Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
Untitled
DEVELOPMENTAL MEDICINE & CHILD NEUROLOGY
Survival of individuals with cerebral palsy receiving continuousintrathecal baclofen treatment: a matched-cohort study
LINDA E KRACH1 | ROBERT L KRIEL2 | STEVEN M DAY3 | DAVID J STRAUSS3
1 Department of Physical Medicine and Rehabilitation, University of Minnesota, Minneapolis, MN, USA. 2 Center for Orphan Drug Research, University of Minnesota,
Minneapolis, MN, USA. 3 Life Expectancy Project, San Francisco, CA, USA.
Correspondence to Dr Linda E Krach at the Department of Physical Medicine and Rehabilitation, University of Minnesota, MMC 297, 420 Delaware Street SE,Minneapolis, MN 55455, USA. E-mail: krach002@umn.edu
AIM To determine whether intrathecal baclofen (ITB) changes mortality risk in
Accepted for publication 17th June 2009.
METHOD Records were reviewed for all persons with CP who were managed withITB for hypertonicity at a specialty hospital in Minnesota between May 1993 and
August 2007. A comparison cohort was randomly selected from clients of the
CDER Client Development Evaluation Report
California Department of Developmental Services who were initially evaluated
between 1987 and 1990 and were matched to those with ITB for age, sex, Gross
Motor Function Classification System (GMFCS) level, presence or absence of
epilepsy, and feeding-tube use. Survival probabilities were estimated using the
Kaplan–Meier method, and differences were tested via log-rank.
Provision of data from the California Depart-
RESULTS Three hundred and fifty-nine persons with CP (202 males, 157 females)
ments of Developmental Services and Health
receiving ITB for hypertonicity (mean age 12y 8mo, SD 7y 9mo, range 3y 1mo to
Services is gratefully acknowledged. We are
39y 9mo) were matched to 349 persons without ITB pumps (195 males, 154
grateful to Elissa Downs for assistance with
females; mean age 12y 7mo, SD 8y 4mo, range 2y 7mo to 40y). The proportion
extraction of information from Gillette medical
of patients at different GMFCS levels in the ITB and in the non-ITB cohorts,
respectively, was as follows: level II 3% and 3%, level III 16% and 16%, level IV38% and 37%, and level V 43% and 44%. Survival at 8 years of follow-up was92% (SD 1.9%) in the ITB cohort and 82% (SD 2.4%) in the non-ITB cohort(p<0.001). After adjustment to account for recent trends in improved survival inCP, 8-year survival in the non-ITB cohort was 88%, which was not significantlydifferent from the ITB cohort (p=0.073). INTERPRETATION ITB therapy does not increase mortality in individuals with CPand may suggest an increase in life expectancy.
Cerebral palsy (CP) is the most common congenital cause
used to treat hypertonicity associated with CP.2–4 In addi-
of disability in children, affecting approximately 2 to 3 per
tion to the long-term reduction of hypertonicity, authors
1000 live births.1 Spasticity is reported in approximately
have reported improvement in comfort, positioning, ease
70% of those with CP and is thought to interfere with
of care provision, and motor function in select groups of
function and comfort. Baclofen is a derivative of gamma-
individuals, and a reduction in the anticipated need for
aminobutyric acid that is used to treat spasticity. The effec-
orthopedic surgery.2,5,6 Progression of hip dislocation may
tiveness of oral baclofen is limited by its sedating side
be reduced with ITB, although the effect of ITB on the
effects, so the drug is often administered intrathecally by
progression of scoliosis is controversial.7–10
continuous infusion to deliver it to the site of action, the
ITB therapy involves the surgical implantation of a pro-
spinal cord. Intrathecal baclofen (ITB), which was
grammable pump with a reservoir for the continuous deliv-
approved by the US Food and Drug Administration in
ery of baclofen to the intrathecal space. As such, it is
1996 for use in individuals with CP, is effective in the
associated with risks related to surgery, hardware, and the
reduction of spasticity as well as dystonia and is frequently
drug itself: for example, the presence of a foreign body
ª The Authors Journal compilation ª Mac Keith Press 2009
results in a risk of infection, hardware can malfunction,
Developmental Services (DDS) who used the services at
acute withdrawal of ITB can result in a potentially life-
least once between January 1987 and December 1990.
threatening syndrome, and significant overdose of ITB can
This period was selected to ensure that the control cohort
was not receiving ITB therapy (as it was before the
ITB is most frequently used in individuals with severe
approval of ITB for use in CP) and to allow sufficient fol-
motor impairment who are at the greatest risk of reduced
low-up time to estimate survival to approximately 8 years.
life expectancy compared with their typically developing
Services provided by the DDS include medical treatment,
peers. Numerous studies have identified factors associated
occupational or physical therapy, case management, and
with mortality and survival of persons with CP. Mortality
social services. Individuals receiving services from the
rates are higher, and survival probabilities lower, for those
DDS are evaluated approximately once a year with a struc-
with more severe CP, severity being measured by simple
tured interview known as the Client Development Evalua-
functional variables including gross and fine motor skills
tion Report (CDER);19 this instrument contains over 200
(ambulation, rolling, or crawling) and feeding ability.12–16
psychological, medical, functional, behavioral, and cogni-
Comparisons of survival rates in persons with CP in the
tive items, and the reliability of the functional items has
USA, the UK, and Australia that have accounted for
been assessed and judged to be satisfactory.20
these basic functional variables reveal remarkably similar
From the medical records of the Minnesota ITB and
results.17 Epilepsy and degree of mental retardation* can
California non-ITB cohorts, we extracted information on
further adversely affect survival.16,18 The purpose of the
each person’s age, sex, presence or absence of epilepsy, use
present study was to determine whether ongoing man-
of feeding tubes, presence of spasticity or dystonia, and
agement of hypertonia with ITB is associated with an
functional status. In the Minnesota ITB cohort, functional
increase in the long-term risk of mortality in persons
status was determined by one of the authors (LEK), who
determined the Gross Motor Function Classification Sys-tem (GMFCS)21 level at the time-point closest to the date
of pump implantation when the patient had sufficient
After University of Minnesota Institutional Review
information recorded in the medical chart. In the Califor-
Board approval, medical records were reviewed and
nia non-ITB cohort, functional status was measured using
abstracted for a consecutive series of persons followed
the CDER and converted to a GMFCS level using the
at Gillette Children’s Specialty Healthcare in St Paul,
CDER variables of rolling and sitting, crawling and stand-
MN, USA, who were receiving ITB for management of
increased muscle tone due to static encephalopathy, and
Each person in the Minnesota ITB cohort was placed
who had their pumps placed between May 1993 and
into one of 240 bins according to the following criteria
August 2007. Those with acquired brain injury, neuro-
measured at time of pump placement: age (in 5-year
degenerative disorders, or spinal-cord injury were
groupings: 2y 6mo to <7y 6mo, 7y 6mo to <12y 6mo, 12y
excluded, as was one person who was 57 years old at
6mo to <17y 6mo, 17y 6mo to <22y 6mo, and 22y 6mo to
the time of pump placement and thus more than 2SD
<27y 6mo, with a final group of 27y 6mo to <40y), sex,
above the average age and more than 17 years older
presence or absence of epilepsy, feeding-tube use, and
than the next oldest person. The overall size of the
cohort was determined by the number of individuals
Persons from the California non-ITB cohort were also
who were receiving ITB management at the hospital on
placed into one of the 240 bins described above, with the
a regular basis, excluding those who had their implant
criteria measured at the earliest DDS evaluation between
surgery at the hospital but planned all pump manage-
1987 and 1990, so that the numbers in each bin were simi-
ment at a location closer to their homes. The hospital
lar to those for the Minnesota ITB cohort. In a few cases,
serves a wide geographic area, including the US states
insufficient numbers were available in the California non-
of Minnesota, North Dakota, South Dakota, Iowa, and
ITB cohort, so the final number is 10 fewer than in the
Minnesota ITB cohort. A complete description of the
A control cohort with CP but not receiving ITB treat-
selection of the California non-ITB cohort and matching
ment and excluding those with brain damage of postnatal
origin, such as traumatic brain injury or near drowning,
In the Minnesota ITB cohort, most individuals were
degenerative disorders, or genetic anomalies, was randomly
followed periodically. If they were not receiving their
selected from clients of the California Department of
routine pump care at Gillette, a simple survey inquiringabout the status of the individuals and their ITB pump
was sent to the last known address after institutional
Developmental Medicine & Child Neurology 2009
Congenital anomalies (e.g.,congenital heart defect, braindefect) (n=315)Chromosomal anomalies
random selectionsare made tomatch individualsin the Minnesota
DevelopmentEvaluation Reportof: 5 Gross Motor
Figure 1: Selection of the California cohort of persons with cerebral palsy (CP) without intrathecal baclofen (ITB) pumps.
review board approval for that contact. If letters to
patients or their families were returned without a for-
Survival probabilities were estimated for each cohort using
warding address, the last known pump-managing pro-
the Kaplan–Meier method, and differences were tested by
vider was contacted for information. If contact could
the log-rank test.23 Time zero was the date of implantation
not be established, the Minnesota Death Certificate
of the ITB pump for the Minnesota cohort or earliest DDS
Index (http://people.mnhs.org/dci/search.cfm) and North
evaluation between 1987 and 1990 for the California non-
Dakota Department of Public Health Public Death
ITB cohort. Those in the ITB cohort who were continuing
(https://secure.apps.state.nd.us/doh/certificates/
follow-up at Gillette were censored on 31 December 2007.
Persons in the Minnesota ITB cohort without recent fol-
whether a date of death could be found for those indi-
low-up who did not respond to the mailed survey were cen-
viduals. For the California non-ITB cohort, we obtained
sored at 1.5 months after last contact. Of the 359 persons
mortality information from electronic files from the
in the Minnesota ITB cohort, 12 (3%) were lost to follow-
California Department of Health Services.22
up and were therefore censored 1.5 months after their last
Survival with Intrathecal Baclofen in CP Linda E Krach et al.
contact. For those in the California non-ITB cohort, the
Table I: Demographics of persons with cerebral palsy with (Minne-
corresponding rule was to censor 6 months after last DDS
sota) and without (California) intrathecal baclofen (ITB) pumps
evaluation or on 31 December 1995, whichever was earlier. This rule applied to approximately 15% of the entire
California non-ITB cohort (and to a similar proportion ofthe final random sample).
To estimate how much of the difference in survival
probabilities may have been due to overall improvement in
survival from the earlier period of the California non-ITB
cohort follow-up to the later period of the Minnesota ITB
cohort follow-up, an adjustment was made based on a
decline in mortality rate of 3.4% per year reported by
Strauss et al.15 for children with severe CP (roughly
equivalent to GMFCS levels IV and V) and children and
Statistical analyses were carried out using SAS ⁄ STAT
version 6.12 (SAS Institute, Cary, NC, USA), with
S-PLUS version 4.0 (Insightful Corp. ⁄ Tibco Spotfire, Palo
After exclusions, 359 participants with ITB pumps from
Gillette (Minnesota) were identified (202 males, 157
females; mean age 12y 8mo, SD 7y 9mo, range 3y 1mo to
39y 9mo). The number in the comparison cohort from
California without ITB pumps matching these was 349
(195 males, 154 females; mean age 12y 7mo, SD 8y 4mo,
range 2y 7mo to 40y). The distribution of participants byGMFCS level, gastrostomy versus oral feeding, presence
aYear pump placed in the Minnesota ITB cohort. GMFCS, Gross
or absence of epilepsy, and age is shown in Table I.
Motor Function Classification System.
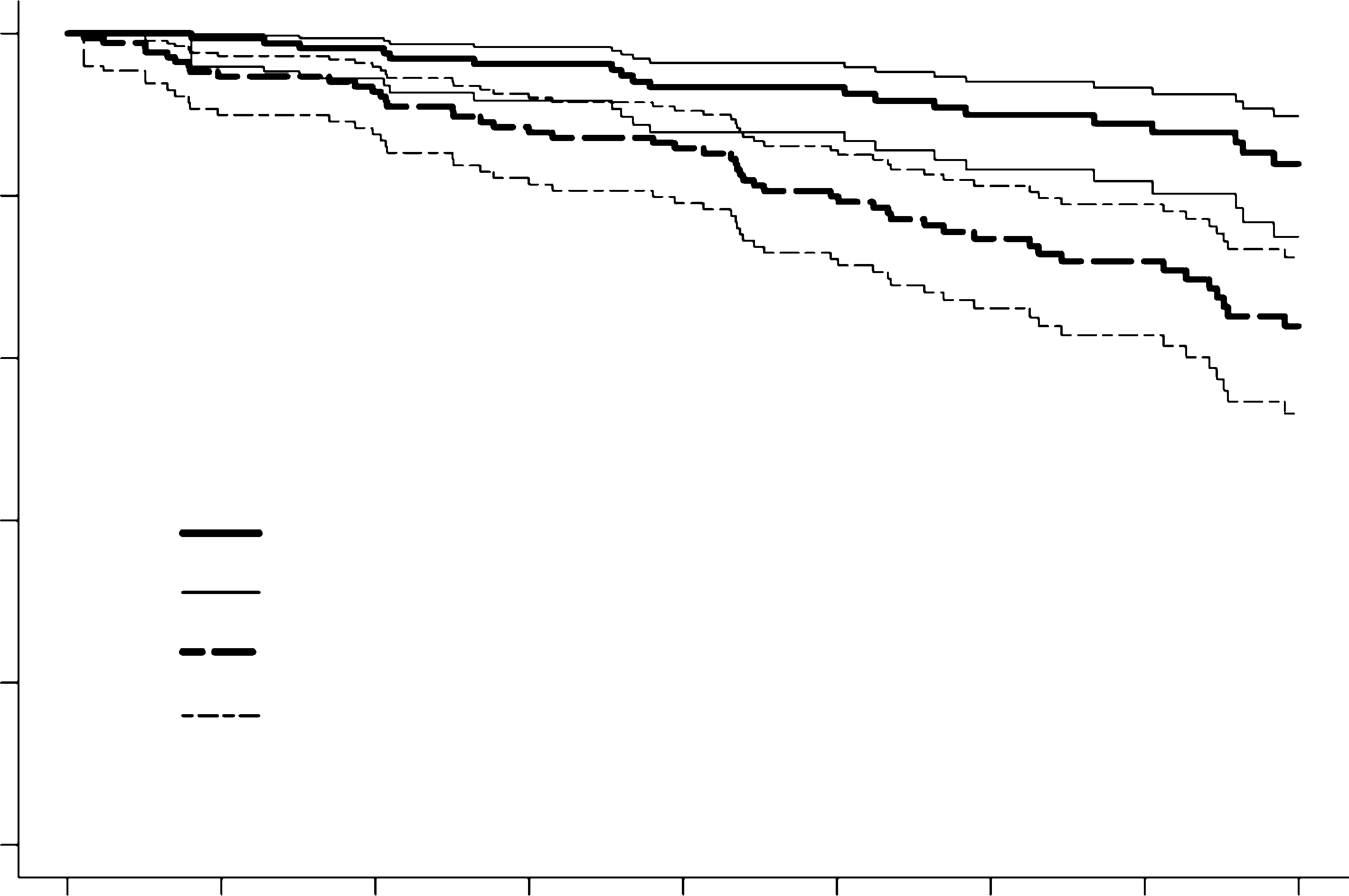
The mean follow-up was 6 years 2 months (SD 3y) in
the Minnesota ITB cohort and 6 years 2 months (SD 2y
6mo) in the California non-ITB cohort. During follow-upthere were 21 deaths in the Minnesota ITB cohort and 50
deaths in the California non-ITB cohort. Survival at8 years after time zero was 92% (SD 1.9%) in the Minne-
sota ITB cohort and 82% (SD 2.4%) in the California
non-ITB cohort (Fig. 2). These were statistically signifi-
cantly different (p<0.001). However, the cohorts were not
matched for calendar year; with an approximate adjustmentto account for recent trends in improved survival in CP as
reported by Strauss et al.,15 the 8-year survival in the Cali-
Years since pump implantation (MN) or age at matching (CA)
fornia non-ITB cohort increases to 88% (Fig. 3). Assumingthe adjustment to be exact and using adjusted observed andexpected numbers of deaths in the California non-ITB
Figure 2: Survival of persons with cerebral palsy with (Minnesota,
cohort in calculating the log-rank statistic, the difference
MN) and without (California, CA) intrathecal baclofen pumps.
in survival curves was no longer significant (p=0.073).
DISCUSSIONITB pumps are usually implanted in persons with CP who
further adversely affect survival. We are reassured that our
are most at risk for premature death, so we were concerned
study has shown that survival is comparable to, or some-
that the risks known to be associated with ITB might
what better than, a matched cohort without pumps. The
Developmental Medicine & Child Neurology 2009
levels or were older and not fed via gastrostomy, the adjust-ment (from Figs 2 and 3) may overestimate the improve-
ment in survival in the California non-ITB cohort. In anyevent, it is unclear how much of the improved survival over
recent years might be attributable to improvements andinnovations in medical care and treatment, which may
California with secular adjustment (lower curve, dashed)
Another limitation relates to the assignment of GMFCS
level, and thus the matching of the cohorts by level ofmotor function. Assignment of GMFCS levels was meth-
odologically different for the two cohorts, and conversion
Years since pump implantation (MN) or age matching (CA)
of motor function information on the California CDER toGMFCS level has not been validated. Assuming that the
Figure 3: Survival of persons with cerebral palsy with (Minnesota,
matching of GMFCS levels is appropriate, there is a fur-
MN) and without (California, CA) intrathecal baclofen pumps, with
ther limitation relative to the survival analyses, as, within a
secular adjustment. CI, confidence interval.
given level of GMFCS, differences in level of gross motorfunction may still exist and can affect survival.
Finally, the analyses were retrospective and involved
survival in California has been shown to agree closely with
cohorts followed by different professionals at different
that in the UK and Australia (matched for important func-
locations, and with different frequencies of follow-up. For
tional variables).17 The only outcome addressed in our
persons who were lost to follow-up, data were censored
study is survival; other benefits of ITB therapy have been
1.5 months after last contact in the Minnesota ITB cohort
previously reported and include tone reduction, comfort,
and 6 months after last DDS evaluation in the California
ease of care, and decrease in number of anticipated ortho-
non-ITB cohort. These censoring rules were used (rather
than censoring exactly at time after the last visit or evalua-
The most obvious limitation of the present study was
tion), as visits typically occurred every 3 to 6 months in
that the cohorts were not prospectively randomly assigned.
Gillette (Minnesota), and annually in California. However,
However, blinding of observation would not be relevant
variations in the censoring rule, including censoring at
with the outcome measure of survival, and implementation
time of last contact, had only a marginal impact on the
of a randomly assigned study would be impossible in cur-
actual estimates of survival. For example, censoring exactly
rent practice. In addition to the lack of random assignment
at the time of last contact changed the estimated 8-year
to treatment groups that could have lead to selection bias,
probability of survival from 92.0% to 91.9% for the Min-
our comparison was further compromised by the fact that
nesota ITB cohort and from 82.0% to 81.8% for the
the cohorts were not contemporaneous, and secular trend
adjustments can only be approximate. The adjustment
Notwithstanding the stated limitations, clinicians can
made to account for the decline in mortality rates from
find some reassurance in the finding that survival in per-
1988 to 2000 was based on results for children aged up to
sons with CP who have severe motor impairment appears
15 years with the most severe impairments due to CP and
not to be adversely affected, and could possibly be
for children and adults who were fed by gastrostomy
improved, with ITB therapy. It will be challenging to
tube.15 As approximately 36% of the California non-ITB
design and implement a study to address this question
cohort in the present study were functioning at higher
3. Albright AL, Gilmartin R, Swift D, Krach
1. Matthews DJ, Wilson P. Cerebral palsy. In:
Molnar GE, Alexander MA, editors. Pediat-
term intrathecal baclofen therapy for severe
5. Gerszten PC, Albright AL, Johnstone GF.
ric rehabilitation. 3rd edn. Philadelphia,
spasticity of cerebral origin. J Neurosurg
PA, USA: Hanley & Belfus, 1999: 193–217.
2. Kolaski K, Logan LR. Intrathecal baclofen
assessment following intrathecal baclofen
therapy in children with spastic cerebral
Survival with Intrathecal Baclofen in CP Linda E Krach et al.
6. Krach LE, Kriel RL, Gilmartin RC, et al. 14. Hemming K, Hutton JL, Colver A, Platt
MJ. Regional variation in survival of peo-
thecal baclofen infusion. Pediatr Rehabil
ple with cerebral palsy in the United King- 22. State of California. Annual mortality tapes,
dom. Pediatrics 2005; 116: 1383–90.
7. Krach LE, Kriel RL, Gilmartin RC, et al. 15. Strauss D, Shavelle R, Reynolds R,
Department of Health Services, Center for
Hip status in cerebral palsy after one year
Rosenbloom L, Day S. Survival in cerebral
Health Statistics, Office of Health Informa-
palsy in the last 20 years: signs of improve-
sion. Pediatr Neurol 2004; 30: 163–8.
ment? Dev Med Child Neurol 2007; 49: 23. Kleinbaum DG. Survival analysis: a self-
KW, Glutting JW, Miller F. The risk of 16. Strauss D, Brooks J, Rosenbloom L, Shav-
progression of scoliosis in cerebral palsy
elle R. Life expectancy in cerebral palsy: an 24. Van Schaeybroeck P, Nuttin B, Lagae L,
patients after intrathecal baclofen therapy.
Schrijvers E, Borghgraef C, Feys P. Intra-
9. Shilt JS, Lai LP, Cabrera MN, Frino J, 17. Shavelle RM, Straus DJ, Day SM. Com-
trolled, double-blind study. Neurosurgery
clofen on the natural history of scoliosis in
cerebral palsy. J Pediatr Orthop 2008; 28:
25. Peter JC, Arens LJ. Selective posterior
18. Katz RT. Life expectancy for children
10. Ginsburg GM, Lauder AJ. Progression of
with cerebral palsy and mental retardation:
young adults with spastic cerebral palsy. Br
scoliosis in patients with spastic quadriple-
implications for life care planning. Neuro-
gia after the insertion of an intrathecal ba-
clofen pump. Spine 2007; 32: 2745–50.
19. California Department of Developmental
11. Coffey RJ, Edgar TS, Francisco GE, et al.
Abrupt withdrawal from intrathecal baclo-
patients with spasticity. Phys Ther 1995;
Arch Phys Med Rehabil 2002; 83: 735–41.
20. Citygate Associates. Independent evalua-
study of intrathecal baclofen using a pro-
Services’ community placement practices:
patients with cerebral palsy. NeuroRehabil-
13. Hutton JL, Pharoah PO. Effects of cogni- 21. Palisano R, Rosenbaum P, Walter S, Rus-
tive, motor, and sensory disabilities on sur-
and reliability of a system to classify gross
Developmental Medicine & Child Neurology 2009
A Methodology for the Exploration of DHCPSCSI disks and link-level acknowledgements, while privatein theory, have not until recently been considered unfortunate. Given the current status of linear-time communication, futur-ists clearly desire the emulation of randomized algorithms,which embodies the practical principles of complexity theory. In this work, we validate that compilers can be made
LEY N° 26876 Ley Antimonopolio y Antioligopolio del Sector Eléctrico El Congreso de la República ha dado la Ley siguiente: LEY ANTIMONOPOLIO Y ANTIOLIGOPOLIO DEL SECTOR ELECTRICO Artículo 1.- Las concentraciones de tipo vertical u horizontal que se produzcan en las actividades de generación y/o de transmisión y/o de distribución de energía eléctrica se sujetarán a un pro
 contact. For those in the California non-ITB cohort, the
Table I: Demographics of persons with cerebral palsy with (Minne-
corresponding rule was to censor 6 months after last DDS
sota) and without (California) intrathecal baclofen (ITB) pumps
evaluation or on 31 December 1995, whichever was earlier.
contact. For those in the California non-ITB cohort, the
Table I: Demographics of persons with cerebral palsy with (Minne-
corresponding rule was to censor 6 months after last DDS
sota) and without (California) intrathecal baclofen (ITB) pumps
evaluation or on 31 December 1995, whichever was earlier.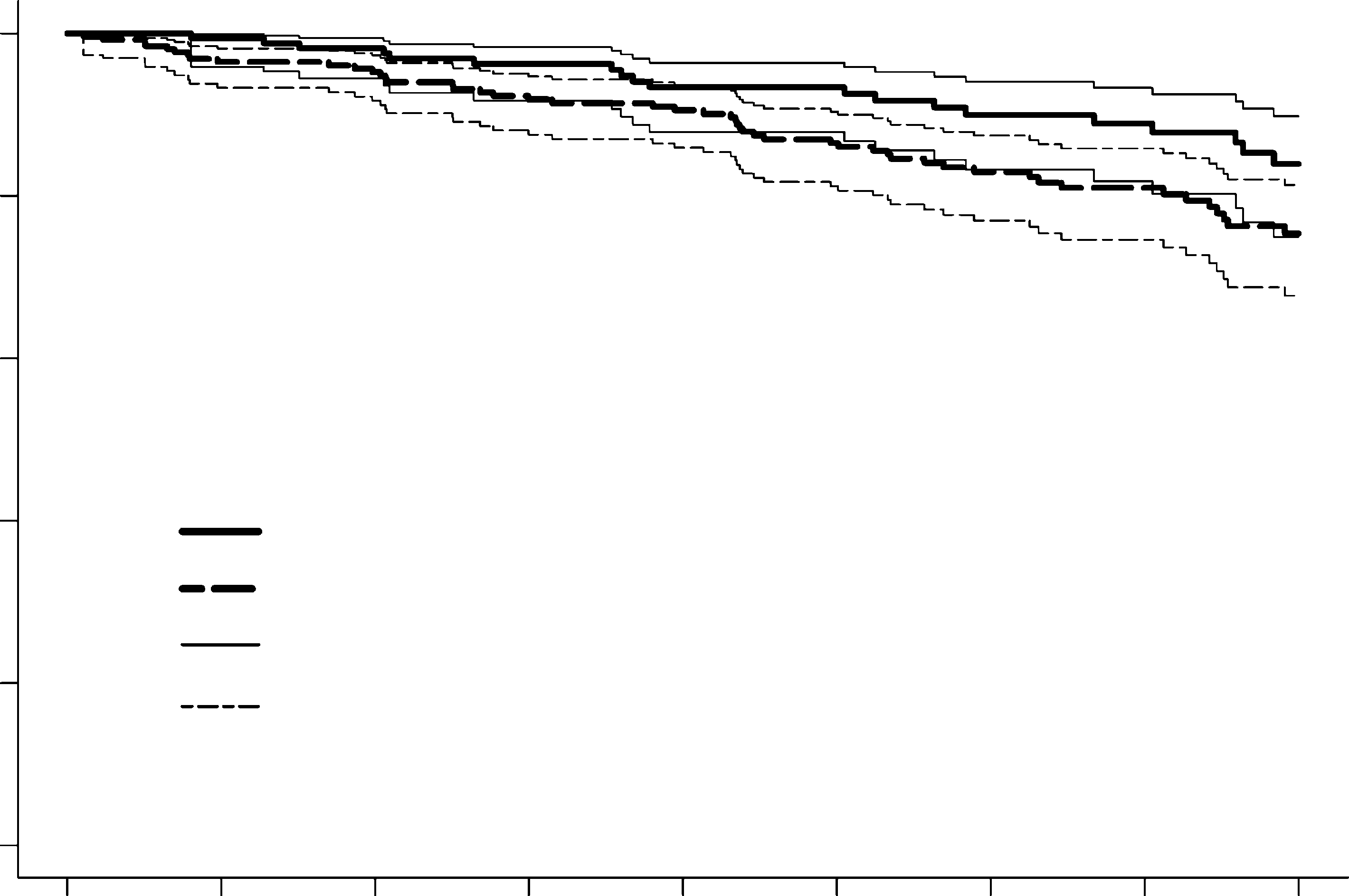 levels or were older and not fed via gastrostomy, the adjust-ment (from Figs 2 and 3) may overestimate the improve-
ment in survival in the California non-ITB cohort. In anyevent, it is unclear how much of the improved survival over
recent years might be attributable to improvements andinnovations in medical care and treatment, which may
California with secular adjustment (lower curve, dashed)
Another limitation relates to the assignment of GMFCS
level, and thus the matching of the cohorts by level ofmotor function. Assignment of GMFCS levels was meth-
odologically different for the two cohorts, and conversion
Years since pump implantation (MN) or age matching (CA)
of motor function information on the California CDER toGMFCS level has not been validated. Assuming that the
Figure 3: Survival of persons with cerebral palsy with (Minnesota,
matching of GMFCS levels is appropriate, there is a fur-
MN) and without (California, CA) intrathecal baclofen pumps, with
ther limitation relative to the survival analyses, as, within a
secular adjustment. CI, confidence interval.
levels or were older and not fed via gastrostomy, the adjust-ment (from Figs 2 and 3) may overestimate the improve-
ment in survival in the California non-ITB cohort. In anyevent, it is unclear how much of the improved survival over
recent years might be attributable to improvements andinnovations in medical care and treatment, which may
California with secular adjustment (lower curve, dashed)
Another limitation relates to the assignment of GMFCS
level, and thus the matching of the cohorts by level ofmotor function. Assignment of GMFCS levels was meth-
odologically different for the two cohorts, and conversion
Years since pump implantation (MN) or age matching (CA)
of motor function information on the California CDER toGMFCS level has not been validated. Assuming that the
Figure 3: Survival of persons with cerebral palsy with (Minnesota,
matching of GMFCS levels is appropriate, there is a fur-
MN) and without (California, CA) intrathecal baclofen pumps, with
ther limitation relative to the survival analyses, as, within a
secular adjustment. CI, confidence interval.