Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
Stockard.pages
Although the term golfer’s elbow has
Clinical practice
historically described medial epicondyli-tis, the more common problem is actuallylateral epicondylitis. McCarroll and col-leagues5 found lateral elbow pain to be
Elbow injuries in golf
more common than medial pain by a5:1 ratio in amateur golfers. Other inves-tigators have found the incidence to be
approximately equal. Lateral epicondylitisoccurs on the left elbow of a right-hand-ed golfer. Medial epicondylitis affecting
Golf is not a sport known for its high injury level; however, injuries do occur. Such mishaps usually involve overuse-type injuries that are more common among amateur golfers than among professional golfers. This article attempts to provide an overview of golf injuries to the elbow, with a concentration on incidence, proper diagnosis, adequate treatment (including rehabilitation), and prevention
tive strokes that leave large divots (Figurestrategies. After reading this article, primary care physicians should be able to man- age most golfing injuries to the elbow. (Key words: primary care, sports medicine, elbow, golf)
caused by the same mechanisms as withnongolfing activities. Specifically, thiscondition is caused by repetitive forceful
Golf is generally considered to be a elbow is the most commonly injured extension of the forearm accompanied
by a twisting motion, especially if asso-
obic benefit that requires a great deal of
the back a close second and the shoulder,
ciated with excessive gripping of the golf
hand, and wrist following that (Table2).3 This may be due to the greater car-
other sports, however, is that it is played
ceivably) avulsion fractures of the medi-
golfers’ injuries occurred primarily from
literature is sparse concerning these con-
ditions. Radial tunnel syndromes are rare
competition. Overuse in either practice or
the frequency of specific injuries differs
golf rounds is the leading cause of injury
among professionals and amateurs (Table3), with poor swing mechanics being an
exclusive cause of injury in amateurs.1,5
spurs and loose bodies may be the cause.6
Most other injuries occur as the golf club
followed by the low back (Table 1).1
patient’s history is the critical part of the
teur golfers, the low back is injured most
diagnosis. History is key, for example, in
differentiating between overuse and acute
Dr Stockard is an associate professor in the
Department of Family Medicine and division
chief of Primary Care Sports Medicine at the
rise” in golfers aged 35 to 55 years. Over-
University of North Texas Health Science Cen-
University of North Texas Health Science Cen-
patient’s injury and find out if any activ-
JAOA • Vol 101 • No 9 • September 2001 • 509
tingling along with the pain, suspect some
Professional Golf Injuries*
sort of neuropathy due to stretching,compression, or osteophytes around the
ruled out.8 If a golfer complains of painon attempting to grip a club—especially
wrist—and has pain at the elbow alongwith resisted extension, the physician
cause lateral or medial epicondylitis, and
strenuous activity can bring on a sub-clinical overuse disorder. It would appear
typically precede an episode of conscious
injury. Symptoms begin gradually andbecome noticeable when a patient’s activ-
have suggested that a preexisting patho-logic mechanism must be present for a
this point: paratenonitis, tendonitis, and
tendinosis. Paratenonitis describes an
inflammation of the outer layer(paratenon) of the tendon alone. Ten-dinitis describes the injury that produces
inflammatory repair response within thetendon. Secondary reactive paratenonitis
can be present along with an inflamma-tory response within the tendon. Tendi-nosis describes intratendinous degenera-
ities of daily living or occupational activ-
ities increase the pain. If the golfer states
Ⅵ “How long have you noticed the with clinically palpable nodules. This
that the pain only occurs during or imme-
diately after playing golf, ask the ques-
tion, “At what point in your golf swing
Physical examination
or later that evening?” Other basic ques-
tions should be asked, including the fol-
Ⅵ “Is your pain sharp or dull? Constant of the musculoskeletal system, it is wise
Ⅵ “How and when did the symptoms game or only afterward?”8
Ⅵ “If your injury is believed to be acute, or any other visible abnormality. Next,
Ⅵ “Was the elbow twisted, struck, or exactly what was occurring when you palpate the elbow to identify tenderness,subjected to shearing forces?”
Ⅵ “Did you fall on your elbow or your Ⅵ “What treatment have you attempt- of the patient’s complaint of pain, andoutstretched hand?”
Ⅵ “What position was your elbow in Ⅵ “Has your pain caused you to alter question. This region should be palpat-when the injury occurred? Was it flexed
your swing or stop playing altogether?”
510 • JAOA • Vol 101 • No 9 • September 2001
gresses gradually to more vigorous pal-pation. In my practice, I find it useful to
Amateur Golf Injuries*
on a scale of 0 to 4, with 0 being no pal-pable tenderness and 4 being extreme
returns for subsequent visits. Compareany findings of swelling, deformity, and
the uninvolved elbow. Make sure to eval-uate the shoulder and wrist of the
looked by dwelling only on the elbow.
swollen joint. Obvious swelling in anelbow is most often caused by posttrau-
mal range of motion for that patient. Normally, elbows have a valgus angle
between the two arms is 5Њ (particularlyin children), one should consider a
ditions that impair extension includehumeral hypertrophy (blocking the ole-
cranon from entering the trochleargroove) and contracture of the forearmmuscles.8 Far and away the most com-
space suggests injury to the radial nerve;
sion, however, is contracture of the elbow
lack of full flexion of the elbow is caused
Diagnosis and diagnostic studies
approximately 30Њ to 40Њ of flexion—to
determine stability. Gapping of the medi-
range of motion, if there is gapping of the
medial joint line, if there is obvious defor-
mity or severe swelling, or if the elbow is
both. This is not an uncommon injury.
percuss the ulnar nerve in this region to
even for a very limited range of motion.
check for Tinel’s sign (tingling at the fin-
the elbow is rare. If range of motion tests
noted, “Weakness of finger extension or
obtain plain radiographs. If negative, pal-
JAOA • Vol 101 • No 9 • September 2001 • 511 Treatment and rehabilitation Mechanisms of Injury
condylitis is far and away the most com-mon elbow injury among amateur
Professional
golfers. Treatment includes rest, ice,compression, and elevation; nonsteroidal
muscle-tendon strengthening within thelimits of pain; tennis elbow strap to
continue; physical therapy; corticos-teroid injections; and measures to pre-
times daily during the acute phase ofthe injury. Rest includes the avoidance of
all activities that significantly increase
the pain in the injured region, includingexcessive wrist motion and hard grip-
usually necessary in cases of lateral epi-condylitis because of the lack of edema. As soon as lateral epicondylitis is diag-nosed, NSAIDs should be prescribed to
ered to be epiphyseal avulsion injuries.
0.5 and 1.0 cm is acceptable if the elbow
get bilateral films. Significant fractures,
is otherwise stable. It is generally believed
that any displacement over 1.0 cm is sig-
lems), neurologic injuries, severe intra-
daily to increase patient compliance.
articular swelling, signs of infection, or
red—especially in the presence of nearby
nance imaging provide for excellent meth-
abrasions, small lacerations, or puncture
soft tissue injuries. A good magnetic res-
out infection is to aspirate fluid from the
joint for Gram stain and culture and sen-
the need for surgery if no fracture, soft tis-
sitivity. When aspirating, be careful not
should “place less emphasis on rest for
sue disruption, spurs, or loose bodies are
to leave a large tract, especially on the tip
infection. In the elbow, infected fluid is
ble the next day, ideally.” They further
imaging has made these studies practically
usually clear and low in viscosity, rather
state that “casting is almost never used
obsolete. Bogard and others8 believe that
than yellowish.8 If infection is suspected,
for fractures or dislocations in elbows.”8
otics (with indications for skin and soft
tissue infection), such as cefadroxil mono-
within the limits of pain is a basic tenet
the acute phase has ended, application of
512 • JAOA • Vol 101 • No 9 • September 2001 Figure 1. A fun- damentally sound golf swing.
decrease muscle spasm and stiffness.
growth plate pathology and “by giving a
Ultrasound therapy also is useful because
bility of tissue while also decreasing pain
resis is by far the most useful modality.
ing grip strength but also includes stretch-
ing exercises for the extensor flexor mus-
treatment for adolescents is rest, ice, and
scribed so far fail to relieve pain, partic-
ularly if there is point tenderness direct-
cians prefer to use an oral corticosteroid
Figure 3. Physical therapy should be pur-
a chance of achieving a “cure” than do
Figure 2. Medial epicondylitis affecting the right elbow is most likely caused bysudden impact loading, such as can occurby taking repetitive strokes that leave
Kenilworth, NJ) because it is easily inject-
A “tennis elbow” strap can be used if
eral epicondyle on the belly of the exten-
certain activities that cannot be discon-
sor carpi radialis brevis (Figure 4).
allows activity to a certain level and can
ate a new “origin” of the muscle that
shortens the length of the overall muscle’s
patient complain of the “steroid flare”
nism of the tennis elbow strap is to cinch
ture to a point that the forced contraction
found that force to the forearm extensors
used in the studies, however, effectively
any golf activities or other vigorous activ-
decreases in lateral tennis elbow and force
to the forearm flexors decreases in medi-
fore increasing force at the elbow,11 mak-
al tennis elbow. The most effective strap
ing wrist braces counterproductive in the
somewhat from clinician to clinician, but
mit, NJ), which has an inflatable air sack
effective is to have the patient sit with
that is placed 1.5 inches distal to the lat-
fully and judiciously in children, as the
JAOA • Vol 101 • No 9 • September 2001 • 513
Clancy and Hagan10 believe there is nogood evidence that injection adjacent totendons, into the surrounding sheath andparatenon, causes injuries to the tendon. It is unclear if steroid injections causeabnormal healing effects with regard totendons; however, they may block a“protective” inflammatory response,making the patient more susceptible to aspontaneous tendon rupture.10 I do notbelieve that it is ever a good policy toinject a tendon or the area immediatelyaround a tendon unless all else fails—and never in a weight-bearing joint.
has been effective in some cases of later-al epicondylitis. The manipulation, ac-cording to Steiner, consists of “soften-ing the muscles of the forearm and thenlocating proximal lesions such as the del-toid, trapezius, and cervical musculaturewhich may have contracted, splintingthe articulations in the process of pro-tecting the inflamed joints. Manipula-tion releases the splinted joints and con-
Figure 3. Common exercises for diminishing the inflammatory response.
tributes to normalization of function.”14I am aware of some high-velocity, low-
down, resting on the examination table.
tion—after I have noted my injection site
condylitis, but I do not believe that this
type of manipulation is effective for this
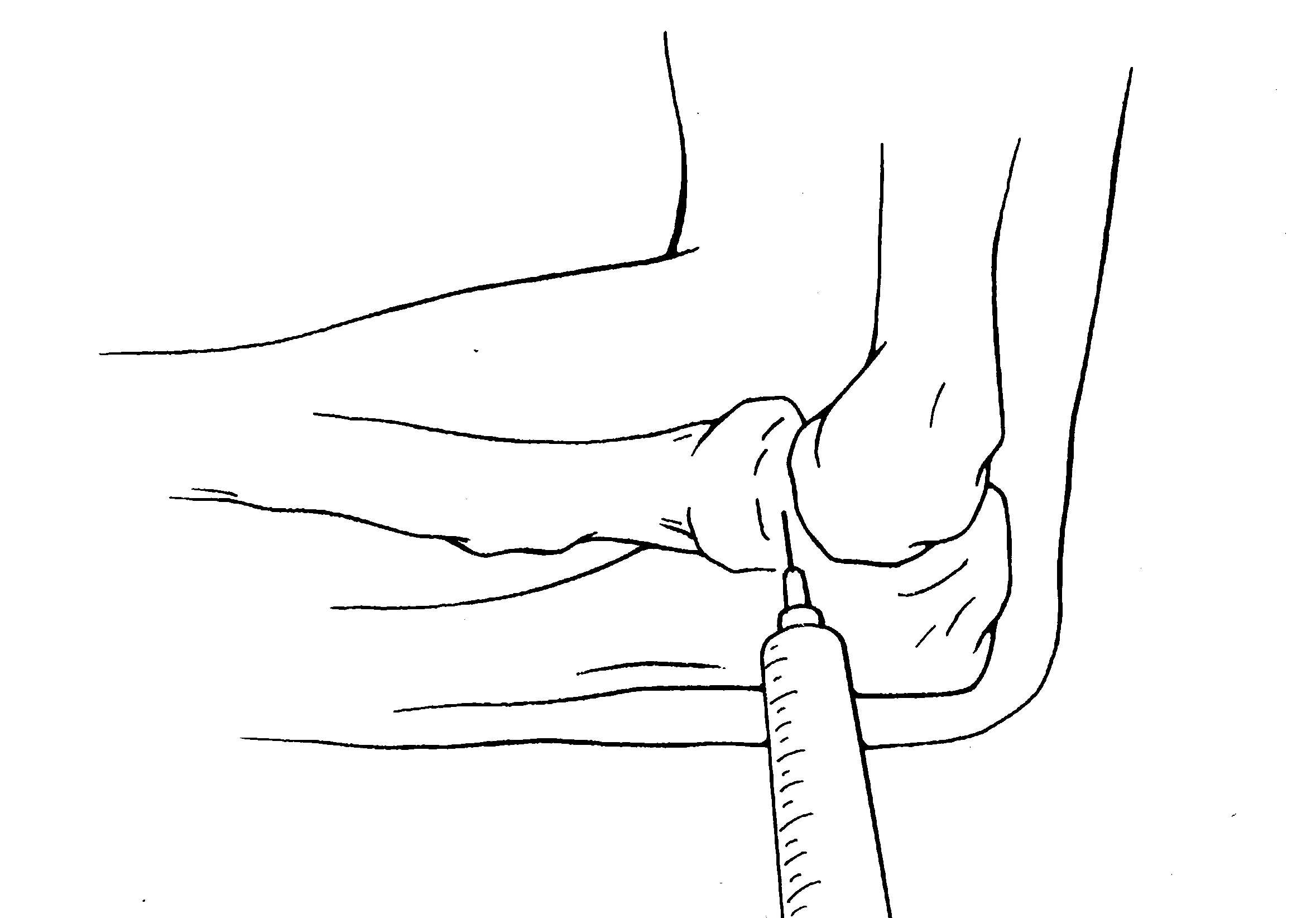
process of the ulna (Figure 5). Using a
resistance; after aspiration is negative for
specific condition. It may be effective for
0.5” to 1” needle, insert perpendicular to
radial head subluxation, or “nursemaid’s
effortless—again with no resistance.
ing the injection of tendons themselves. Figure 4. Proper placement of tennis elbow support. The inflat- Figure 5. Site of steroid injection for lateral epicondylitis. able air sack is placed 1.5 inches distal to the lateral epicondyleon the belly of the extensor carpi radialis brevis.514 • JAOA • Vol 101 • No 9 • September 2001 Figure 6. Shoulder and elbow exercises. Figure 7. Shoulder and elbow stretches with weights or assistance.
ment has failed to be helpful for at least
tures, as well as grade I or II ulnar col-
lateral ligament sprains, can be treated in
recurrence of the injury in the future.
teroid injections. Obviously, surgery might
the office with initial immobilization in
Prevention
bodies, avulsion fracture, or other degen-
(range of motion within the limits of pain
Most golf injuries can be prevented by the
films or magnetic resonance imaging.
ics, which makes it less likely that he or
stated before, lateral compression injuries
she will develop overuse injuries. Proper
“golfer’s elbow,” is usually treated con-
servatively, as in lateral epicondylitis.
golf professional, during multiple lessons,
until the swing has become “grooved.”
tween the two conditions is that the medi-
ics, hitting 250 golf balls in an afternoon
never be injected with corticosteroids.
valgus stresses that can lead to rupture of
the ulna collateral ligament. Prevention of
non fossa. This is also generally treated
medial epicondylitis requires altering the
conservatively, but surgical intervention
is often necessary to restore full range of
assistance of a golf professional in this
elbow injuries. Proper conditioning before
regard), and, obviously, not making large
ovitis is usually treated conservatively,
repetitively swinging a golf club involves
divots when attempting to hit the ball. As
like lateral epicondylitis, except that injec-
with lateral epicondylitis, surgical inter-
is free of pain, full range of motion has
JAOA • Vol 101 • No 9 • September 2001 • 515 Comments 7. Plancher KD, Minnich JM. Sports-specific
minutes of general stretches, a few jump-
Elbow injuries in golf, while not as preva-
injuries. Clin Sports Med 1996;15:207-218. 8. Bogard S, et al. Elbow: keep the whole arm
in focus. Patient Care 1992; Feb. 29.
point, which should be static and involve
treated by the primary care physician. 9. Curl WW. Office treatment of elbow injuries in the athlete. Instr Course Lect 1994;43:55-61.
tive treatment, particularly if formal phys-
10. Clancy WG Jr, Hagan SV. Tendinitis in
therapist or an athletic trainer. Because
golf. Clin Sports Med 1996;15:27-35.
10 seconds, performing three to five rep-
11. Harding WG, Warren G. Use and misuse
etitions. The golfer also could place his or
due to overuse rather than to direct trau-
of the tennis elbow strap. The Physician and
her hands under an object, such as a desk
Sports Medicine 1992;20:65-74.
injury treatment tend to be effective. As
12. Groppel JL, Nirschl RP. Can a joint brace alleviate your pain? Maybe and maybe not!
to hyperextend the elbows more fully.
tion is the best treatment. Therefore, all
neuromuscular facilitation–type stretch. 13. Groppel JL, Nirschl RP. A mechanical and
electromyographical analysis of the effects ofvarious joint counterforce braces on the tennis
player. Am J Sports Med 1986;14:195-200.
mately 10 seconds, with three to five rep-
14. Steiner C. Tennis elbow. JAOA 1976;75:
10 seconds, with three to five repetitions. References 15. Pink MM, Jobe FW, Yocum LA, Mottram 1. McCarroll JR, Gioe TJ. Professional golfers
R. Preventative exercises in golf: arm, leg,
and the price they pay. The Physician and
and back. Clin Sports Med 1996;15:147-162. Sports Medicine 1982;10:54-70.
If lack of flexibility is a recurring prob-
2. Mallon WJ. Ask the doctor [column]. Golf
lem, stretches should be performed daily,
3. McCarroll JR. The frequency of golf injuries.
neuromuscular facilitation–type stretches
(Figure 7). Kohn6 recommends a shortperiod of upper body stretching per-
4. Batt ME. Golfing injuries. An overview. 5. McCarroll JR, Rettig AC, Shellbourne KD.
Injuries in the amateur golfer. The Physician
believes that this best acclimates forearm
and Sports Medicine 1990;18:122-126. 6. Kohn HS. Prevention and treatment of elbow
longer and heavier clubs, while also invok-
injuries in golf. Clin Sports Med 1996;15:65-83.
ing muscle memory of the previouslylearned “grooved swing.” Probably acombination of these two types of stretch-ing/warm-up would be ideal.
be overemphasized. A golf pro shouldhelp each golfer assess his or her grip sizeas well as length of clubs. New golf tech-nology has developed cavity-backed ironsthat lessen the vibration of off-center hits. Also available are oversized irons andwoods that give a greater “sweet spot” orhitting area. Graphite shafts fitted to theindividual golfer’s size and swing speedoffer a truer flight of the ball with dimin-ishment of vibrations, thus reducing thepossibility of overuse injuries.6
516 • JAOA • Vol 101 • No 9 • September 2001
Introduction Over the last 20 years, scholars have devoted considerable attention to the ability of farmers, fishermen, pastoralists and other types of resource users to organize, adopt, monitor and enforce institutional arrangements that govern their use of common pool resources (CPRs) in a sustainable manner (Ostrom et al ., 2002). During this period, progress has been made in carefully iden
DOSAGE FORMS AND STRENGTHS A long-term open-label extension study of subjects from the two short-term efficacy studies was also conducted 12.2 Pharmacodynamics in which subjects were treated with 3900 mg/day for up to 5 days during each menstrual period for up to Tranexamic acid, at in vitro concentrations of 25 - 100 M, reduces by 20 - 60% the maximal rate of plasmin lysis (tranexamic a
 Figure 1. A fun-
Figure 1. A fun-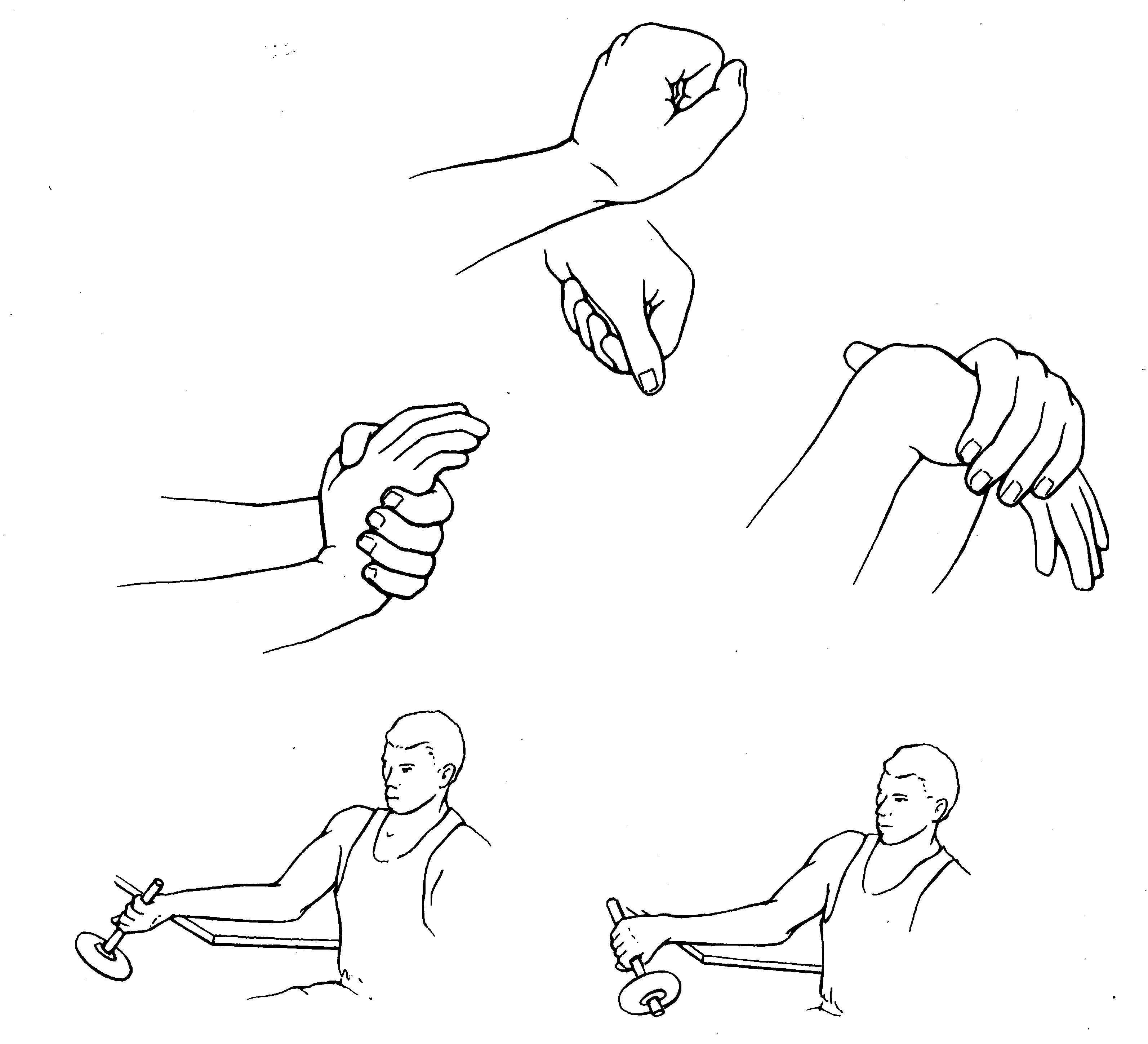

 Clancy and Hagan10 believe there is nogood evidence that injection adjacent totendons, into the surrounding sheath andparatenon, causes injuries to the tendon.
Clancy and Hagan10 believe there is nogood evidence that injection adjacent totendons, into the surrounding sheath andparatenon, causes injuries to the tendon.
 Figure 6. Shoulder and elbow exercises.
Figure 6. Shoulder and elbow exercises.