Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
Anxiety disorders and major depression, together or apart
94 Levine et al. DEPRESSION AND ANXIETY 14:94–104 (2001) ANXIETY DISORDERS AND MAJOR DEPRESSION, TOGETHER OR APART
Joseph Levine, M.D.,* Daniel P. Cole, M.D., K. N. Roy Chengappa, M.D., and Samuel Gershon, M.D. This paper will discuss the relationship between anxiety and depression. We will begin with a brief historical perspective. We will then move into the twen- tieth century, with a focus on the 1950s, at which time the introduction of pharmacological treatment options revolutionized the field of psychiatry. The use of psychiatric medications and the observation of treatment response pro- vided an additional means of understanding the relationship between anxiety and depression. From the late 1970s to the 1990s, it became apparent that various medications possessed wider therapeutic profiles than were previously recognized. For example, many medications were found to be efficacious in both anxiety and depressive disorders. These expanded therapeutic profiles pro- vided additional clues to fuel our thinking about the relationship between anxiety and depression. The two major objectives of this paper are, first, to describe and formalize a process of pharmacological dissection and, second, to consider how this process might contribute to our search for a better under- standing of the relationship between anxiety and depression. Depression and Anxiety 14:94–104, 2001. 2001 Wiley-Liss, Inc. Key words: major depression; anxiety disorders; antidepressive agents; antianxiety agents; pharmacological dissection; comorbidity HISTORICAL PERSPECTIVE
hensive phenomenological description of signs and
symptoms. Thus, his description of neurosis was
hroughout the Greco-Roman period up to the
rather general, including symptoms of both anxiety
Rennaissance period, and through much of the 18th,
19th, and the beginning of the 20th century, the entity
Aubrey Lewis [1970-1] in agreement with Map-
of melancholia was understood to encompass symp-
other [1926] proposed a new conceptual viewpoint in
toms of both depression and anxiety [Glass, 1994].
1934, suggesting a continuum between anxiety and
Kraepelin [1927] believed that the mental disorders
depression. He regarded anxiety as an integral part of
were brain disorders and aimed to define discrete and
depression. In fact, Lewis [1966, 1970-71] described a
mutually exclusive psychiatric diseases. Kraepelin dif-
variant of manic-depressive illness in which the major
ferentiated two types of depression. One type was
form was agitated depression and the minor form was
Angst (anxiety) that appeared with melancholia in con-
anxiety neurosis. Lewis too failed to draw a distinction
trast to another type that was Angestlichkeit, character-
ized by helplessness in the face of danger. While
Adolf Meyer [Slater and Roth, 1969] played an im-
Kraepelin made significant contributions to the epis-
portant role in the development of DSM I and II
temology of psychiatric diseases, he made no clear dis-
[American Psychiatric Association, 1952, 1968]. Meyer
tinction between anxiety and depression.
suggested that psychiatric disorders were the conse-
Freud [Fenichel, 1945] was the first to address anxi-
ety as a separate entity. Initially, he proposed that theaccumulation of tension due to frustrated sexual dis-charge was the cause of anxiety. Later in 1926, hedrew a distinction between realistic anxiety (in the face
Stanley Center for the Innovative Treatment of Bipolar Dis-
of actual danger) and neurotic anxiety (in the face of
order, Western Psychiatric Institute and Clinic, Pittsburgh,
subjective perception of danger). Freud spoke sepa-
Pennsylvania
rately on the issue of melancholia in 1917. According
*Correspondence to: Dr. Joseph Levine, Beersheva Mental Health
to Freud, melancholia may encompass symptoms of
Center, P.O. Box 4600, Beersheva, Israel.
both depression and anxiety. On the whole, though,
Freud was more interested in formulating the patient’spsychodynamic forces than in formulating a compre-
Received for publication 10 April 2000; Accepted 10 May 2001
2001 WILEY-LISS, INC. Theoretical Review Article: Depression and Anxiety, Together or Apart 95
quence of an individual’s reaction to internal and exter-
brought a (premature) closure to the question of shared
nal stressors. In both DSM I and II, differentiation be-
vulnerability (matrix) . for anxiety and depression.”
tween disorders was based more on precipitants andseverity of illness than on the quality of symptoms. THE LATE 1980S AND 1990S: ANXIETY AND
Thus, less severe clinical states were diagnosed as
DEPRESSION TOGETHER AGAIN
“neuroses,” while more severe clinical states with no
Various authors challenged the validity of the hier-
clear precipitants were diagnosed as “psychoses.” So, in
archical and exclusionary relationship between anxiety
this schema, the less severe depressive disorder was re-
and depression, as was put forth in DSM III. So
ferred to as depressive neurosis (a neurosis) and the
strongly were these ideas challenged that in DSM III-
more severe form of depression was referred to as a
R and DSM-IV the restriction on Axis I was lifted,
psychotic depressive reaction (a psychosis). Both states
opening the door for the diagnosis of both anxiety and
consisted of a similar symptom profile that consisted of
depressive disorders on Axis I. Soon, it became clear
depressed mood, psychomotor retardation, apprehen-
from epidemiological studies that the comorbidity of
sion, anxiety, and perplexity. Anxiety neurosis, on the
anxiety and depression was quite frequent.
other hand, was said to present with anxiety but was
Table 1 summarizes some of this epidemiologic data
also known to present with symptoms of depression. In
in terms of lifetime comorbidity of several anxiety dis-
the end, neither DSM I nor DSM II drew a clear line
orders with major depressive disorder. In Table 1, data
to distinguish between anxiety and depression.
are reported as rough estimates, since the literature re-
Perhaps, the best summary of the relationship be-
ports a wide range of values for percent of life-time
tween anxiety and depression up to the 1970s was pre-
comorbidity. On the whole, Reiger [1988] estimated
sented by Roth [1972] who stated: “Most of the
that the comorbidity between anxiety disorders and ei-
workers in the field, whether Kraepelinian, psycho-
ther major depressive disorder or dysthymia was 25–
analytic, Meyerian, or Genetical-interactional in their
40%. This is a much higher percentage of comorbidity
approach towards classification of affective disorder,
than would be expected if the disorders were com-
have conceived of anxiety and depression as closely re-
pletely independent (i.e., if comorbidity was solely a
lated and interlocked forms of emotional response in
respect to both normal and pathological reaction.”
So, after less than two decades (the late 1970s and
the1980s), the concept of anxiety and depression being
THE 1970S AND EARLY 1980S: ANXIETY AND
separable entities have again begun to be viewed as less
DEPRESSION APART
distinct and more overlapping entities.
In 1972, Roth and colleagues published epidemio-
logical studies on the classification of affective disor-
EXPLORING THE RELATIONSHIP
ders [Roth et al., 1972; Gurney et al., 1972]. In
BETWEEN DEPRESSION AND ANXIETY
particular, they examined the relationship between
Table 2 summarizes the possible relationship be-
anxiety and depression, differentiating the two on the
tween anxiety and depression. Several lines of investi-
basis of symptom clusters, using “discriminant func-
gation can be used to explore this relationship. A
tion analysis.” These authors found a bimodality of
partial list of these investigations include epidemiol-
symptom scores, suggesting that anxiety states and de-
ogy (including population genetics), neuropsychologi-
pressive illness characterize two different groups of
cal, and CNS pathophysiological studies. Additional
patients. These findings were incorporated into the
approaches involve the comparative analysis of phe-
definitions of psychiatric illnesses in DSM III.
nomenological clusters and the treatment response to
DSM III [1980] was designed to be an atheoretical,
various medications, i.e., pharmacological dissection.
symptom-oriented classification. It introduced explicitinclusion and exclusion criteria, including such data as
TABLE 1. Estimates of life-time comorbidity
number and type of symptoms, age of onset, and type
depression and anxiety*
and extent of disability. It, thus, established thresholdsfor various disorders. It allowed for multiple diagnoses
on Axis II (personality disorders) and on Axis III
(physical disorders). It did not, however, allow for
comorbid diagnosis of an anxiety disorder along with
major depression in Axis I. Moreover, it gave major
depression precedence over anxiety disorders. Simply
put, there was no diagnostic mechanism for acknowl-
edging the presence of an anxiety disorder in the con-
Together, the epidemiologic study of Roth and the
diagnostic guidelines of DSM III supported the idea
*See Gorman, 1997; Kessler, 1994; Ries Merikangas, 1995; Dubson &
that anxiety and depression were two distinct entities. Chung, 1990; Lydiard, 1996; Weissman, 1994; Gorman, 1996; Pasnau,
Of this conclusion, Maser et al. [1995] stated that, “it
96 Levine et al. TABLE 2. Possible relationship between depression
predominantly double-blind studies), findings will be
and anxiety
grouped by disorder, first focusing on the role of anti-depressants in anxiety disorders and then focusing on
Both anxiety and depression are reflections of the same
the role of anxiolytics in major depression. This will
provide us with data necessary for a pharmacological
1. Both are reflections of the same phenomenon (different parts
dissection between the entities of the anxiety disorders
2. One of the two is but a mere relfection of the other
and major depressive disorder. Thereafter, we will dis-
3. One of the two induces changes that lead to the other
cuss the need for higher doses of certain psychotropics
There is a comon factor for both anxiety and depression
in panic disorder and OCD. Although these data are
1. There is common factor to both anxiety and depression (e.g.,
more relevant for a pharmacological dissection within
stress, negative affectivity, or vulnerability). Such
the sphere of anxiety disorders, it will enable us to fur-
vulnerability may interact with other parameters leading to
ther demonstrate the usefulness of pharmacological
anxiety, depression, or mixed anxiety-depression (common
dissection to differentiate disorders.
Anxiety and depression are two separate entitles
ANTIDEPRESSANT USE IN ANXIETY
1. These are two separate entities. Mainly they can be either
DISORDERS
depression or anxiety (sometimes referred to as the
Panic disorder. Klein and Fink [1962] examined be-
2. These are two separate entities. However they may frequently
havioral response to imipramine in an open study of
215 inpatients with anxiety disorders. This was the first
3. These are two separate entities; each can appear at threshold
study to demonstrate the beneficial effect of imi-
or sub-threshold level. Any combination is possible (mixture
pramine in a subgroup of 14 patients who were suffer-
ing from panic attacks. At discharge, 79% (11 of 14)
4. Comorbidity is a common final pathway of two distinct
were improved and 21% (3 of 14) were much im-
proved. The efficacy of imipramine in treatment ofpanic attacks was later confirmed by Klein et al. [1964]in a small double-blind study. Thirteen additional
The method to be used in the remainder of this pa-
double-blind studies have confirmed the efficacy of
per is evaluation of clinical response to psychotropic
imipramine in the treatment of panic disorder, phobia
medications in the context of anxiety and depressive
plus panic attacks, agorophobia plus panic attacks, and
illnesses. First, we will consider a focused review of
phobic anxiety [Jefferson, 1997]. Also, Jefferson [1997]
current data related to the therapeutic profiles of
summarized the data supporting the efficacy of MAOIs
available medications which are currently used in the
in the treatment of panic disorder, suggesting that the
treatment of anxiety and depressive disorders. The
most definitive evidence was provided by Sheehan et
particular disorders that will be considered in this
al. [1980]. In this study 57 patients with “endogenous
analysis are major depressive disorder and the anxiety
anxiety” were treated for 12 weeks with either phenel-
disorders including panic disorder, social phobia, ob-
zine, imipramine, or placebo. At week 6, both drugs
sessive-compulsive disorder (OCD), post-traumatic
were better than placebo. By the end of the study,
stress disorder (PTSD), and generalized anxiety disor-
phenelzine was shown to be more efficacious than imi-
der (GAD). We will then propose some of the guiding
pramine in most of the outcome measures. The SSRIs
principles that are used in our approach to pharmaco-
have also been shown to be effective in panic disorder.
logical dissection. Finally, we will demonstrate the
Black et al. [1993] compared fluvoxamine with placebo
in an 8-week trial. At the end of the study, 81% of pa-tients treated with fluvoxamine were free of symptoms,
MEDICATION TRIALS OF
while only 29% of the placebogroup responded. Effi-
ANXIETY AND DEPRESSION
cacy of sertraline in panic disorder was demonstratedin a large placebo controlled study of 320 patients
The process of pharmacological dissection is based
[Gorman et al., 1994; Rapoport et al., 1998]. Efficacy
upon knowledge of the therapeutic profiles of a vari-
of paroxetine in panic disorder was demonstrated in at
ety of medications or treatments. Since such knowl-
least two double-blind controlled studies [Jefferson,
edge is fundamental to the process of pharmacological
1997; Oehrberg et al., 1995]. Efficacy data for fluoxe-
dissection, we will provide some relevant data en-
tine is supported by a small double-blind study [By-
abling such dissection. In general, it appears that most
stritsky et al., 1994]. Efficacy of citalopram was
medications which are principally used as antidepres-
demonstrated in a large double-blind, placebo and
sants (e.g., TCAs, MAOIs, and SSRIs) are, also, effica-
clomipramine controlled trial of 475 patients [Wade et
cious as anxiolytics (see Table 3). On the other hand,
al., 1997].Alprazolam has been shown to be as effec-
this same reciprocity of therapeutic profiles is not al-
tive as imipramine and to be more effective than pla-
ways evident in medications which are principally used
cebo [Ballenger et al., 1988]. Inositol, a simple sugar
as anxiolytics (e.g., various benzodiazaepines). When
with antidepressant efficacy [Levine, et al., 1995], has
discussing relevant data, (published clinical trials -
been reported to have efficacy in panic disorder, based
Theoretical Review Article: Depression and Anxiety, Together or Apart 97 TABLE 3. Efficacy of pharmacological treatments for anxiety disorders and major depresison
Tranditional antidepressantsSSRIs (including clomipramine)
Traditional anxiolyticsBenzodiazepines (diazepam, clonazepam)
upon a 4-week double-blind cross-over study [Benjamin
[1995] performed a cross-over study of sertraline vs.
et al., 1996]. While the literature addressing efficacy of
placebo, which demonstrated response rates of 50%
the newer antidepressants in panic disorder is inad-
equate in terms of placebo controlled studies, data from
Obsessive-compulsive disorder. The treatment of
one site (n=25) of an 8-week multi-site double blind
OCD with clomipramine has been demonstrated in a
study of venlafaxine for treatment of panic disorder has
large multicenter study (n=520) [Anonymous, Clomi-
demonstrated a trend toward efficacy of venlafaxine as
pramine Collaborative Study Group, 1991]. An aver-
compared to placebo [Pollack et al., 1996].
age reduction in OCD symptoms of 40% was reported
Charney et al. [1986] found trazodone to be less ef-
in the clomipramine group, while only a 4% reduction
fective than imipramine or alprazolam in treating
of symptoms was seen in the placebo group. Several of
panic disorders, and buproprion does not appear to be
the newer SSRIs have also demonstrated efficacy in
effective [den Boer and Westenberg, 1988]. Interest-
OCD [Chouinard, 1992; Griest et al., 1995a,b]. In a
ingly, bupropion does not seem to be effective in panic
multi-center meta-analysis, Griest et al. [1995a] found
that placebo controlled trials have demonstrated that
Social phobia. Keck and McElroy [1997] surveyed
clomipramine, fluoxetine, and sertraline are superior to
the literature on social phobia, finding seven double-
placebo. Clomipramine, however, did have a larger ef-
blind studies of antidepressants being used in the treat-
fect size as compared to the other SSRIs. Trazodone
ment of social phobia. Five of these studies assessed the
was found not to be an effective anti-obsessional agent
efficacy of MAOIs and/or RIMAs (reversible inhibitors
in OCD in one double-blind controlled study [Pigott
of monoamine oxidase) in social phobia. Liebowitz et
al. [1992] conducted an 8-week study comparing par-
Posttraumatic stress disorder. Three studies have
allel groups of phenelzine vs. atenolol vs. placebo.
evaluated TCAs in the treatment of PTSD. Frank et
Response rates were 64% for phenelzine, 30% for
al. [1988] compared imipramine, phenelzine, and pla-
atenolol, and 23% for placebo. Gelernter et al. [1991]
cebo. Both imipramine and phenelzine were found to
conducted a 12-week study that compared parallel
be superior to placebo. Davidson et al. [1990] showed
groups of phenelzine vs. alprazolam versus placebo.
in an 8-week trial that amitriptyline up to 300 mg/day
Response rates were 69% for phenelzine, 38% for
may improve some PTSD symptoms as compared
alprazolam, and 20% for placebo. Versiani et al. [1992]
with placebo. Reist et al. [1989] evaluated the efficacy
also conducted a parallel group study for 16 weeks that
of desipramine vs. placebo and found the desipramine
compared phenelzine vs. moclobemide vs. placebo.
group had improvement of depressive symptoms but
Response rates were 91% for phenelzine, 82% for
no significant improvement of the core PTSD symp-
moclobemide, and 43% for placebo. Another parallel
toms. A double-blind placebo controlled study by van
group study was performed by van Vliet et al. [1992].
der Kolk et al. [1994] demonstrated superiority of
This 8-week study compared brofaromine with pla-
cebo and response rates were 79% for brofaromine
Generalized anxiety disorder. GAD, perhaps, has
(belonging to the RIMA class) and only 14% for pla-
had the least clear results. Hoehn-Saric et al. [1988]
cebo. The final study on MAOIs/RIMAs in social pho-
studied outpatients with GAD in a double-blind trial
bia was again a parallel design, this time for 12 weeks,
comparing alprazolam and imipramine for 6 weeks.
which compared brofaromine with placebo. Response
Both medications were comparable in terms of reduc-
rates were 79% for brofaromine and 26% for placebo
ing anxiety. Imipramine was superior to alprazolam in
[Fahlen et al., 1995]. The remaining two double-blind
terms of reducing depressive symptoms, obsessive and
studies assessed the efficacy of SSRIs in social phobia.
somatic symptoms, hyperarousal, and interpersonal
Van Vliet et al. [1994] studied parallel groups of
sensitivity. Rickels et al. [1993] compared imipramine,
fluvoxamine versus placebo. Response rates were47%
trazodone, diazepam, and placebo over an 8-week pe-
for fluvoxamine and 8% for placebo. Katzelnick et al.
riod in 230 GAD patients. At 3 weeks, all active drugs
98 Levine et al.
were superior to placebo. At week 4 imipramine was
found to be effective in mild to moderate depression,
superior to trazodone and diazepam. By the end of
although they have been shown to be inferior to tricy-
week 6 only imipramine was superior to placebo. No
clic antidepressants (TCAs) in patients with endog-
correlation between baseline depression and the out-
enous or melancholic depression. Furthermore, it is
come was found. However, in a subgroup meeting also
questionable whether triazolo-benzodiazepines amelio-
criteria for major depression, imipramine and trazo-
rate the core symptoms of depression [Casacalenda and
done were superior to diazepam and placebo. Roca et
al. [1997] conducted an 8-week double-blind study of
Buspirone, an anxiolytic drug [Rickels et al., 1990;
paroxetine, imipramine, and 2-chlordesmethyldia-
Fulton, 1997], has shown some efficacy in reducing
zepam in 81 outpatients with GAD. All three medica-
depressive symptoms in patients diagnosed with major
tions showed significant improvement after 8 weeks.
depression which was associated with significant anxi-
However, conclusions drawn from these results should
ety symptoms. Robinson et al. [1990] reported these
be taken with caution for the lack of a placebo group.
results in a large (n=382) double-blind placebo con-
Casacalenda and Boulenger [1998] summarize the results
trolled study, noting that higher doses (40–90 mg per
of these antidepressant drug trials in GAD concluding
day) were used and that particular items of improve-
that TCAs and the SSRI paroxetine demonstrate effi-
ment on the Hamilton Depression Rating Scale repre-
cacy in GAD compatible to that of the benzodia-
sented some of the core depressive symptoms, such as
depressed mood, guilt, work and interest, anergia, anddiurnal variation of mood.Fabre et al. [1990] studied
ANXIOLYTIC USE IN MAJOR DEPRESSIVE
140 outpatients and reported that buspirone (41–54
DISORDER
mg daily) was better than placebo in the treatment of
While many antidepressants are quite effective in
major depression up to 6 weeks (but not in week 8).
the treatment of a variety of anxiety disorders, this
Buspirone was superior to placebo in a subgroup of
same reciprocity does not appear to be the case for the
patients with severe melancholic depression. However,
use of anxiolytics in the treatment of depression.
since the analysis used was intent-to-treat and the
Schatzberg and Cole [1978] reviewed 20 double-blind
drop-out rate was very high, these results should be
studies and concluded that benzodiazepines are not
viewed with caution. Rickels et al. [1997] studied 155
particularly effective for the treatment of depression.
patients suffering from major depression with moder-
A possible exception is the use of the triazolo-benzo-
ate anxiety. Twenty-nine percent of buspirone and
diazepine, alprazolam. Casacalenda and Boulenger
40% of placebo treated patients discontinued treat-
[1998] surveyed 21 double-blind controlled studies
ment before 8 weeks. Thirty-five percent of subjects
comparing alprazolam, TCAs, and/or placebo in adult
taking placebo and 70% of buspirone-treated patients
subjects with major depression. These authors con-
were rated moderately to markedly improved at 8
clude that alprazolam in doses up to 4 mg daily appear
weeks. Casacalenda and Boulenger [1998], surveying
to have an acute effect comparable to that of several
the literature on buspirone in major depression, con-
TCAs in outpatients with mild to moderate major de-
cluded that buspirone has modest antidepressant effi-
pression [Rickels et al., 1985, 1987; Feighner et al.,
cacy especially in patients exhibiting anxiety symptoms
1983]. However, alprazolam does not seem to be ef-
and that one cannot rule out that at least part of the
fective in inpatients with severe major depression or
improvement seen was due to an antianxiety effect of
significant psychomotor retardation or decreased
REM latency [Hubain et al., 1990; Eriksson et al.,1987; Rush et al., 1985]. VARIABLE DOSAGE REQUIREMENTS
Some writers have suggested that high doses of ben-
Benzodiazapines in panic disorder versus GAD.
zodiazepines may be effective in the treatment of de-
Charney and Woods [1989] studied alprazolam and
pression [Tyrer and Tyrer, 1994]. However, Petty et al.
lorazepam in 48 patients with panic attacks with or
[1995] and Lipman et al. [1986] demonstrated in
without agorophobia. Both benzodiazepines were
double-blind placebo controlled studies that chlordia-
shown to have similar efficacy in reducing the panic
zepoxide was not efficacious in the treatment of de-
attacks. It is of note, though, that the doses required to
pression. In a more recent review on this topic,
achieve such response were double those required for
Birkenhager et al. [1995]commented that comparative
the treatment of generalized anxiety (mean daily dose
studies with classical (non-triazolo) benzodiazepines in
of alprazolam and lorazepam, administered for panic
major depression show that these agents do not allevi-
disorder at week 6 of the study, were 2.7 and 6 mg, re-
ate the core symptoms of depression. They do, though,
spectively). Similar results, that is, that higher doses of
have an effect on sleep and anxiety. Classic benzodiaz-
benzodiazepines were required in the treatment panic
epines show some efficacy in minor depression, but
disorder, were reported by Schweizer et al. [1988].
this conclusion, again, may be related to efficacy in pa-
Clomipramine and SSRIs in OCD versus major
tients suffering from anxiety disorders rather than de-
depression. In the meta-analysis by Greist et al.
pression. Triazolo-benzodiazepines, mainly alprazolam
[1995a], fixed-dose studies revealed that the “best”
(mean doses approximately 2.5 to 4 mg/day), have been
doses of fluoxetine and sertraline were 60 mg and 200
Theoretical Review Article: Depression and Anxiety, Together or Apart 99
mg, respectively. The recommended doses of these
RULE OF LIMITED EFFICACY
drugs for major depression are in general about 20 mg
If a medication is efficacious in one disorder, but
of fluoxetine [i.e., Patris et al., 1996]. This data sug-
has a lower rate of response or requires significantly
gests that higher doses of serotonergic antidepressants
higher doses in a second disorder, then we will assume
are necessary for effective treatment of OCD as com-
that there is some biological similarity between these
disorders. However, this situation of limited efficacy,
SUPERIOR EFFICACY OF VARIOUS
also, suggests that there is unshared biological at-
TREATMENTS IN PARTICULAR ILLNESSES OR SUBGROUPS OF ILLNESSES
The intention of our pharmacological dissection is
to gain some insight into the shared and unshared bio-
Superior efficacy of serotoninergic antidepres-
logical characteristics of anxiety and depression. It is
sants in OCD. Whereas other anxiety disorders re-
important to note that, by these rules, we are attribut-
spond to a greater variety of antidepressants, OCD
ing “biological similarity” based on pharmacological
appears to respond more selectively to clomipramine
dissection but not other dissecting tools. So, the con-
and the SSRIs [Lydiard, 1994]. These medications
clusions that we reach through this analytic process
seem to represent one class of antidepressants based
will need to be considered as suggestive only [see also
on our current understanding of putative mechanisms
of action, i.e., serotonergic modulation. EXAMPLES OF AN APPROACH TO PHARMACOLOGICAL PHARMACOLOGICAL DISSECTION DISSECTION
Three examples will be provided in order to dem-
While the intuitive process of pharmacological dis-
onstrate the process of pharmacological dissection.
section is not novel, there is no established method by
The first example will consider the relationship be-
which this process is carried out. Toward this end, we
tween MDD and panic disorder and the second will
draw on the rule of logic known as “Ockham’s Razor,”
consider the relationship between MDD and OCD. A
which was proposed by William of Ockham (1285–
third example will consider the relationship between
1349). Essentially, this rule states that, when seeking
panic disorder and GAD, particularly to demonstrate
to explain the nature of something, the simplest expla-
nation is more likely to be true than a more compli-cated explanation. The elegant simplicity of this
MDD AND PANIC DISORDER
principle was a noticeable departure from other philo-
By the Rule of Shared Efficacy, we conclude that
sophical approaches of the time and it has been sug-
there is some degree of biological similarity between
gested that Ockham’s Razor paved the way for modern
these two disorders. Medications from each of the
three major antidepressant groups (TCAs, SSRIs, and
Using Ockham’s Razor as a guide, we shall formal-
MAOIs) have demonstrated efficacy in both MDD
ize an approach to pharmacological dissection by pre-
and panic disorder [Gorman, 1994, 1996, 1997]. The
senting three basic rules that will be used to compare
two best studied members of the TCA class are imi-
anxiety and depression. In brief, The Rule of Shared
pramine and clomipramine. Studies suggest that these
Efficacy describes situations that suggest biological
two medications are either equivalent in terms of
similarity; The Rule of Unshared Efficacy describes
panic disorder efficacy or that clomipramine may be
situations that suggest biological differences; and The
superior [Boyer, 1995; Modigh et al., 1992]. Good ef-
Rule of Limited Efficacy describes situations that sug-
ficacy for both disorders has been demonstrated with
gest both shared and unshared biological attributes.
By the Rule of Unshared Efficacy, it is important to
RULE OF SHARED EFFICACY
note that bupropion, while it is effective in the treat-
If a single medication is efficacious in two disor-
ment of MDD, does not appear to be efficacious in
ders, then we will assume that these disorders share a
the treatment of panic disorder [Sheehan, 1983].
common biological dysfunction. If this shared effi-
In conclusion, this pharmacological dissection sug-
cacy exists for more than one class of medication,
gests that there is a biological similarity between
then the disorders may share more than one biologi-
MDD and panic disorder. This is supported by the
observation that three classes of antidepressants dem-onstrate efficacy in both disorders. The fact that
RULE OF UNSHARED EFFICACY
buproprion is ineffective in panic disorder suggests
If a single medication is efficacious in one disorder
there are also unshared biological attributes between
but not the other then we will assume that these disor-
ders have different biological attributes.
Speculating briefly about possible meanings in
100 Levine et al.
terms of shared biological attributes, the most consistent
Speculating briefly about the possible meaning of
similarity in terms of putative mechanisms of action is
these similarities, the strongest association between
the role of 5-HT enhancement. Support for this asser-
GAD and panic disorder is demonstrated by the effi-
tion derives from the idea that the most effective antide-
cacy of imipramine, thus suggesting a role for the NE
pressants in the treatment of panic disorder are the
system in these illnesses. While not yet definitively
more pro-serotonergic agents, such as clomipramine
demonstrated, there may be efficacy with paroxetine
and the SSRIs [Boyer, 1995; Modigh et al., 1992]. Addi-
as well. This may eventually lead to recognition that
tionally, the apparent lack of efficacy in panic disorder of
the 5-HT system may be involved in GAD as well.
buproprion, which lacks significant serotonergic effects,
Alternatively, it may reveal that even the relatively
suggests a less significant role for the NE and DA sys-
small NE effects of paroxetine or some other actions
tems in this illness [Ascher et al., 1995].
of paroxetine are involved in the pathology of GAD. The gamma aminobutyric acid (GABA) system, the
MDD AND OCD
apparent active site of the benzodiazepines, may be in-
By the Rule of Shared Efficacy, we can again con-
volved to a greater degree in GAD and to a lesser ex-
clude that there is biological similarity between MDD
and OCD. Primarily, the SSRIs and clomipramine have
If these rules are applied to MDD and other anxiety
been shown to be efficacious in both MDD and OCD.
disorders, such as GAD, PTSD, and social phobias, it
By the Rule of Unshared Efficacy, we note that
will be noted that MDD has shared biological proper-
non-seroternergic antidepressants do not display re-
ties with these disorders as well. However, space con-
ciprocal efficacy in OCD. While there have been case
straints and lack of double-blind studies of several
reports that suggest limited efficacy of several of the
classes of antidepressants in these anxiety disorders
MAOIs, and of the more noradrenergic TCAs, there
prevents us from elaborating further. For example,
are no controlled studies that support the efficacy of
there is lack of good data on TCAs in social phobia
and MAOI and SSRI antidepressants in GAD.
Speculating about shared biological attributes, sero-
tonergic mechanisms of action of clomipramine and
DISCUSSION
the SSRIs suggest that a disordered serotonergic sys-tem may represent a common biological property be-
Since the earliest conceptualizations of melancholia,
this malady was considered to be comprised of bothanxiety and depressive symptoms. Modern pharmaco-
PANIC DISORDER AND GAD
logical treatment for anxiety and depression began in
By the Rule of Shared Efficacy, we conclude that
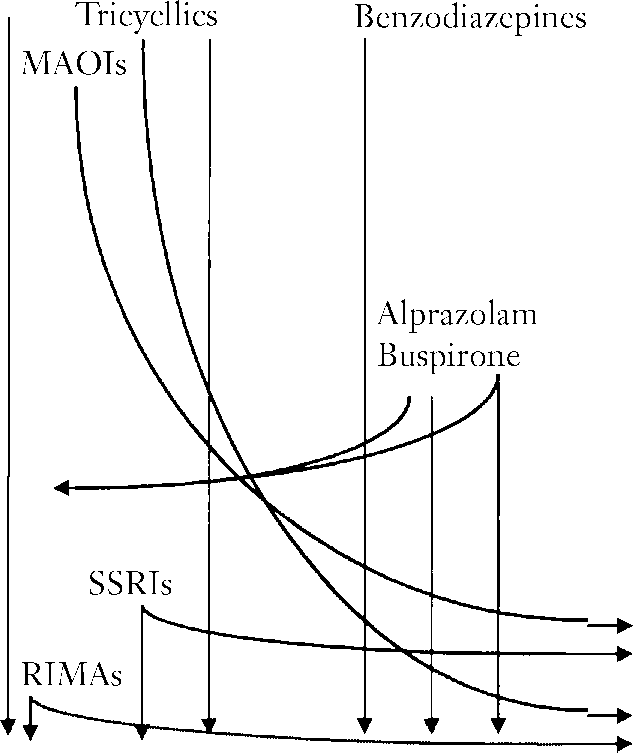
the 1950s. During the 1960s and early 1970s, the ex-
there is biological similarity among panic disorder and
isting knowledge and experience suggested that the
GAD. Since Klein’s demonstration of therapeutic effi-
tricyclic antidepressants (TCAs) and monoamine oxi-
cacy in the 1960s, imipramine is known to be an effec-
dase inhibitors (MAOIs) were efficacious for treat-
tive treatment for panic disorder. More recently, it has
ment of depression and that benzodiazepines (BNZs)
been shown that imipramine isalso an effective treat-
were efficacious for treatment of anxiety, but not vice
ment of GAD [Rickels et al., 1993]. Additionally, the
versa (see Table 4). In contrast to the pharmacological
SSRI paroxetine is clearly effective in the treatment of
dichotomy between anxiety and depression, diagnostic
panic disorder and has been suggested in one recent
manuals prior to DSM III [1980] essentially grouped
study [Rocca et al., 1997] to have efficacy in GAD (this
together what appeared to be pharmacologically dis-
was neither double-blind nor placebo controlled).
tinct entities. In DSM III, however, a specific effort
By the Rule of Limited Efficacy, we consider the
was made to distinguish between anxiety and depres-
case of the benzodiazepines. While standard doses of
sion. By prohibiting the co-diagnoses of major depres-
benzodiazepines appear to demonstrate efficacy in the
sive disorder along with any of the anxiety disorders, it
treatment of GAD, this is not the case for panic disor-
became necessary to separate anxiety and depression,
der. Panic disorder appears to be more responsive to
choosing the most accurate of the two diagnoses in
higher doses of benzodiazepines, such as alprazolam
cases of ambiguity. However, a growing body of psy-
and lorazepam [Charney and Woods, 1989].
chiatric knowledge, based upon clinical observation
In conclusion, this pharmacological dissection sup-
and treatment with available medications (see Table 4)
ports the existence of both shared and unshared bio-
demonstrated that the goal of full separation between
logical properties for these two disorders. Biological
anxiety and depression was unattainable. Thus, subse-
commonality is demonstrated by the efficacy of imi-
quent diagnostic manuals (DSM III-R and DSM IV)
pramine in both illnesses. Preliminary findings suggest
have opted to allow, on Axis I, both diagnoses of major
that the SSRIs may also prove to be efficacious in both
depressive disorder and one or more anxiety disorders.
anxiety disorders.The limited efficacy of the GABA-
Furthermore, in DSM IV, anxiety disorder NOS is de-
ergic medications in panic disorder suggests that be-
fined as a mixture of anxiety and depressive symptoms.
side shared biological attributes there may be unshared
DSM IV also introduces the diagnostic consideration
biological attributes between GAD and panic disorder.
of mixed anxiety-depressive disorder. Theoretical Review Article: Depression and Anxiety, Together or Apart 101 TABLE 4. Evolution of the indications for pharmacological treatments for anxiety and depression during the last five decades
Upon reflection, the current conceptualization of
al., 1996]. Additionally, genetic studies have suggested
the relationship between anxiety and depression is not
similarity in terms of shared genetic risk in both anxi-
fundamentally different from the conceptualization of
ety and depression [Kendler et al., 1987,1992]. Other
several hundred years ago. Anxiety and depression,
findings suggest differences between anxiety and de-
both then and now, appear to be closely linked. Per-
pression. A few examples of unshared characteristics in
haps, the greatest difference is that present day views
anxiety and depression include shortened REM la-
are supported not only by clinical observation but also
tency and increased REM density during the first
by biological data. It is important to realize the value
REM period in depression but not in anxiety disorders
of this accumulating data, since it is a means by which
[Stein et al., 1994], different patterns in platelet recep-
we are able to recognize both similarities and differ-
tor binding [Cameron et al., 1984], and low electro-
ences between the currently defined clinical entities of
dermal activity in major depression compared with
anxiety and depression. In essence, techniques used to
high values in anxiety disorders [Stein et al., 1994].
gain biological data serve as dissection tools to better
Thus we argue that the long-standing perception
define clinical entities. These dissecting tools include,
along with the accumulating biological evidence and
for example, phenomenological, endocrinologic, neuro-
pharmacological dissection suggests both shared and
receptor, and genetic investigations.
unshared characteristics for these two clinical disorders.
Another available approach for studying the rela-
Such suggestions may effect future research by fo-
tionship between anxiety and depression is pharmaco-
cusing on shared and unshared biological characteris-
logical dissection. In the preceding pages, we have
tics instead of concentrating on either entity alone. It
offered an approach based upon three basic rules that
may also affect the development of newer drugs for
can be applied in order to perform such a dissection.
these conditions. For instance, research evaluating
Along with other biological findings, this pharmaco-
drugs for major depression tend to overlook drugs
logical dissection tool can be used to suggest possible
that show efficacy in models for anxiety disorders and
shared and unshared biological matrices for anxiety
vice versa [Robinson and Kurtz, 1990].
and depressive disorders. Several biological findings
In the above dissection, we treated anxiety disorders
support the similarity between anxiety and depression.
and major depression without referring to the evolu-
A few examples of shared characteristics include 1)
tion of these disorders and their different stages. Dif-
blunted growth hormone response to clonidine [Siever
ferences in treatment response to the different classes
et al., 1992; Coplan et al., 1995; Uhde, 1986], 2)
of medications may vary depending upon the “stage”
dysregulation of the hypothalamic-pituitary-adrenal
of the illness. Also, we did not refer to the severity or
axis [Butler and Nemeroff, 1990], and 3) dysfunction
the heterogeneity of the clinical presentation of these
of brain response to serotonergic challenge [Mann et
disorders (i.e., major depression with melancholia vs. 102 Levine et al.
major depression without melancholia). Still another
T, Liebowitz, MR, Gorman, JM. 1995. Persistence of blunted hu-
important variable is the length of the pharmacologi-
man growth hormone response to clonidine in fluoxetine-treated
cal treatment, since there may be a difference between
patients with panic disorder. Am J Psychiatry 152:619–622.
the result of pharmacological dissection done with
Cutler NR, Sramek JJ, Keppel Hesselink JM, Krol A, Roeschen J,
short-term treatment trials (few weeks) compared with
Rickels K, et al. 1993. A double-blind placebo-controlled studycomparing the efficacy and safety of ipsapirone versus lorazepam
long-term trials (several months to years). Future dis-
in patients with generalized anxiety. J Clin Psychopharmacol
sections may need to consider these issues.
Davidson J, Kudler H, Smith R, Mahorney SL, Lipper S, Hammeth
REFERENCES
E, Saunders WB, Cavenar JO, Jr. 1990. Treatment of posttrau-matic stress disorder with amitriptyline and placebo. Arch Gen
Anonymous. 1991. Clomipramine in the treatment of patients with
obsessive-compulsive disorder. The Clomipramine Collaborative
den Boer JA, Westenberg HG. 1988. Effect of a serotonin and no-
Study Group. Arch Gen Psychiatry 48:730–738.
radrenaline uptake inhibitor in panic disorder: a double-blind
Ascher JA, Cole JO, Colin JN, Feighner JP, Ferris RM, Fibiger
comparative study with fluvoxamine and maprotiline. Int Clin
HC, Golden RN, Martin P, Potter WZ, Richelson E, et al. 1995.
Bupropion: a review of its mechanism of antidepressant activity. J
Diagnostic and Statistical Manual of Mental Disorders, 1st edition.
1952. Washington, DC: American Psychiatric Association.
Audi R, editor. 1995. The Cambridge dictionary of philosophy.
Diagnostic and Statistical Manual of Mental Disorders, 2nd edi-
Cambridge: Cambridge University Press. p 543–545.
tion. 1968. Washington, DC: American Psychiatric Association.
Ballenger JC, Burrows GD, DuPont RL, Jr., Lesser IM, Noyes R,
Diagnostic and Statistical Manual of Mental Disorders, 3rd edition.
Jr, Pecknold JC, Rifkin A, Swinson RP. 1988. Alprazolam in
1980. Washington, DC: American Psychiatric Association.
panic disorder and agoraphobia: results from a multicenter trial.
Diagnostic and Statistical Manual of Mental Disorders, 3rd edi-
I. Efficacy in short-term treatment. Arch Gen Psychiatry 45:
tion, revised. 1987. Washington, DC: American Psychiatric
Benjamin J, Levine J, Fux M, Aviv A, Levy D, Belmaker RH. 1995.
Diagnostic and Statistical Manual of Mental Disorders, 4th edi-
Double-blind placebo-controlled crossover trial of inositol treat-
tion, Vol. 886. 1994. Washington, DC: American Psychiatric
ment in panic disorder. Am J Psychiatry 152:1084–1086.
Boyer W. 1995. Serotonin uptake inhibitors are superior to imi-
Dubson KS, Chung MA. 1990. Relationship between anxiety and
pramine and alprazolam in alleviating panic attacks: a meta-
depression: Conceptual and issues. In: Master JD, Cloninger
analysis. Int J Psychopharmacol 10:45–49.
CR, editors. Comorbidity of mood and anxiety disorders. Wash-
Birkenhager TK, Moleman P, Nolen WA. 1995. Benzodiazepines
ington, DC: American Psychiatric Press, Inc. p 631.
for depression? A review of the literature. Int Clin Psycho-
Eriksson B, Nagy A, Sarmark JE, Thelander U. 1987. Alprazsolam
compared to amitriptyline in the treatment of major depression.
Black DW, Wesner R, Bowers W, Gabel J. 1993. A comparison of
Acta Psychiatrica Scand 75:656–637.
fluvoxamine, cognitive therapy, and placebo in the treatment of
Fabre LF. 1990. Buspirone in the management of major depression:
panic disorder. Arch Gen Psychiatry 50:44–50.
a placebo-controlled comparison. J Clin Psychiatry 51:55S–61S.
Butler PD, Nemeroff CB. 1990. Corticotropin-realising factor as a
Fahlen T, Nilsson HL, Borg K, Humble M, Pauli U. 1995. Social
cause of comorbidity in anxiety and depressive disorders. In:
phobia: the clinical efficacy and tolerability of the monoamine oxi-
Master JD, Cloninger CR, editors. Comorbidity of mood and
dase and serotonin reuptake inhibitor barofaromine in double-
anxiety disorders. Washington, DC: American Psychiatric Press,
blind controlled study. Acta Psychiatr Scand 92:351–358.
Feighner JP, Aden GC, Fabre LF, Rickels K, Smith WT. 1983.
Bystritsky A, Rosen RM, Murphy KJ, Bohn P, Keys SA, Vapnik T.
Comparison of alprazolam, imipramine, and placebo in the treat-
1994. Double-blind pilot trial of desipramine versus fluoxetine in
ment of depression. JAMA 249:3057–3064.
panic patients. Anxiety 1:287–290.
Fenichel O. 1945. The psychoanalytic theory of neurosis. New
Cameron GC, Smith CB, Hollingsworth PJ, Nesse RM, Curtis
GC. 1984. Platelet alpha 2-adrenergic receptor binding and
Frank JB, Kosten TR, Giller EL, Jr., Dan E. 1988. A randomized
plasma catecholamines before and during imipramine treatment
clinical trial of phenelzine and imipramine for posttraumatic
in patients with panic anxiety. Arch Gen Psychiatry 41:1144–
stress disorder. Am J Psychiatry 145:1289–1291.
Fulton B, Brogden RN. 1997. Buspirone: an updated review of its
Casacalenda N, Boulenger JP. 1998. Pharmacologic treatment ef-
clinical pharmacology and therapeutic applications (review). Cns
fective in both generalized anxiety disorder and major depres-
sion: clinical and theoretical implications. Can J Psychiatry
Fyer AJ, Leibowitz MR, Klein DF. 1990. Treatment trials, comor-
bidity, and syndromal complexity. In: Maser JD, Cloninger CR,
Charney DS, Woods SW, Goodman WK, Rifkin B, Kinch M,
editors. Comorbidity of mood and anxiety disorders. Washing-
Aiken B, Quadrino LM, Heninger GR. 1986. Drug treatment of
ton, DC: American Psychiatric Press, Inc. p 669–680.
panic disorder: he comparative efficacy of imipramine, alpra-
Gelernter CS, Uhde TW, Cimbolic P, Arnkoff DB, Vittone BJ,
zolam, and trazodone. J Clin Psychiatry 47:580–586.
Tancer ME, Bartko JJ. 1991. Cognitive-behavioral and pharma-
Charney DS, Woods SW. 1989. Benzodiazepine treatment of panic
cological treatments of social phobia: a controlled study. Arch
disorder: a comparison of alprazolam and lorazepam. J Clin Psy-
Glass GA. 1994. A conceptual history of anxiety and depression. In:
Chouinard G. 1992. Sertraline in the treatment of obsessive com-
den Boer JA, Sitsen JMA. Handbook of depression and anxiety.
pulsive disorder: two double-blind, placebo-controlled studies.
New York, NY: Marcel Dekker. p 1–44.
Gorman JM. 1997. The use of newer antidepressants for panic dis-
Coplan JD, Papp LA, Martinez J, Pine D, Rosenbaum LA, Cooper
order. J Clin Psychiatry 58:54–58. Theoretical Review Article: Depression and Anxiety, Together or Apart 103
Gorman JM, Coplan JD. 1996. Comorbidity of depression and panic
Lydiard RB. 1994. Obsessive-compulsive disorder: a new perspective
disorder. Journal of Clinical Psychiatry 57:34–41; discussion 42–43.
in diagnosis and treatment. Int Clin Psychopharmacol 3:33–37.
Gorman J, Wolkow R. June 27–July 1, 1994. Sertraline as a treat-
Lydiard RB. 1996. Panic disorder and social phobia: possible impli-
ment for panic disorder. The XIXth Collegium International
cation of comorbid depression for drug therapy. Anxiety 2:61–70.
Neuropsychopharmacologicum Congress. Washington, DC. Vol
Mann JJ, Malone KM, Diehl DJ, Perel J, Cooper TB, Mintun, MA.
1996. Demonstration in vivo of reduced serotonin responsivity
Greist J, Chouinard G, DuBoff E, Halaris A, Kim SW, Koran L,
in the brain of untreated depressed patients. Am J Psychiatry
Liebowitz, M, Lydiard RB, Rasmussen S, White K, et al. 1995b.
Double-blind parallel comparison of three dosages of sertraline
Mapother E. 1926. Discussion on manic-depressive psychosis. Br
and placebo in outpatients with obsessive-compulsive disorder.
Maser JD, Weise R, Gwirtsman H. 1995. Depression and its
Greist JH, Jefferson JW, Kobak KA, Katzelnick DJ, Serlin RC.
boundaries with selected axis I disorders. Beckham EE, Leber
1995a. Efficacy and tolerability of serotonin transport inhibitors
WR, editors. Handbook of depression, 2nd edition. New York,
in obsessive-compulsive disorder: a meta-analysis. Arch Gen
Merikangas KR, Angst J. 1995. Comorbidity and social phobia evi-
Gurney C, Roth M, , Kerr GT, Schapira K. 1972. Studies in the
dence from clinical, epidemiologic, and genetic studies. Eur
classification of affective disorders: The relationship between anxi-
Arch Psychiatry Clin Neurosci 244:297–303.
ety states and depressive illness-II. Br J Psychiatry 121:162–166.
Modigh K, Westberg P, Eriksson E. 1992. Superiority of clomipra-
Hoehn-Saric R, McLeod DR, Zimmerli WD. 1988. Differential ef-
mine over imipramine in the treatment of panic disorder: a pla-
fects of alprazolam and imipramine in generalized anxiety disorder:
cebo-controlled trial. J Psychopharmacol 12:251–261.
somatic versus psychic symptoms. J Clin Psychiatry 49:293–301.
Oehrberg S, Christiansen PE, Behnke K, Borup AL, Severin B,
Hubain PP, Castro P, Mesters P, de Martelaer V, Mendelwicz J.
Soegaard J, Calberg H, Judge R, Ohrstrom JK, Manniche PM.
1990. Alprazolam and amitriptyline in the treatment of major
1995. Paroxetine in the treatment of panic disorder: a random-
depressive disorder: a double-blind clinical and sleep EEG study.
ised, double-blind, placebo-controlled study. Br J Psychiatry
Jefferson JW. 1997. Antidepressants in panic disorder. J Clin Psy-
Pansau RO, Brystritsky A. 1994. On the comorbidity of anxiety and
chiatry 58:20–4; discussion 24–5.
depression. In: den Boer JA, Sitsen JMA, editors. Handbook of
Katzelnick DJ, Kobak KA, Greist JH, Jefferson JW, Mantle JM,
depression and anxiety. New York: Marcel Dekker. p 45–56.
Serlin RC. 1995. Sertraline for social phobia: a double-blind, pla-
Patris M, Bouchard JM, Bougerol T, Charbonnier JF, Chevalier JF,
cebo-controlled crossover study. Am J Psychiatry 152:1368–1371.
Clerc G, Cyran C, Van Amerongen P, Lemming O, Hopfner
Keck PE, Jr., McElroy SL. 1997. New uses for antidepressants: so-
Petersen HE. 1996. Citalopram versus fluoxetine: a double
cial phobia. J Clin Psychiatry 58:32–36; discussion 37–38.
blind, controlled, multicenter, phase III trial in patients with uni-
Kendler KS, Heath AC, Martin NG, Eaves LJ. 1987. Symptoms of
polar major depression treated in general practice. Int Clin
anxiety and symptoms of depression: same genes, different envi-
ronments? Arch Gen Psychiatry 44:451–457.
Petty F, Trivedi MH, Fulton M, Rush AJ. 1995. Benzodiazepines as
Kendler KS, Neale MC, Kessler RC, Heath AC, Eaves LJ. 1992.
antidepressants: does GABA play a in depression? Biol Psychia-
Major depression and generalized anxiety disorder: same genes,
(partly) different environments? Arch Gen Psychiatry 49:716–722.
Pigott TA, F LH, Rubenstein CS, Bernstein SE, Hill JL, Murphy
Kessler RC, McGonale KA, Zhao S, Nelson CB, Hughes M,
DL. 1992. A double-blind, placebo controlled study of trazo-
Eshleman S, Wittchen HU, Kendler KS. 1994. Life time and 12
done in patients with obsessive-compulsive disorder. J Clin
month prevalence of DSM-III-R psychiatric disorders in the
United States: results from the national comorbidity survey.
Pollack MH, Worthington JJ, 3rd, Otto MW, Maki KM, Smaller
JW, Manfro GG, Rundolph R, Rosenabum JF. 1996. Venlafaxine
Klein DF, Fink M. 1962. Psychiatric reaction pattern to imipra-
for panic disorder: results from a double-blind, placebo-con-
mine. Am J Psychiatry 119:432–438.
trolled study. Psychopharmacol Bull 32:667–670.
Klein DF, Zitrin CM, Woerner M. 1964. Delineation of two drug-
Rapoport MH, Wolkow RM, Clary CM. 1998. Methodologies and
responsive anxiety syndromes. Psychopharmacologia (Berlin)
outcome from the sertaline multicenter flexible-dose trials.
Kraeplin E, Lange J. 1927. Psychiatrie. Band I (neunte Auflange),
Reiger A, Boyd JD, Burke, et al. 1988. One month prevalence of
mental disorders in the United States. Arch Gen Psychiatry
Levine J, Barak Y, Ganzlves M, Szor H, Elizur A, Kofman O,
Belmaker RH. 1995. Double-blind controlled trial of inositol
Reist C, Kauffmann CD, Haier RJ, Sangdahl C, Demet EM,
treatment of depression. Am J Psychiatry 152:792–794.
Chicz-Demet A, Nelson JN. 1989. A controlled trial of de-
Lewis AJ. 1966. In: Scott B, editor. Price’s textbook of medicine.
sipramine in 18 men with posttraumatic stress disorder. Am J
Lewis AJ. 1970–1. The ambiguous word “anxiety.” Int J Psychiatry
Rickels K. 1990. Buspirone in clinical practice. J Clin Psychiatry
Liebowitz MR, Schneier F, Campeas R, Hollander E, Hatterer J,
Rickels K, Feighner JP, Smith WT. 1985. Alprazolam, amitrip-
Fyer A, Gorman J, Papp L, Davis S, Gully R, et al. 1992.
tyline, doxepin, and placebo in the treatment of depression. Arch
Phenelzine vs. atenolol in social phobia: a placebo-controlled
comparison. Archives of General Psychiatry 49:290–300.
Rickels K, Chung HR, Csanalosi IB, Hurowitz AM, London J,
Lipman RS, Covi L, Rickels K, McNair DM, Downing R, Kahn
Wiseman K, Kaplan M, Amsterdam JD. 1987. Alprazolam, diaz-
RJ, Lasseter VK, Faden V. 1986. Imipramine and chlordiazep-
epam, imipramine, and placebo in outpatients with major de-
oxide in depressive and anxiety disorders. I. Efficacy in depressed
pression. Arch Gen Psychiatry 44:862–866.
outpatients. Arch Gen Psychiatry 43:68–77.
Rickels K, Downing R, Schweizer E, Hassman H. 1993. Antide-
104 Levine et al.
pressants for the treatment of generalized anxiety disorder: a pla-
remitted depressed male patients. Neuropsychopharmacology
cebo-controlled comparison of imipramine, trazodone, and diaz-
epam. Arch Gen Psychiatry 50:884–895.
Slater E, Roth M. 1969. Mayer-Gross Slater and Roth Clinical Psy-
Robinson DS, Rickels K, Feighner J, Fabre LF Jr., Gammans RE,
chiatry. 3rd edition. Baltimore, MD: Williams and Wilkines Com-
Shrotriya RC, Alms DR, Andary JJ, Messina ME. 1990. Clinical
effects of the 5-HT1A partial agonists in depression: a composite
Solomon Z, Bleich A. 1998. Comorbidity of posttraumatic stress dis-
analysis of buspirone in the treatment of depression. J Clin
order and depression in Israeli veterans. CNS Spectrum 3:16–21.
Stein MB, Wilson KG, Uhde TW. 1994. The psychophysiology of
Robinson DS, Kurtz NM. 1990. Relationships between anxiety and
depression and anxiety. In: den Boer, Sitsen JMA, editors. Hand-
depression affecting development of antidepressant and antianxi-
book of depression and anxiety. New York: Marcel Dekker. p
ety drugsIn: Maser JD, Cloninger CR, editors. Comorbidity of
mood and anxiety disorders. Washington, DC: American Psychi-
Tyrer P, Tyrer J. 1994. Antidepressive drugs for treatment of anxiety
disorders and vice versa. In: den Boer JA, Sitsen JMA, editors.
Rocca P, Fonzo V, Scotta M, Zalanda E, Ravizza L. 1997. Paroxetine
Handbook of depression and anxiety. New York: Marcel Dekker. p
efficacy in the treatment of generalized anxiety disorder. Acta
Uhde TW, Vittone BJ, Siever LJ, Kaye WH, Post RM. 1986.
Roth M, Gurney C, Kerr GT. 1972. Studies in the classification of
Blunted growth hormone response to clonidine in panic disorder
affective disorders: the relationship between anxiety states and de-
patients. Biol Psychiatry 21:1081–1085.
pressive illness-I. Br J Psychiatry 121:147–161.
van der Kolk BA, Dreyfuss D, Michaels M, Shera D, Berkowitz R,
Rush AJ, Erman MK, Schlesser MA, Roffwarg HP, Vasavada N,
Fisher R, Saxe G. 1994. Fluoxetine in posttraumatic stress disor-
Khatarni M, Fairchild C, Giles DE. 1985. Alprazolam vs. amitrip-
der. J Clin Psychiatry 55:517–522.
tyline in depressions with reduced REM latencies. Arch Gen Psy-
van Vliet IM, den Boer JA, Westenberg HG. 1992. Psychopharma-
cological treatment of social phobia: clinical and biochemical
Schatzberg AF, Cole JO. 1978. Benzodiazepines in depressive disor-
effects of brofaromine, a selective MAO-A inhibitor. Eur Neuro-
ders. Arch Gen Psychiatry 35:1359–1365.
Schweizer E, Fox I, Case G, Rickels K. 1988. Lorazepam vs.
van Vliet IM, den Boer JA, Westenberg HG. 1994. Psychopharmaco-
alprazolam in the treatment of panic disorder. Psychopharmacol
logical treatment of social phobia: a double-blind placebo-con-
trolled study with fluvoxamine. Psychopharmacology 115:128–134.
Sheehan DV, Ballenger J, Jacobsen G. 1980. Treatment of endog-
Versiani M, Nardi AE, Mundim FD, Alves AB, Liebowitz MR,
enous anxiety with phobic, hysterical, and hypochondriacal symp-
Amrein R. 1992. Pharmacotherapy of social phobia: a controlled
toms. Arch Gen Psychiatry 37:51–59.
study with moclobemide and phenelzine. Br J Psychiatry 161:
Sheehan DV, Davidson J, Manschreck T, Van Wyck Fleet J. 1983.
Lack of efficacy of a new antidepressant (bupropion) in the treat-
Wade AG, Lepola, U, Koponen HJ, Pedersen V, Pedersen T. 1997.
ment of panic disorder with phobias. J Clin Psychopharmacol
The effect of citalopram in panic disorder. Br J Psychiatry
Siever LJ, Trestman RL, Coccaro EF, Bernstein D, Gabriel SM,
Weissman MM, Bland RC, Canino GJ, et al. 1994. The cross national
Owen K, Moran M, Lawrence T, Rosenthal J, Horvath TB.
epidemiology of obsessive compulsive disorder. The Cross National
1992. The growth hormone response to clonidine in acute and
Collaborative Group. Journal of Clinical Psychiatry 55:5–10.
F ONDHANDLAR E F ÖRENINGE N [Denna versionen är avsedd att gälla fr.o.m. 2007-11-01] INFORMATION OM EGENSKAPER OCH RISKER AVSEENDE FINANSIELLA INSTRUMENT 1. HANDEL MED FINANSIELLA INSTRUMENT Handel med finansiella instrument , dvs bl.a. aktier i aktiebolag och motsvarande andelsrätter i andra typer av företag, obligationer, depåbevis, fondandelar, penningmarknadsinstrument,
P O S I T I O N S T A T E M E N T Dyslipidemia Management in Adults With Diabetes AMERICAN DIABETES ASSOCIATION (Ͻ40 mg/dl), and modestly elevated trig-lycerides (4). MODIFICATION OF RATIONALE FOR of alcohol or estrogen may also contribute LIPOPROTEINS BY TREATMENT OF MEDICAL NUTRITION DYSLIPIDEMIA — The rationale for THERAPY AND PHYSICAL the treatment of di
 Theoretical Review Article: Depression and Anxiety, Together or Apart
Theoretical Review Article: Depression and Anxiety, Together or Apart