Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
English-lss.com
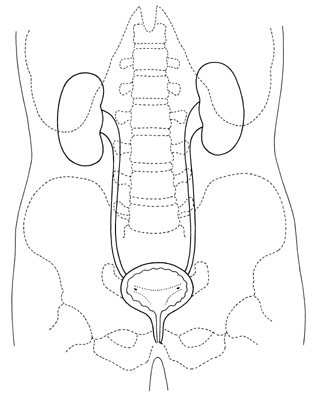
The Urinary System This Version Last Updated On Friday, March 27, 2009
The urinary system consists of the following organs: two kidneys, two ureters, a urinary bladder and
a urethra. The functional unit of the kidney is the Nephron. The functions of the urinary system include regulation of the body fluid volume, pH, osmolarity, and electrolyte composition; excretion of metabolic waste products and excretion of foreign substances; activation of vitamin D; and production of the hormones renin and erythropoietin.
An Overview: The average kidney is about 10 cm long, 5.5 cm
wide and 3 cm in thickness. The kidneys are located on the posterior wall of the abdominal cavity and either side of the vertebral column. They are typically located between the level of the T12 and L3 vertebrae. The kidneys, the two ureters (which connect the kidneys to the urinary bladder) are behind the peritoneum or outside the peritoneal cavity. As a result, these organs are sometimes described as being retroperitoneal. The bladder is located in the pelvic cavity under the peritoneum. Each ureter (approximately 30 cm long) descends lateral to the vertebral column and enters the posterior, inferior surface of the bladder. The urethra exits the inferior surface of the bladder and empties to the exterior of the body. In females the urethra is short, about 4 cm, while in males it is about 19 cm long.
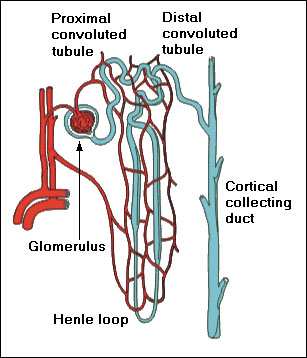
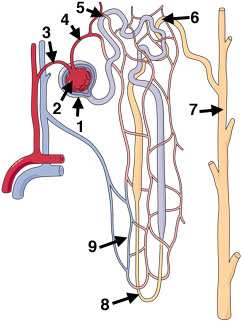
The Nephron: The real work of the urinary system is done by the nephrons within the kidneys. The 2
ureters and the urethra are little more than conduits for moving urine; and the bladder is used to hold urine between periodic urinations (micturitions). Each kidney contains about 1.25 million nephrons. On average 20% of the cardiac output goes to the kidneys each minute or about 1 liter of blood per minute (renal blood flow). From that liter of blood the nephrons filter and process about 125 ml per minute. If all of the filtered amount were turned into urine, it would equal about 180 liters per day. However, the nephrons aggressively reabsorb most of the filtered water and put it back into the circulation. Ultimately only about 1.5 liters (less than 1%) of water is excreted per day. This volume is more than enough to remove the waste products processed by the kidneys. In general, the kidneys must excrete a minimum of 500 ml per day to remove the necessary amounts of waste products. Even at 1.5 liters per day, each nephron is only processing about 0.0006 ml per day or 0.000000417 ml per minute. As you can see in the diagram, the nephron is intimately associated with the vascular system. Plasma is
filtered at a specialized capillary called the glomerulus, while the reabsorbed water is returned to the circulation via capillaries that surround the remaining parts of the nephron. As the filtered fluid passes along the nephron the cells lining the tubules adjust osmolarity, volume, pH and electrolyte balance. Once the fluid leaves the collecting duct its composition can no longer be adjusted. From this point on, it is called urine and is destine for elimination without any further changes. Check Point – Vocabulary Instructions: Match the words in column A with the contextual meaning in column B.
1. consists
2. foreign
3. typically
C. changes designed to make something correct or perfect
4. descends
5. empties
E. describing what will happen to something else over time
6. conduits
7. periodic
8. process
H. greater than required in order to accomplish a task
9. turned into
I. in close contact / in close spatial relationship
10. aggressively
11. ultimately
12. more than enough
13. intimately
14. specialized
O. steps involved with something procedure or activity
16. remaining parts
P. that which is left over / that which has yet to be involved
17. lining
Q. the contents of something are released or removed
18. adjust
R. to convert something into something else
19. destine
20. further
Clinical Corner Catheterization: The process of Urethritis: Inflammation of the Diuretic: A substance [caffeine, Urgency: A symptom of cystitis in Dysuria: Difficult or painful Urinary obstruction: A situation in Frequency: A symptom of cystitis in Clean catch: Method used to get a Urinary tract infection UTI: An Glucosuria: Presence of glucose in Gonorrhea: Type of urethritis
caused by Neisseria gonorhoeae (a
Void: A verb use to describe the Hematuria: Presence of blood in the Continuous ambulatory peritoneal dialysis (CAPD): A process in Hemodialysis: The process in which Incontinence: Inability to retain Nosocomial: An infection acquired Proteinuria: Presence of protein in Cystitis: Inflammation of the urinary Pyelogram: An X-ray of the kidney Dip stick urine tests: Quick test for Pyelonephritis: Inflammation of the Renal calculi (Kidney stones): Talking with the Patient Instructions: work with a partner. One person can read the part of the doctor and the other person can read the part of the patient.
25. D: Yes that’s fine. Let me test it with one of
4. P: I think I may have a bladder infection.
27. D: Yes. This little strip can test a variety of
5. D: Really – tell me what kind of symptoms
things some of which are very indicative
6. P: For starters I’ve got a crampy feeling in my
28. P: Maybe I should get a can of those.
29. D: You can – they are sold over the counter.
Well – let’s see what we’ve got? Nitrates
are positive, leukocytes are positive and a
trace of red blood cells – everything else is
9. D: And you’re sure they are not related to your
10. P: Yes, I finished my last period about two
31. D: These findings are consistent with a
bladder infection. Nitrites are byproducts
11. D: Are you periods normal – any problems –
of bacterial metabolism and leukocytes are
33. D: Blood is sometimes present if the infection
15. D: Okay – go on – what other symptoms do you
more thing – let’s put a little bit in a tube
16. P: It seems like I have to pee every few minutes
– I always have the sensation that I need to
35. D: That will concentrate all this cloudy
material in the bottom of the tube – we can
then stain it and take a look at it under the
18. P: There is also a slight burning sensation when
I urinate and my urine is cloudy and has a
strong smell. I’ve also had a low grade fever
19. D: Have you had any recent illnesses – a cold or
38. D: Okay – well see all those little things
21. D: Well -- all the things you have described
certainly fits cystitis. We can check it out
40. D: Those are bacteria – lots of them.
pretty easily. Here is a sample cup – please
take it down to the toilet and bring back a
sample. We will need a clean catch – so start
the stream first and then get the sample. We
44. D: Don’t worry – 90% of bladder infections
don’t need much – half the cup is more than
22. P: Okay – no problem, I already feel the urge to
46. D: Are you currently taking any medications?
48. D: Are you seeing any other doctors for any
65. P: I work in a microprocessor assembly
50. D: Okay – well, I’m going to prescribe you seven
days of Macrodantin, which is an antibiotic
66. D: Do you work in one of those clean rooms
and I’m also going to give you 2 days worth
of pyridium, which will relieve some of the
67. P: Yes – but the work is easy – nothing
68. D: I’m not worried about the labor part. How
52. D: While you will need to take the antibiotic for
69. P: Oh we can go whenever we want – but we
7 days, the symptoms should be gone in 2
days. So I don’t think you will need more
70. D: So I’m guessing you go as seldom as
54. D: You will need to take the Marcodantin four
times a day – and you should take it after
72. D: How many times do you urinate each day?
meals. I want you to start it right away – so
73. P: I don’t know – may 3 or 4 times.
grab a bite to eat and get the first one down
ASAP. You can then take one after dinner
75. P: Normally never – but since this started –
tonight and then one more with a glass of
76. D: Isn’t it uncomfortable to work while
divide the four doses evenly throughout the
77. P: We all have a routine – we rarely drink
anything before lunch and almost nothing
56. D: The Pyridium should be taken 3 times a day
at lunch. If you don’t drink – you don’t
and it should also be taken with food and at
least 2 glasses of water. Now Pyridium will
78. D: How much water do you drink each day?
turn your urine red-orange – so don’t be
79. P: Not much, 2 cups of coffee, a glass of tea
alarmed – this is quite normal. And Pyridium
will stain you underwear – so don’t wear any
80. D: Well that is a problem – the dehydration
and the infrequent urination is the perfect
recipe for a bladder infection. If you are
58. D: As I said, the pain should be gone in 2 days –
going to continue at this job you are going
if the pain persists after 2 day I want you to
more normally or you’re going to be in
60. D: I also want you to increase you water intake –
and make sure you finish all the antibiotics,
even if you’re feeling fine. If you don’t, you
changes. If it would be helpful for me to
run the risk of the infection coming back.
explain this to the plant manger I will be
62. D: I’m also going to send your sample to the lab
81. P: Thanks – but I don’t think they mind – it’s
for a positive ID of the bacteria in your urine.
It’s not likely, but if it turns out to be
through the hassle. But I guess I’ll have to
something other than E. coli I may want to
change the antibiotic you’re taking. If that
82. D: The key is to not dehydrate yourself and to
happens I’ll call you and let you know. If you
urinate when the urge hits – I mean you
don’t hear from me, you can assume that
can delay for a while, but don’t hold if for
everything is fine. But I expect everything to
be okay and after 7 days you should be fully
84. D: And try to drink at least a liter and half of
64. D: Before you go – can you tell me what sort of
86. D: Here – this brochure that will give you more
information about cystitis and things you can
90. D: Great – call me if you have any problems.
91. P: Okay – thanks Dr. Musaf. Have a good
88. D: Unless, there is a problem, I don’t think there
Taking with the Patient
Instructions: Reread the interview and then, working with a partner, try to recreate the interview using some of the question variations below – then switch roles and recreate the interview again using other question variations. Focus on using the past simple and present perfect tenses during the interview. Questions to Remember (note the verb tenses used in the different types of questions)
Are you currently taking any medications?
Are you seeing another doctor for any health
When did the cramps start? (past simple)
How long have you had the cramps? (present
How many times do you urinate during the
How many times do you urinate at night?
Instructions: Review the interview and find line numbers that correspond to the interview elements listed below. In some cases different aspects of the same interview element may be addressed in different parts of the interview – one such case has been done as an example. The questions in the table below are not in the sequence of the interview. Interview element Line numbers
Request for information on patients chief complaint
Request for information on patients current and recent health
Request for information about medications being taken by patient
Request for information about working environment
Request for information regarding monthly cycle
Explaining what additional tests will be used to confirm the diagnosis
Request for behavioral change regarding urination and hydration
Providing patient written information about regarding their condition
Explaining how lab results will be communicated
Request for information regarding urination habits and frequency
Check Point – Comprehension Instructions: Work with a partner and take turns asking the following questions. When answering, practice giving full answers, not short cryptic answers – don’t limit you use of language.
1. What is the patient’s chief complaint? 2. Based on the interview, what is the minimum and maximum age you would predict for this patient?
What is the rationale for your conclusion?
3. Is this patient seeing any other doctors for health issues? 4. How long has the patient been experiencing the chief complaint? 5. What symptoms does the patient include as part of the description of their CC? 6. What is the initial diagnosis? 7. Describe the medications included in the treatment plan. What is the purpose of each? 8. What urine parameters were particularly important in making the diagnosis? Why? 9. Why is the doctor interested in the patient’s monthly cycle? 10. Why is the doctor concerned about the patient’s work environment?
Practice Dialog
Instructions: Work with a partner to complete the two scenarios. After completing the first scenario, switch roles and complete the second scenario.
Scenario A: Doctor -- Initiate a phone conversation with the patient. (1) explain that the lab results indicate a different bacteria (2) tell the patient that you are going to change her medication to Bactrim (3) explain that the new medication should be taken PO, q12h x 10 days, 1 hr ac or 2 hr pc with 2 glasses of water (4) reiterate the prognosis (5) tell the patient to call if the prognosis does not evolve as expected, (6) reiterate the need for changes in water intake and urination frequency, (7) conclude the conversation. Patient – Ask relevant and realistic questions in response to the information the doctor provides.
Scenario B: Doctor – Initiate a phone conversation with the patient. (1) explain that the lab results confirmed cystitis but also indicated a gonorrhea infection as well (2) explain that she needs to contact all the sexual partners she has had in the last 60 days and tell them that they need to be tested for gonorrhea (3) reassure the patient that this is not a serious complication and the overall prognosis is still fine (4) tell the patient that she needs to come in to get an injection of Rocephin (5) explain that this medication must be injected and will work with only a single dose (6) explain that the disease must be reported, but that the information is confidential (7) schedule an appointment, (8) conclude the conversation. Patient – Ask relevant and realistic questions in response to the information the doctor provides.
Check Point – Asking questions Instructions: work with a partner to write questions that would generate the listed responses from a patient. Then put the Q and A in what you think is the most logical sequence. Compare your sequence with other groups.
Yes, it is very cloudy and has a foul smell.
My health has been fine I haven’t had any recent
No, I’ve never had this problem before.
I don’t drink much water, some coffee and tea.
Check Point – Present Perfect Instructions: Rewrite the sentences in column A in the present perfect form.
2. I worked at the microchip factory since 2005.
3. I was not sick with a cold or flu in over a year.
5. I lived in my present flat for 6 years.
7. I had asthma since I was 7 years old.
8. I no idea how much urine I pass each day.
Cross Word Puzzle
2. by-product of bacterial metabolism found in the
4. abbreviation for take medication by mouth or
4. common name for a woman's monthly cycle
6. a drug used to relieve the pain and cramping of
8. a strong feeling of the need to urinate
9. an infection that is acquired while in the hospital
12. the urinary bladder is located in the _?_ cavity
13. connects the kidneys to the urinary bladder
14. abbreviation for after meals 15. painful of difficult urination
Check Point –Vocabulary Builder Instructions: For each group of 4 words, fine the word that is unrelated to the other 3 words. Odd One Out
Check Point – Past Continuous and Past Simple Instructions: Use the word pairs to complete the sentences. One word in each pair should in the past continuous and the other word in the pair should be in the past simple. Mini-lesson: A common use for past continuous relative to the past simple is when we want to describe a process that was taking place in the past that was interrupted by some event. Example: I was surfing the internet when my brother called from Alaska. (In this example “surfing” is the process that was taking place in the past, which was interrupted when my brother “called.”)
[look / walk] [visit / sound] [start / get] [start / make] [complain / come]
[operate / start] [shake / arrive] [become / study] [ski / notice] [stop / talk]
1. I _____________ when I first _____________ the blood in my urine.
2. I _____________ my friend in the hospital when the fire alarm _____________ and the patients had
3. Just as I _____________ to urinate I _____________ this terrible pain in my urethra.
4. We _____________ friends when I _____________ at the university.
5. The doctor _____________ to pass a kidney stone just as he _____________ the incision to remove
6. Whenever I _____________ by to talk to the Dean, he _____________ always _____________ on
7. Just as I _____________ about the mess, housekeeping _____________ in to clean up the office.
8. The doctor _____________ still _____________ when the patient _____________ to come out
9. While the doctor _____________ for a hypodermic needle, the patient quietly _____________ out of
10. The patient _____________ with chills when the doctor _____________.
Reading
Focus on: Benign prostatic hyperplasia
Prostatic hyperplasia should not be confused with prostatitis. The most common cause of
prostatitis is a bacterial infection which can be treated with antibiotics. Benign prostatic hyperplasia is a hormone induced increase in the number of cells in the prostate gland. Because the prostate completely surrounds the urethra, any increase in the size of the prostate has the potential to compress the urethra and restrict or completely block the flow of urine from the bladder. The resulting symptoms include hesitancy, intermittency, incomplete voiding, weak urinary stream, and straining. Additionally patients experience frequency, which when it occurs at night is called nocturia, and urgency. If left untreated the condition can lead to bladder infections, urethral infections, bladder stones and urinary retention with resulting bladder distension.
middle-aged and elderly men. About one-half of men over fifty have some degree of hyperplasia and the percentage increases with age. By age 90, the percentage of men with this condition may be as high as 90%. The condition is related to the production of testosterone, although the exact hormonal interactions that lead to the condition are still being elucidated. What is clear is that circulating testosterone is converted to dihydrotestosterone (DHT) by the stromal cells of the prostate gland. DHT then binds with nuclear androgen receptors which lead to transcription of mitogenic growth factors that act on the stromal and near by epithelial cells. The increased mitosis leads the hyperplasia associated with this condition.
Benign prostatic hyperplasia can be managed with drugs (alpha blockers) that relax the smooth
muscle in the prostate gland and the smooth muscle associated with the internal urethral sphincter. The relaxation allows urine to pass more freely through the enlarged prostate gland. If pharmacological interventions are inadequate there are a variety of surgical / laser techniques that can be used to reduced the size of the prostate gland. Check Point – Word pairs Instructions: Draw lines between the words in column A and B to make a meaningful word pair related to the article above. Check Point – Vocabulary Instructions: Match the term in column A with its contextual meaning in column B. Terms are taken from the article on Benign Prostatic Hyperplasia.
A. to think something is one thing when it is something else
C. to squeeze something / to reduce the size of something
F. repeated stopping and starting of the urine stream
G. inability to completely empty the bladder
H. reduced urine flow rate during micturition
I. having to use more force than normal to do something
O. to be linked to something / to be related to something
Check Point – Talking about the urinary system. Instructions: Work with a partner. Read the sentences in column A and find the word in column B that best completes the sentence.
1. The patient reported having a _____ during urination.
2. Diabetics have to _____ their urine for protein, ketones and glucose
4. Some drugs used during anesthesia can cause urinary _____.
5. Prostatitis is usually _____ with antibiotics.
6. Benign prostatic hyperplasia is a common problem in _____ men.
7. Acute urinary retention produces an extremely _____ bladder on
8. With chronic retention the bladder _____ and the distention caused
9. The prostate gland is often _____ by palpation through the anterior
10. The urogenital diaphragm forms the external urethral _____.
11. While females do not have a prostate gland they do have an _____
called the Skene’s gland, and like the prostate it can sometimes become inflamed due to a bacterial infection.
12. Prostatic specific antigen (PSA) is an _____ of a prostatic
13. Women tend to have more urinary tract infections (UTIs) than men
because of the _____ between the urethral opening and the anus and because of shorter urethral length.
14. Patients who receive kidney transplants require life-long _____ to
prevent rejection of the transplanted kidney.
15. Statistics indicate that a kidney transplant can _____ a patient’s life
16. Normal urine is usually described as being _____ in color.
17. Bacterial infections can produce _____ , murky or turbid urine.
18. Dark brown urine can indicate liver _____ .
19. Certain vegetables, such as asparagus, can cause the urine to have a
20. _____ can cause the urine to be darker yellow than normal.
Talking with the Patient
Instructions: Work with a partner. One person should play the role of the doctor while the other plays the role of the patient. The doctor should practice asking clear, concise questions to get information about the outlined items. Once finished, switch roles and repeat. The patient needs to provide realistic information – the patient can pretend to have one of the following: cystitis, prostatic hyperplasia, or polycystic kidney disease. 1) Introductions
a) Give your name and get the patient’s
b) Ask an “open-ended” question about the
a) Neurological diseases that could affect
e) Surgical procedures that could affect the
Check Point – Anatomy Review Instructions: Work with a partner to label the diagram. Put the number in the blank next to the corresponding name.
____ glomerular capsule (Bowman’s capsule)
Self-test
1. The average person produces between ___
6. The kidneys and the ureters are said to be:
2. Benign prostatic hyperplasia normally occurs
7. The most immediate solution to acute urinary
9. The kidneys normally receive between 20%
5. The hormone produced by the kidney is:
10. A diuretic is a substance that increases urine
Suggested Mini-Lectures
The mini-lectures listed below can be used as topics for instructors to add additional information to this unit or the topics can be assigned to students for classroom presentations.
Further discussion of the anatomy of the kidney Further discussion of the anatomy of the nephron Discussion of the physiology of the nephron
o Glomerular filtration o Tubular reabsorption o Tubular secretion
Discussion of the renin-angiotensin-aldosterone system Discussion of plasma clearance Discussion of mechanism for excretion of concentrated urine
WHAT’S NEXT FOR OCD MEDICATION? “First line” treatments for OCD (treatments that multiple research studies have shown to be effective in reducing symptoms for a significant number of patients) include medication and cognitive behaviorial therapy, specifically Exposure and Response Prevention. For many people, one of these treatments, or a combination of the two, have been extremely
Cornea Surgery 1 WEEK BEFORE SURGERY STOP any Aspirin, Coumadin, Plavix, Vitamin E 1 DAY BEFORE SURGERY Zymar (antibiotic) Xibrom (anti - inflammatory) 2 doses Discontinue contact lenses NO food or drink after midnight. You may take your normal medications (pills) with sips of water. Remove all eye makeup including eyeliner and mascara Be certain to have driving arrangemen
 The urinary system consists of the following organs: two kidneys, two ureters, a urinary bladder and
The urinary system consists of the following organs: two kidneys, two ureters, a urinary bladder and 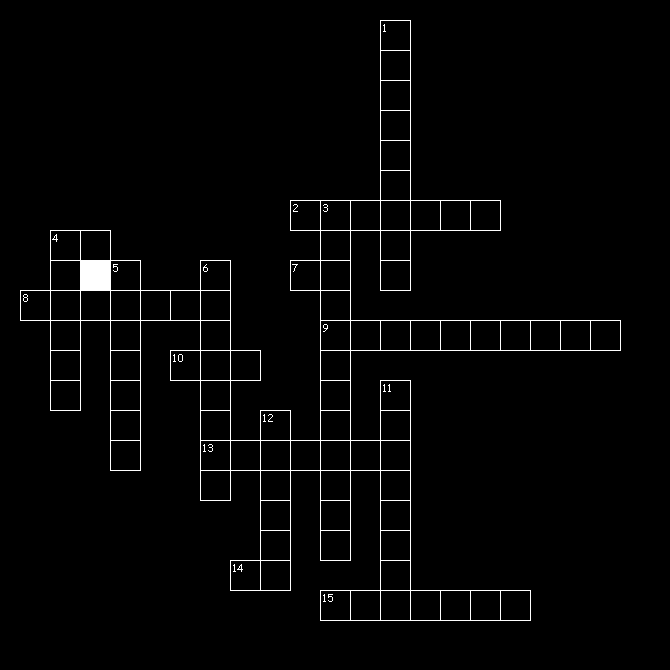 Cross Word Puzzle
Cross Word Puzzle 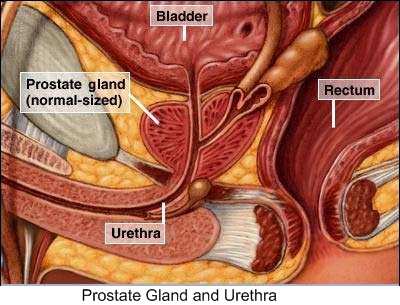
 Check Point – Anatomy Review
Check Point – Anatomy Review