Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
Hyperkalemia -- january 15, 2006 -- american family physician
Hyperkalemia JOYCE C. HOLLANDER-RODRIGUEZ, M.D., and JAMES F. CALVERT, JR., M.D. Oregon Health & Science University, Portland, Oregon Hyperkalemia is a potentially life-threatening metabolic problem caused by inability of the kidneys to excrete potas- sium, impairment of the mechanisms that move potassium from the circulation into the cells, or a combination of these factors. Acute episodes of hyperkalemia commonly are triggered by the introduction of a medication affecting potassium homeostasis; illness or dehydration also can be triggers. In patients with diabetic nephropathy, hyperkalemia may be caused by the syndrome of hyporeninemic hypoaldosteronism. The presence of typical electrocardiographic changes or a rapid rise in serum potassium indicates that hyperkalemia is potentially life threatening. Urine potassium, creatinine, and osmolarity should be obtained as a first step in determining the cause of hyperkalemia, which directs long-term treatment. Intravenous calcium is effective in reversing electrocardiographic changes and reducing the risk of arrhythmias but does not lower serum potassium. Serum potassium levels can be lowered acutely by using intravenous insulin and glucose, nebulized beta2 agonists, or both. Sodium polystyrene therapy, sometimes with intravenous furo- semide and saline, is then initiated to lower total body potassium levels. (Am Fam Physician 2006;73:283-90. Copyright 2006 American Academy of Family Physicians.)
The prevalence of hyperkalemia in Normal Potassium Physiology
hospitalized patients is between Two mechanisms normally regulate potas-1 and 10 percent.1 Although the sium levels in response to variation of potas-exact prevalence of hyperkalemia sium intake. First, ingested potassium rapidly
in community-based medical practice is enters the portal circulation, stimulating the unknown, potassium elevation is a common, pancreas to release insulin. Elevated insulin potentially life-threatening problem most levels induce rapid transport of potassium often occuring in patients with chronic renal from the extracellular space into cells via failure or other illnesses that reduce renal cellular sodium-potassium adenosine tri-potassium excretion (Table 12,3). In these phosphatase. Second, increased potassium patients, acute hyperkalemia often is precipi-
in the circulation causes the renal juxtaglo-
tated by stressors such as illness, dehydration, merular cells to release renin. This stimulates or initiation of medicines that alter potas-
hepatic activation of angiotensin I that is
sium homeostasis (Table 24-10).4-7
then converted in the lungs to angiotensin II.
table 1 Disorders Causing Hyperkalemia Disorders leading to hyperkalemia caused by Disorders leading to hyperkalemia caused by impaired renal excretion of potassium shift of potassium into the extracellular space
Damage to tissue from rhabdomyolysis, burns,
Congenital adrenal hyperplasia (recesssive or
Hyperosmolar states, (e.g., uncontrol ed diabetes,
Primary hypoaldosteronism or hyporeninemia
Systemic lupus erythematosusType IV renal tubular acidosis
Information from references 2 and 3.January 15, 2006 ◆ Volume 73, Number 2American Family Physician 283
Downloaded from the American Family Physician Web site at www.aafp.org/afp. Copyright 2006 American Academy of Family Physicians. For the private, noncommercial
use of one individual user of the Web site. All other rights reserved. Contact copyrights@aafp.org for copyright questions and/or permission requests. Hyperkalemia sort: key reCommeNDatioNs for PraCtiCe
Patients with hyperkalemia who have electrocardiographic (ECG) changes, a rapid rate of rise of serum
potassium, decreased renal function, or significant acidosis should be urgently treated.
Patients with hyperkalemia and characteristic ECG changes should be given intravenous calcium gluconate.
Acutely lower potassium by giving intravenous insulin with glucose, a beta2 agonist by nebulizer, or both.
Total body potassium should usual y be lowered with sodium polystyrene sulfonate (Kayexalate). A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, see page 196 or http://www.aafp.org/afpsort.xml.
Angiotensin II stimulates the adrenal zona glomerulosa
Hyporeninemic hypoaldosteronism, a syndrome asso-
to secrete aldosterone. Elevated serum aldosterone causes ciated with type IV renal tubular acidosis, may be part the renal cortical collecting ducts to excrete potassium of the mechanism behind hyperkalemia in patients with and retain sodium, further lowering serum potassium.2
mild renal failure, particularly diabetic nephropathy. Hyporeninemic hypoaldosteronism can cause patients
Causes of Hyperkalemia
who have diabetic nephropathy to develop acute eleva-
The first step in the evaluation of a patient with elevated tions of potassium because of medications or stress serum potassium is to exclude spurious potassium eleva-
tion (Table 32,3). If the elevation is shown to be real, the next step is to consider: (1) the effects of medica-
meDiCatioN-iNDuCeD HyPerkalemia
tions, including increased potassium intake (Table 24-10); The factors that decrease potassium excretion also increase (2) the impaired distribution of potassium between the the risk of medication-induced hyperkalemia. Because of intracellular and extracellular space; or (3) the impaired the relative decline in renal function with age, family renal excretion of potassium. All three factors often are physicians should use caution when prescribing medica-present (e.g., the stress of illness induces hyperkalemia tions that alter potassium metabolism in older patients. in a patient rendered susceptible by impaired homeo-
Judicious monitoring of potassium levels is important in
static mechanisms and the presence of a medication that at-risk patients receiving these medicines. impairs normal potassium regulation).
Neurohumoral inhibition with angiotensin-converting
enzyme (ACE) inhibitors or angiotensin receptor block-
PseuDoHyPerkalemia
ers benefits patients with chronic heart failure; adding
Pseudohyperkalemia occurs when laboratory reports of spironolactone (Aldactone) reduces morbidity and mor-potassium do not reflect actual values. The most common tality in patients with severe heart failure.13 ACE inhibi-cause is lysis of red cells in a phlebotomy specimen. Other tion also decreases cardiovascular mortality in high-risk causes are listed in Table 32,3. Potassium released from patients, particularly in those with diabetes.14,15 However, platelets can lead to spuriously high levels of potassium patients who take a combination of ACE inhibitors and in a blood sample allowed to clot to collect serum. Pseu-
spironolactone are prone to hyperkalemia8; hyporenin-
dohyperkalemia can be excluded by repeating the sample emic hypoaldosteronism may contribute as well. Non-collection as atraumatically as possible and obtaining steroidal anti-inflammatory drugs (NSAIDs) decrease serum and plasma potassium levels. In patients with renin secretion, leading to decreased potassium secretion. pseudohyperkalemia, the plasma potassium will be nor-
The addition of NSAIDs in these patients can impair renal
mal in the face of an elevated serum potassium.
function to the degree of inducing life-threatening hyper-kalemia. Thus, NSAIDs should be taken with caution in
HyPerkalemia CauseD by DeCreaseD exCretioN
patients with diabetes or renal failure.10,16
of Potassium
Effective excretion of potassium is dependent on aldoste-
aDreNal iNsuffiCieNCy
rone and sufficient distal delivery of sodium and water The possibility of adrenal insufficiency should be consid-within the nephron. Hyperkalemia may occur when one ered in all patients with hyperkalemia. Clinical suspicion of these mechanisms is impaired because of renal failure, is increased by the presence of hyponatremia and mus-renal hypoperfusion (e.g., volume depletion, congestive cular weakness.17 Primary adrenal insufficiency is best heart failure), or hypoaldosteronism. Hypoaldosteron-
screened for with a standard cosyntropin-stimulation
ism may be the cause of hyperkalemia in patients who do test,18 in which 0.25 mg of synthetic cosyntropin is given not have advanced renal failure or hypoperfusion.11
as an intravenous bolus. Plasma cortisol is measured
284 American Family Physician Volume 73, Number 2 ◆ January 15, 2006 Hyperkalemia
table 2 agents that may Cause Hyperkalemia
Diminishes potassium secretion by reducing the electrical gradient between the intracel ular space and
the renal tubule, causing potassium to leave the cel s
Lysine, arginine, or epsilon-aminocaproic acid enters cel s in exchange for potassium, causing hyperkalemia
Decreases aldosterone synthesis; hyperkalemia often can be reduced by concomitant diuretic use; ARBs
less likely to cause hyperkalemia than ACE inhibitors
Inhibits adrenal steroid synthesis, which can lead to aldosterone deficiency
Decreases sodium-potassium adenosine triphosphatase (ATPase) activity; beta2 agonists decrease
Suppresses renin release, leading to decreased aldosterone synthesis, decreased potassium secretion
Decreases sodium-potassium ATPase activity
Blocks aldosterone binding at mineralocorticoid receptors
Decreases aldosterone synthesis; most common in patients on dialysis who drink water with high
Hypertonicity caused by hyperglycemia from glucose infusions can drive potassium out of the
intracel ular space, leading to hyperkalemia. Hyperkalemia may occur with continuous infusions or with boluses of hypertonic glucose. May be present with hypertonicity caused by other agents such as mannitol (Osmitrol) as wel .
Can cause hyperkalemia in patients with decreased renal function; inhibits adrenal aldosterone synthesis
Specific agents include milkweed, lily of the val ey, Siberian ginseng, Hawthorn berries, or preparations
from dried toad skin (Bufo, Chan’su, Senso). All these agents act by decreasing sodium-potassium ATPase activity, leading to elevated extracel ular potassium.
Decreased prostaglandin production leads to decreased afferent arteriolar flow, suppressing renin and
aldosterone secretion. Typical of NSAIDs as well as cyclooxygenase-2 selective inhibitor drugs.
Herbs containing high potassium levels (e.g., Noni juice, alfalfa, dandelion, horsetail, nettle)
Stored cel s can partial y hemolyze and release potassium when infused.
Can cause hyperkalemia in patients with impaired renal function caused by increased potassium load;
can be administered oral y or intravenously
Ingestion of potassium can lead to hyperkalemia, particularly if renal function is impaired; dietary
sources include bananas, melon, and orange juice.
Inhibits binding of aldosterone to receptors in the renal tubule
Increases nicotinic acetylcholine receptors in damaged skeletal muscle (e.g., trauma or burn patients)
Suppresses renin release, leading to decreased aldosterone synthesis and decreased potassium secretion
Diminishes potassium secretion by reducing the electrical gradient between the intracel ular space and
the renal tubule, causing potassium to leave the cel s. ARB = angiotensin receptor blockers; ACE = angiotensin-converting enzymes; NSAID = nonsteroidal anti-inflammatory drug.
*—Hyperkalemia can occur in the setting of amino acids administered intravenously as part of total parenteral nutrition. It is unknown whether oral dietary amino acid supplements cause hyperkalemia.Information from references 4 through 10.
45 to 60 minutes later, and values less than 20 mcg per tends to be less severe as they get older.20 Pseudohypoal-dL (550 nmol per L) suggest adrenal insufficiency.19
dosteronism refers to congenital resistance to the actions of aldosterone on the kidney; the autosomal recessive
CoNgeNital Causes of HyPerkalemia
form is more severe and can lead to death in the neonate
Congenital abnormalities of aldosterone synthesis also if not treated aggressively. Patients suspected to have one can lead to potassium elevation and excessive sodium of these unusual genetic abnormalities should be referred loss. Severe forms of these disorders lead to electrolyte to a pediatric endocrinologist to establish appropriate imbalances in neonates that can be fatal if not corrected initial treatment; patients may then be managed by their promptly. If these patients survive infancy, the disorder family physician with occasional consultation. January 15, 2006 ◆ Volume 73, Number 2American Family Physician 285 Hyperkalemia
table 3 Causes of actual Potassium Values that are lower than laboratory Values
Drawing blood samples from a vein or line into which
potassium levels are significantly altered. Although con-
trolled trials have not been conducted, it is thought that
potassium levels greater than 6.0 mEq per L (6.0 mmol
per L) are clinically significant. ECG changes in a patient
with hyperkalemia are an ominous portent of potentially
fatal arrhythmias. However, hyperkalemia can be life
threatening even if the ECG is normal,25,26 and about one
Repeated clenching of the fist during phlebotomy
half of patients with potassium levels exceeding 6.0 mEq
There are no clear guidelines regarding the appro-
priate setting for the treatment of hyperkalemia. The
decision for hospital admission for continuous ECG
Information from references 2 and 3.
monitoring is a matter of clinical judgment in each case.2,27 Patients believed to have a rapid rise in potas-sium commonly need inpatient care, whereas patients
Diagnosis
whose hyperkalemia has developed over a period of
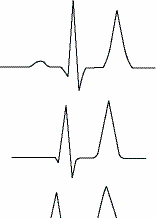
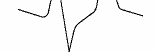
The initial diagnostic approach begins with the clinical weeks can often be managed in an outpatient setting history, review of medications, and physical examination. with close follow-up. Symptoms and signs include muscular weakness or flaccid paralysis, ileus, and characteristic electrocardiograph aCute treatmeNt (ECG) changes (Figure 121). Laboratory tests should Urgent treatment of hyperkalemia includes stabilizing be directed towards causes suggested by the history the myocardium to protect against arrhythmias and and physical examination, with attention to serum shifting potassium from the vascular space into the cells. electrolytes, creatinine, and blood urea nitrogen. A After the serum potassium level is reduced to safe levels, spot urine test for potassium, creatinine, and osmoles should be obtained to calculate the fractional excretion of potassium and the transtubular potassium gradient (Table 422,23). The transtubular potassium gradient is
an assessment of renal potassium handling, with a nor-mal value of eight to nine, rising at times to 11 after an increase in potassium intake. Values lower than five in the face of hyperkalemia suggest an inappropriate renal response to high potassium22; a very low value suggests hypoaldosteronism.
Hyporeninemic hypoaldosteronism should be consid-
ered in patients with diabetes and hyperkalemia, who
generally have a low serum aldosterone. A trial of oral fludrocortisone (Florinef) is generally the most practical way to empirically establish this diagnosis; if the patient has hyporeninemic hypoaldosteronism, potassium lev-
els will return to normal in a day or two after initiation
management Factors necessitating emergent treatment of hyperka- lemia include changes on ECG, a rapid rise of serum potassium, decreased renal function, and the presence of significant acidosis23 (Figure 2). Urgent treatment figure 1. typical electrocardiograph changes seen in
should not be delayed while a work-up for the etiology patients with hyperkalemia. is undertaken, although urine potassium, creatinine, Reprinted with permission from Slovis C, Jenkins R. ABC of clinical electrocar-
and osmolarity studies should be obtained before serum diography: conditions not primarily affecting the heart. BMJ 2002;324:1320.286 American Family Physician Volume 73, Number 2 ◆ January 15, 2006 Hyperkalemia
treatment focuses on lowering total body potassium. In
Sodium bicarbonate is no longer recommended to
patients who do not require urgent treatment, lowering lower potassium, although it may be appropriate in total body potassium may be the only step necessary.
patients with severe metabolic acidosis.32
Intravenous calcium is administered to stabilize the
myocardium; it lowers the threshold potential, thus loweriNg total boDy Potassium counteracting the toxic effect of high potassium. Cal-
Treatments that shift potassium into the cells have no
cium does not have any effect on the serum potassium effect on total body potassium. Potassium can be elimi-level. Improvement in the ECG changes should be vis-
nated by renal excretion, gastrointestinal elimination, or
ible within two to three minutes of administration of dialysis. The agents taken to lower total body potassium calcium (Table 52,3). Repeated doses can be given while can interfere with tests to determine the cause of hyper-other measures are initiated.28
kalemia. Thus, spot urine potassium, creatinine, and
Caution should be used in patients who take digoxin osmolality levels should be obtained before the agents are
because calcium has been reported to worsen the myo-
initiated; however, treatment should not be delayed while
cardial effects of digoxin toxicity.2,3 Some experts sug-
gest using a slower calcium infusion for 20 to 30 minutes
Gastrointestinal excretion is accomplished using
in patients with hyperkalemia who are on digitalis ther-
sodium polystyrene sulfonate (Kayexalate), which binds
apy.28-30 An alternative is to consider using magnesium potassium in the colon in exchange for sodium; it can be instead of calcium to stabilize the myocardium.29
given orally or as a retention enema. The enema form is
Shifting potassium intracellularly is done using insu-
faster; the oral route can take four to six hours because it
lin or a beta2 agonist (Table 52,3). Insulin typically is requires the resin to get to the colon before it takes effect. given as 10 units intravenously with 50 mL of 50 percent Sodium polystyrene sulfonate often is given with sorbi-glucose to counteract hypoglycemia. Repeated doses can tol to decrease constipation. However, sorbitol can have be given if the potassium level remains elevated.
intestinal complications, with reports of bowel necrosis
Inhaled beta2 agonists have a rapid onset of action. and perforation in immunocompromised patients.33
The effect of beta2 agonists is additive to that of insu-
Using furosemide (Lasix) with polystyrene reduces the
lin administration, and they can be taken together.31 risk of volume overload because of the sodium that is Nebulized albuterol (Ventolin) is taken in a dose of exchanged for potassium by the resin (Table 52,3).3310 to 20 mg. Intravenous beta2 agonists have been used
Excretion of renal potassium can be increased
in Europe, but they are not approved by the U.S. Food with the use of diuretics, particularly loop diuret-and Drug Administration.3
ics (e.g., furosemide). Patients with decreased kidney
table 4 Diagnostic equations for Hyperkalemia
FEK less than 10 percent indicates renal etiology
FEK greater than 10 percent indicates extrarenal
Gradient less than 6 to 8 indicates renal cause
Gradient greater than 6 to 8 indicates extrarenal
UK = urine potassium; SK = serum potassium; UCr = urine creatinine; SCr = serum creatinine; Uosm = urine osmolality; Sosm = serum osmolality.
*—For the most accurate representation of the kidney’s response to hyperkalemia, these measurements should be drawn before the serum potassium is corrected. †—Plasma values for potassium and osmolality are recommended for this equation, but serum values are listed because these are more commonly available.Information from references 22 and 23.January 15, 2006 ◆ Volume 73, Number 2American Family Physician 287 Hyperkalemia
function may be relatively resistant to the effects of loNg-term treatmeNt diuretics. If the patient is volume depleted, saline can Long-term treatment should be tailored to correcting be given with the diuretic. Hemodialysis or continu-
the underlying cause of hyperkalemia. Low-potas-
ous renal replacement therapy are the treatments of last sium diets should be discussed with patients, and resort, with the exception of patients already receiving medications that precipitated hyperkalemia should be these therapies.
discontinued if possible. The use of loop diuretics or
management of Hyperkalemia
Is potassium level more than 6.0 mEq per L (6.0 mmol per L) or are electrocardiograph (ECG) changes present?
Patient requires emergency potassium reduction.
Order tests: spot urine potassium, osmolality, creatinine. figure 2. algorithm for the management of hyperkalemia. 288 American Family Physician Volume 73, Number 2 ◆ January 15, 2006 Hyperkalemia
table 5 medications used in acute treatment of Hyperkalemia
repeated doses. Glucose unnecessary if blood sugar elevated above 250 mg per dL (13.9 mmol per L)
*—Medications listed in order of use from most to least urgent.Information from references 2 and 3.
fludrocortisone will be needed for patients with hypo-
renal failure and metabolic acidosis may respond to
reninemic hypoaldosteronism whose hyperkalemia sodium bicarbonate supplementation. The dosage is recurs or is chronic. The usual dosage of fludrocor-
25 to 50 mEq daily (two tablets twice a day at 8 mEq
tisone is 0.1 mg daily, although more will be needed each,) or baking soda (1/2 to 1 tsp daily). Concomitant in some patients. In some patients, hyporeninemic diuretic use limits the risk of volume overload.12 hypoaldosteronism is transitory and resolves after acute management; in others, long-term management the authors
with fludrocortisone is required. Many patients toler-ate long-term use of fludrocortisone with no problems. JOYCE C. HOLLANDER-RODRIGUEZ, M.D., is assistant professor in The principal side effects are hypertension and fluid the Department of Family Medicine at the Oregon Health & Science
University, Portland, Ore, and is a faculty member in the Cascades East
retention, which may respond to an added diuretic. Family Practice Residency Program in Klamath Fal s, Ore. She received her
Although the question of appropriate treatment dura-
medical degree from Oregon Health & Science University and completed
tion with fludrocortisone has never been studied, one a family practice residency at Cascades East. approach to management would be to slowly taper JAMES F. CALVERT, JR., M.D., is associate professor in the Department fludrocortisone on an outpatient basis, and reinstate of Family Medicine at Oregon Health & Science University, and a faculty fludrocortisone if potassium rises.
member in the Cascades East Family Practice Residency Program. Dr. Calvert received his medical degree from George Washington University,
Hyperkalemia caused by the use of ACE inhibitors or Washington, D.C., and completed a family practice residency at the
angiotensin receptor blockers in patients with chronic University of Wisconsin at Madison. January 15, 2006 ◆ Volume 73, Number 2American Family Physician 289 Hyperkalemia Address correspondence to James F. Calvert, Jr., M.D., Merle West
J Med 2000;342:1376; N Engl J Med 2000;342:748]. N Engl J Med
Center for Medical Research, 1453 Esplanade Ave., Klamath Falls, OR 97601-5904 (e-mail: calvertj@ohsu.edu). Reprints are not available
15. McFarlane SI, Sowers JR. Cardiovascular endocrinology 1: aldosterone
function in diabetes mel itus: effects on cardiovascular and renal dis-ease. J Clin Endocrinol Metab 2003;88:516-23.
16. Perazel a MA, Tray K. Selective cyclooxygenase-2 inhibitors: a pattern
of nephrotoxicity similar to traditional nonsteroidal anti-inflammatory drugs. Am J Med 2001;111:64-7. refereNCes
17. Smith JC, Siddique H, Corrall RJ. Misinterpretation of serum cortisol in
a patient with hyponatremia. BMJ 2004;328:215-6.
1. Acker CG, Johnson JP, Palevsky PM, Greenberg A. Hyperkalemia in
hospitalized patients: causes, adequacy of treatment, and results of
18. Dorin RI, Qual s CR, Crapo LM. Diagnosis of adrenal insufficiency [pub-
an attempt to improve physician compliance with published therapy
lished correction appears in Ann Intern Med 2004;140:315]. Ann Intern
guidelines. Arch Intern Med 1998;158:917-24.
2. Gennari FJ. Disorders of potassium homeostasis. Hypokalemia and
19. Becker KL. Principles and practice of endocrinology and metabolism.
hyperkalemia. Crit Care Clin 2002;18:273-88.
3rd ed. Philadelphia: Lippincott Wil iams & Wilkins, 2001.
3. Kim HJ, Han SW. Therapeutic approach to hyperkalemia. Nephron
20. White PC. Disorders of aldosterone biosynthesis and action. N Engl J
4. Perazel a MA. Drug-induced hyperkalemia: old culprits and new
21. Slovis C, Jenkins R. ABC of clinical electrocardiography: conditions not
offenders. Am J Med 2000;109:307-14.
primarily affecting the heart. BMJ 2002;324:1320-3.
5. Perazel a MA. Drug-induced hyperkalemia [Letter Reply]. Am J Med
22. Ethier JH, Kamel KS, Magner PO, Lemann J JR, Halperin ML. The trans-
tubular potassium concentration in patients with hypokalemia and hyperkalemia. Am J Kidney Dis 1990;15:309-15.
6. Pantanowitz L. Drug-induced hyperkalemia [Letter]. Am J Med 2002;
23. Greenburg A, Cheung AK; National Kidney Foundation. Primer on
kidney diseases. 4th ed. Philadelphia: Elsevier Saunders, 2005.
7. Huggins RM, Kennedy WK, Melroy MJ, Tol erton DG. Cardiac arrest
from succinylcholine-induced hyperkalemia. Am J Health Syst Pharm
24. Watanabe T, Nitta K. Transient hyporeninemic hypoaldosteronism in
acute glomerulonephritis. Pediatr Nephrol 2002;17:959-63.
8. Juurlink DN, Mamdani MM, Lee DS, Kopp A, Austin PC, Laupacis A,
25. Martinez-Vea A, Bardaji A, Garcia C, Oliver JA. Severe hyperkalemia
et al. Rates of hyperkalemia after publication of the Randomized
with minimal electrocardiographic manifestations: a report of seven
Aldactone Evaluation Study. N Engl J Med 2004;351:543-51.
cases. J Electrocardiol 1999;32:45-9.
9. Witham MD, Gil espie ND, Struthers AD. Hyperkalemia after the
26. Szerlip HM, Weiss J, Singer I. Profound hyperkalemia without electro-
publication of RALES. N Engl J Med 2004;351:2448-50.
cardiographic manifestations. Am J Kidney Dis 1986;7:461-5.
10. Adhiyaman V, Asghar M, Oke A, White AD, Shah IU. Nephrotoxicity in
27. Charytan D, Goldfarb DS. Indications for hospitalization of patients
the elderly due to co-prescription of angiotensin converting enzyme
with hyperkalemia. Arch Intern Med 2000;160:1605-11.
inhibitors and nonsteroidal anti-inflammatory drugs. J R Soc Med
28. Wil iams ME. Endocrine crisis. Hyperkalemia. Crit Care Clin 1991;
11. DeFronzo RA. Hyperkalemia and hyporeninemic hypoaldosteronism.
29. Davey M. Calcium for hyperkalemia in digoxin toxicity. Emerg Med J
12. Grande Vil oria J, Macias Nunez JF, Miral es JM, De Castro del Pozo S,
30. Weiner ID, Wingo CS. Hyperkalemia: a potential silent kil er. J Am Soc
Tabernero Romo JM. Hyporeninemic hypoaldosteronism in diabetic
patients with chronic renal failure. Am J Nephrol 1988;8:127-37.
31. Lens XM, Montoliu J, Cases A, Campistrol JM, Revert L. Treatment of
13. Pitt B, Zannad F, Remme WJ, Cody R, Castaigne A, Perez A, et al. The
hyperkalemia in renal failure: salbutamol v. insulin. Nephrol Dial Trans-
effect of spironolactone on morbidity and mortality in patients with
severe heart failure. Randomized Aldactone Evaluation Study investiga-
32. Kim HJ. Combined effect of bicarbonate and insulin with glucose in
acute therapy of hyperkalemia in end-stage renal disease patients.
14. Yusuf S, Sleight P, Pogue J, Bosch J, Davies R, Dagenais G. Effects of
an angiotensin-converting enzyme inhibitor, Ramipril, on cardiovas-
33. Gerstman BB, Kirkman R, Platt R. Intestinal necrosis associated with
cular events in high-risk patients. The Heart Outcomes Prevention
postoperative oral y administered sodium polystyrene sulfonate in sor-
Evaluation Study Investigators [published corrections appear in N Engl
bitol. Am J Kidney Dis 1992;20:159-61. 290 American Family Physician Volume 73, Number 2 ◆ January 15, 2006
Dopage, éducation, sport et étude! « (…) Dans un article publié dans le dernier numéro du British Medical Journal, le psychologue australien Vince Cakic prédit que certaines universités ne tarderont pas à soumettre leurs étudiants à des tests antidopage lors des examens (…). Aux États-Unis, un étudiant sur quatre utilise des nootropes, selon une étude de 2005. Provigil, ritali
Fourth Sunday after Trinity Preached by Hugh Bryant 17 July 2011 Romans 8:12-25 - We are debtors, not to the flesh, to live according to the flesh - for if you live according to the flesh, you will die; but if by the Spirit you put to death the deeds of the body, you will live. Romans chapter 8, from which this morning's lesson comes, is the most famous chapter in St Paul's greate
 Hyperkalemia
Hyperkalemia