Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
Doi:10.1016/s0967-5868(03)00010-9
Journal of Clinical Neuroscience (2003) 10(3), 338–339ª 2003 Elsevier Science Ltd. All rights reserved. doi:10.1016/S0967-5868(03)00010-9
Treatment of painful peripheral neuroma by vein implantation
R.J. Mobbs BSc(MED) MB BS, M. Vonau MB BS FRACS, P. Blum MB BS FRACS
Department of Neurosurgery, Institute of Neurological Sciences, The Prince of Wales Hospital, Sydney, Australia
Summary Painful neuromas form on cutaneous nerves as a result of trauma, pressure, stretch or entrapment. Since the earliest descriptionsof neuromas, proposed treatments have been met with poor results and controversy. The myriad of treatments described include: simpledivision of an affected nerve, implantation into muscle or bone, silicon sleeves and caps, repeated injection of steroids, end-to-side neuro-rrhaphy, medication and vein caps to name a few. Due to encouraging recent reports of treatment of painful neuromas by vein implantation, theauthors describe a simple technique to achieve this surgical goal. As veins are readily accessible due to their proximity in the neurovascularbundle, they serve as a ready source for grafting. The advantages include minimisation of trauma to bone and muscle as compared withprevious treatment techniques and the relative ease of the method. ª 2003 Elsevier Science Ltd. All rights reserved.
Painful neuromas form on cutaneous nerves as a result of trauma,
The authors have trialed several techniques for nerve implantation
pressure, stretch or entrapment. In addition, neuromas can be
into a vein including a single and dual incision approach. With the
psychologically incapacitating with resulting reduction in quality
single incision technique, the vein is clamped and divided with an
of life. Since the earliest descriptions of neuromas, proposed
open ending. The nerve is then inserted into the open end and
treatments have been met with poor results and controversy.
sutured closed with an appropriate sized non-absorbable suture.
Furthermore the issue of compensation and litigation complicate
The clamp is then removed. This technique is similar to that de-
outcomes. The myriad of treatments described include: simple
scribed by Herbert and Filan.10 The problem that the authors en-
division of the affected nerve, implantation into muscle or bone,1
countered was that the nerve may retract and pull out of the vein,
silicon sleeves and caps,2 repeated injection of steroids,3 end-to-
leading to failure and potential re-neuroma formation. Thus a dual
side neurorrhaphy,4 medication5 and vein caps6 to name a few.
anchoring technique has been developed to help reduce tension on
The physiology of neuroma formation and subsequent axonal
hyperexcitability is being studied and increasingly understood.
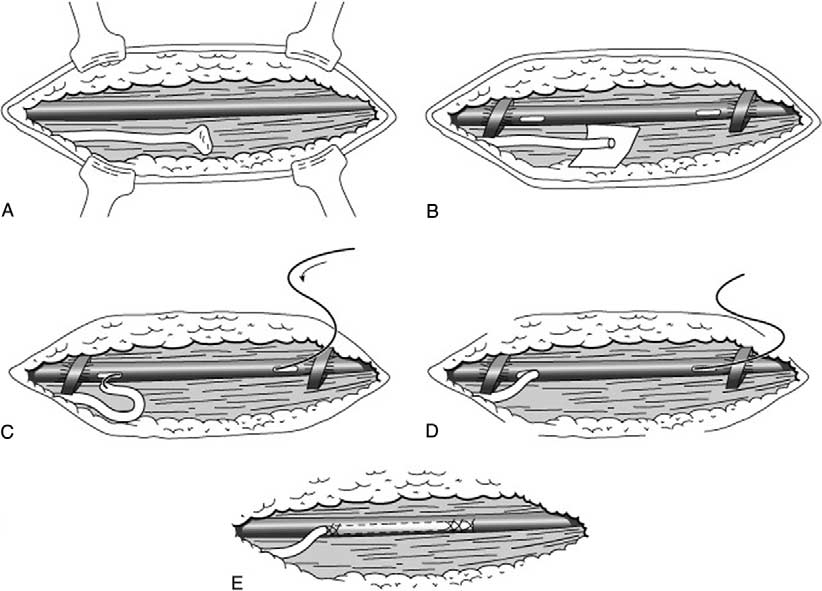
Figs. 1A–E describe the sequence of events of the technique.
Sodium channels accumulate abnormally within the axons of
An appropriate incision is performed to expose the neuroma and
neuromas and this alteration may underlie the generation of
an adjacent normal length of nerve. A vein is next located if
hyperexcitability with resulting abnormal sensory phenomena.7
possible (Fig. 1A). Following excision of the neuroma to a normal
Methods to minimise neuroma formation and axonal hyperexcit-
segment of nerve, the surgeon clamps an adjacent vein at a
ability are however not as well understood, thus the countless
proximal and distal location (Fig. 1B). A small longitudinal slit is
reported techniques to find a solution.
made at either ends of the exposed vessel. A suture is fed up the
In a review of the literature, there is one randomized control
vein from distal to proximal to attach the nerve and pull through
trial investigating the issue of which treatment method is of most
(Figs. 1C and D). Once the nerve is fed through the vein it should
value. Amputation stumps from neuroma removal were capped
be checked to make sure no excessive tension is on the nerve that
with epineural ligature, epineural flaps or an epineural graft, with
may result in failure of the technique. The slit incisions on the
each technique used on 16 nerve endings. Epineural grafts were
vein are closed making sure that the suture picks up some epi-
significantly more effective in preventing neuroma pain in this
neurium to hitch the nerve within the vein (Fig. 1E).
study group.8 In a study of 78 neuromas, Dellon1 trialed im-plantation of neuromas into muscle bulk, stating an overall ex-cellent result of 82% with a mean follow-up of 31 months. The
interest in vein implantation follows several case reports, a de-
The choice of treatment for painful peripheral nerve neuroma
tailed clinical study and a laboratory study.9 The clinical study
depends on the surgeonÕs experience and what they have at-
involves 14 patients with 79% of patients symptom free and the
tempted previously with success. Although the literature does not
rest with minor residual symptoms, with a follow-up at 15
give us a definitive answer on the technique of choice, vein im-
plantation has received many encouraging anecdotal reports andsuccessful short series reports. The simple technique describedhere helps answer the problem of failure that previous authorshave encountered with vein implantation.
Dellon AL, Mackinnon SE. Treatment of the painful neuroma by neuroma
Correspondence to: Dr. R.J. Mobbs BSc(Medc) MB BS, Department of
resection and muscle implantation. Plast Reconstr Surg 1986; 77(3): 427–438.
Neurosurgery, 3 Wansey Road, Randwick NSW 2031, Australia.
Swanson AB, Boeve NR, Lumsden RM. The prevention and treatment of
Tel.: +61-2-9398-7358; Fax: +61-2-9310-0319;
amputation neuromata by silicone capping. J Hand Surg [Am] 1977; 2(1):
Operative sequence for vein implantation.
Smith JR, Gomez NH. Local injection therapy of neuromata of the hand with
England JD, Happel LT, Kline DG, Gamboni F, Thouron CL, Liu ZP, Levinson
triamcinolone acetonide. A preliminary study of twenty-two patients. J Bone
SR. Sodium channel accumulation in humans with painful neuromas.
Al-Qattan MM. Prevention and treatment of painful neuromas of the superficial
Yuksel F, Kislaoglu E, Durak N, Ucar C, Karacaoglu E. Prevention of painful
radial nerve by the end-to-side nerve repair concept: an experimental study and
neuromas by epineural ligatures, flaps and grafts. Br J Plast Surg 1997; 50(3):
preliminary clinical experience. Microsurgery 2000; 20(3): 99–104.
Rizzo MA. Successful treatment of painful traumatic mononeuropathy with
Low CK, Chew SH, Song IC, Ng TH. Implantation of a nerve ending into a
carbamazepine: insights into a possible molecular pain mechanism. J Neurol
vein. Clin Orthop 2000;(379): 242–246.
Herbert TJ, Filan SL. Vein implantation for treatment of painful cutaneous
Chiu DT, Wu J. Treatment of painful neuromas: a case report. Ann Plast Surg
neuromas. A preliminary report. J Hand Surg [Br] 1998; 23(2):
ª 2003 Elsevier Science Ltd. All rights reserved.
Journal of Clinical Neuroscience (2003) 10(3), 338–339
Reporter's Notebook: German Drug Firm Provides Cipro Ever since Tom Brokaw ended a newscast with the words, "In Cipro we trust," this brand of antibiotic has been on every American's lips. And so has "Bayer," the German company that makes the drug. Bayer (pronounced in German like the English word "buyer") has been a household name since the early 1900s when the f
www.rsc.org/pps | Photochemical & Photobiological Sciences A simple procedure for the photoregulation of chymotrypsin activity Stephen Thompson,* Marie-Claude Fawcett, Lesley B. Pulman and Colin H. Self* Received 25th October 2005, Accepted 9th January 2006 First published as an Advance Article on the web 19th January 2006 DOI: 10.1039/b515146e A convenient and rapid method for
 Operative sequence for vein implantation.
Operative sequence for vein implantation.