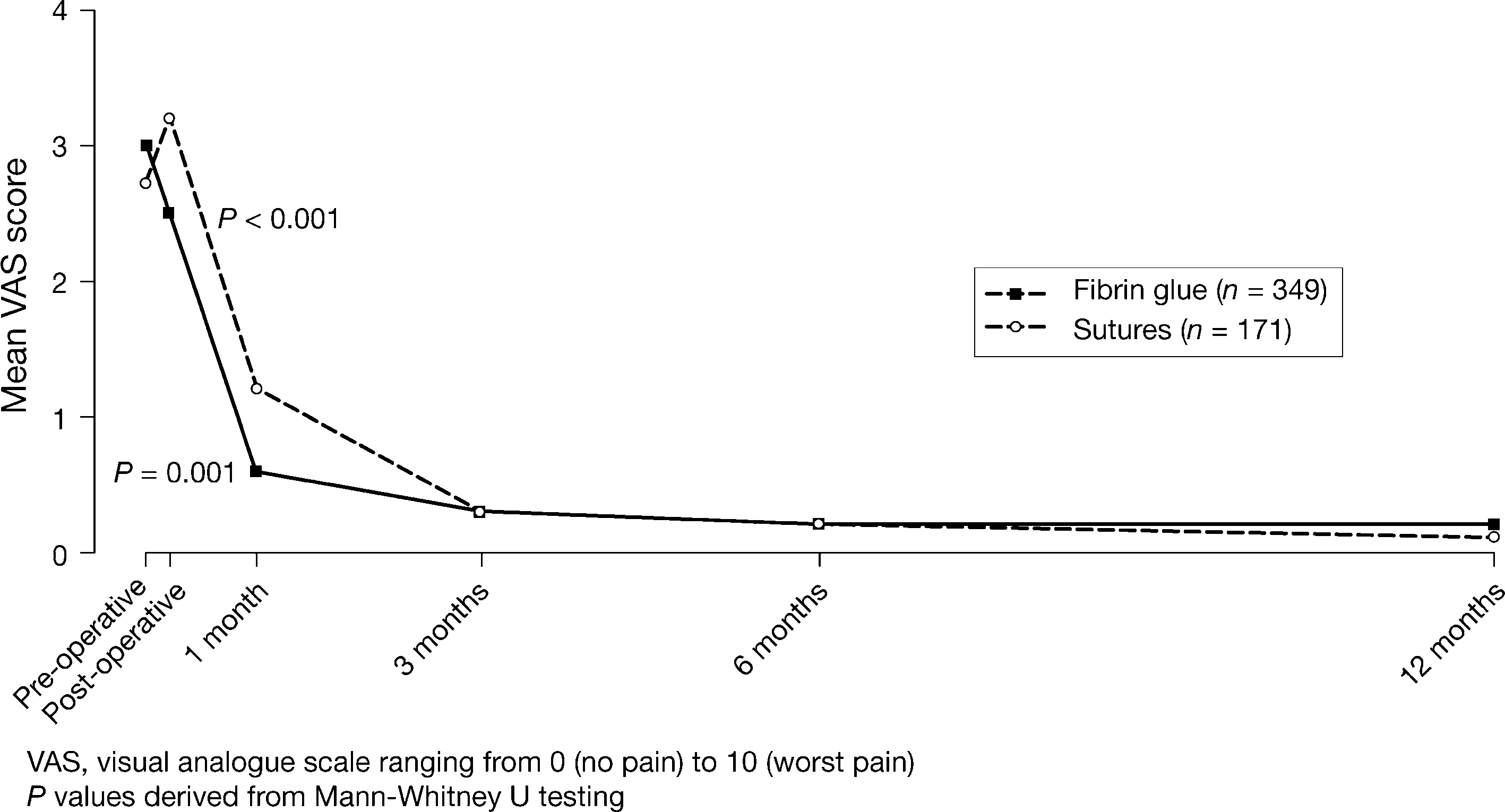 Fig. 2 Pain intensity asassessed by the visual analogscale (VAS) score before andafter surgery
(8.1 vs. 14.8%; P = 0.034) [Less numbness and groin
accompanied by reduction in postoperative inguinal pain.
Fig. 2 Pain intensity asassessed by the visual analogscale (VAS) score before andafter surgery
(8.1 vs. 14.8%; P = 0.034) [Less numbness and groin
accompanied by reduction in postoperative inguinal pain.