Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
Microsoft word - mann1.doc
9th Annual Conference of the International FES Society
A Pilot Study to investigate the effects of Functional Electrical
Stimulation on gait in Parkinson’s Disease
Mann GE 1, Finn SM 1, Taylor PN 1
1 Department of Medical Physics & Biomedical Engineering, Salisbury District Hospital, Salisbury,Wiltshire SP2 8BJ. Abstract 1 Introduction Parkinson’s Disease (PD) is a progressive
Parkinson’s Disease (PD) is a progressive
neurological condition resulting in motor
neurological condition which gives rise to
and functional disability. Walking
motor and functional disability as a result of
becomes slower, and frequently a
reduced production of the neurotransmitter,dopamine, through degeneration of the basal
shuffling gait develops with reduced stride
ganglia and substantia nigra. Parkinson’s
length and cadence. There are difficulties initiating and maintaining movement and an increased incidence of falls. Ten
slower, with reduced stride length and cadence
subjects with idiopathic PD were recruited
giving rise to a shuffling gait. As the disease
to the 16 week study. Following a 4 week
progresses there are difficulties initiating and
baseline period each subject received Functional Electrical Stimulation (FES)
blocks (freezing), which occur particularly in
for 8 weeks to the common peroneal nerve
confined spaces. Symptoms may be relieved by
of the more severely affected side.
Levodopa - based drugs, which increase the
Stimulation was withdrawn for the
amount of dopamine in the body. These drugs
following 4 weeks. Assessments were
become less effective as the disease progresses
made of stride length, time and number of steps to complete a 20 metre walk with a Effect of External Cues turn and walking distance over 3 minutes.
There is evidence that external ‘cues’– visual,
Episodes of ‘freezing’ and quality of life
auditory, cognitive or sensory, may be able tocompensate for the defective internal ‘cueing
measures were also recorded. Each subject kept a falls diary.
movement, usually facilitated by dopamine
Results indicate that there is no immediate orthotic effect of electrical stimulation on 1 . 2 T h e O d s t o c k D r o p p e d F o o t gait but that there is a significant learning Stimulator effect on unstimulated walking at the end of the trea tm ent per iod wh ich is
The Odstock Dropped Foot Stimulator (ODFS)
maintained for at least a month after
is a single channel footswitch controlled
stimulation has been withdrawn.
neuromuscular device used to correct droppedfoot during walking. Stimulation is applied tothe
dorsiflexion and eversion during the swingphase of walking. Study hypothesis It is hypothesised that use of electrical stimulation of the common peroneal nerve in patients with PD may act to provide an appropriate external sensory cue to maintain or improve the normal gait pattern and reduce episodes of ‘freezing’ during gait.
9th Annual Conference of the International FES Society
2 Methods
10 subjects, 6 male and 4 female, aged 41 to 80
Subjects
years (mean = 66.7) and PD of 2 to 25 years(mean = 8.7) duration were recruited to the
10 subjects with Parkinson’s Disease who were
study. Three were excluded as their primary
problem was a dropped foot rather than more
recruited to the study. Each subject exhibited
commonly recognised symptoms of idiopathic
reduced stride length and heel strike during gait
and most experienced both motor blocks andepisodes of falling.
Subjects required significantly fewer steps andless time to complete the 20 metre walk at the
Stimulation treatment
end of the treatment period than during the 4
Subjects received single channel FES of the
week baseline period both with and without
common peroneal nerve of the lower limb of
stimulation. This effect was maintained at the
the more severely affected side. Stimulation
end of the follow up period (Tables 1&2). A
was delivered by the Odstock Dropped Foot
similar pattern was seen in the shuffle ratio and
Stimulator (ODFS), a neuromuscular stimulator
step index for the 3 minute walk (Tables 3&4).
powered by a 9 volt battery, producing a train
of pulses of 300 microseconds duration at a
frequency of 40Hz. Stimulation was appliedthrough PALS adhesive electrodes and
assessments Wilcoxon
triggered by a pressure sensitive switch placed
Assessments
The 16 week study period comprised a 4 week
baseline period without stimulation, 8 weeks
with stimulation and a 4 week follow up period
conducted at weeks 0, 2, 4, 8, 12, 14 and 16. Subjects completed a 20 metre walk which
Table 1: Number of steps to complete 20m Walk
included walking through a doorway, turning
and walking back to the start. Two high backed
assessments Wilcoxon
chairs were placed in the walkway as obstacles
to be negotiated. Subjects also completed a
timed 3 minute walk over the same walkway. A
video recording was made of each walk for
Assessments included the motor examination of
the Unified Parkinson’s Disease Rating Scale
(UPDRS), the Mini-Mental State Examination(MMSE), and the PDQ 39 quality of life
Table 2: Time taken to complete 20m Walk With
questionnaire. Subjects completed a falls diary
assessments Wilcoxon
The number and length of steps and time to
complete the 20 metre and 3 minute walks were
recorded with and without stimulation from the
distinguished from the number of shuffling step
movements in which the foot moved forwardbut did not clear the floor. This is referred to as
The average stride length is referred to as the
Table 3: Shuffle ratio – 3 minute walk.
‘step index’. This is the number of steps taken over the distance covered in 3 minutes. 3 Results
9th Annual Conference of the International FES Society
assessments Wilcoxon
effect at all but one stage of the study. It may be
that a greater distance was necessary for the
effect of the stimulation to be shown with such
small number of subjects. This training effect is
reinforced by results showing the benefits to be
maintained to the end of the follow up period
The training effect may have implication for the
way in which stimulation is used in this patient
Table 4: Step index – 3 minute walk
group. Most subjects reported that the devicetrained them to improve gait features such asheel strike and stride length. One user reported
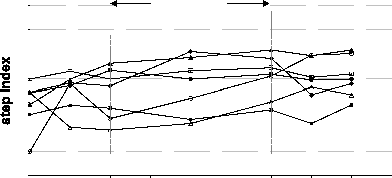
Step index 3 min endurance walk - no stimulation
that the improvement in his unassisted walkingwas maintained through periodic use of the
TREATMENTPERIOD
Subjects may have benefited from the gait re-
education as an adjunct to the study. Further
work is necessary to establish the mechanisms
of the effects of stimulation in patients with PD
and to identify which patients are likely to
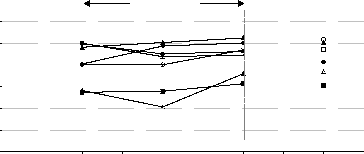
Figure 1: Step index – 3 minute walk, no
maintained for the period of this trial. A trialwith a control group is needed to verify thisconclusion. Step index 3 min endurance walk - with stimulation References TREATMENTPERIOD
Bagley S, Kelly B, Tunnicliffe N, Turnbull
G.I., Walker G.M. The effect of visual cues
Parkinson’s disease. Physiotherapy. 77(6).
facilitation of gait patterns in patient’s withParkinson’s Disease. Journal of Neurology,Figure 2: Step index – 3 minute walk, with Neurosurgery and Psychiatry. 62(1). 22–
4 Discussion and Conclusions
Summers J.J. Ability to modulate walkingcadence remains intact in Parkinson’s
For the results presented in this paper there was
found to be a significant carry over effect at the
Neurosurgery, and Psychiatry. 57. 1532-
Jacobs A.B., Horak F.B., Nutt J.G., Obeso
withdrawn. This agrees with anecdotal evidence
J.A. Step initiation in Parkinson’s Disease:
from study participants who reported that the
stimulator acted as a training device. This
Sensory Triggers. Movement Disorders.
suggests an improvement in stride length and
Acknowledgements
improvement in gait pattern. Interestingly there
The authors acknowledge the Parkinson’s Disease
was no immediate orthotic effect for most of
the 20m Walk With Turn tests at any stage ofthe study. However, the step index for the 3minute walk did reveal an immediate orthotic
JOINT NEUROSURGICAL CONVENTION 2013 –PROGRAM (AS OF JANUARY 17, 2013) TUESDAY, JANUARY 29, 2013 (DAY 1) WEDNESDAY, JANUARY 30, 2013 (DAY 2) General Session 2 - MVD & Spine, Moderated by Izumi Koyanagi. M.D. The preoperative assessment of hemifacial spasm by direct coronal Kiyohiro Houkin, M.D. & Hideyuki Ohnishi, M.D. thin slice heavy T2 MRI, Miki Ohta, M.D. de
Patient Registration Form PLEASE PRINT Title: Mr Mrs Miss Ms Ps Dr (Med) Dr (PhD) Other: ___________________________ Surname: ________________________ Given Names: _______________________________ Date of Birth: / / Occupation: ________________________________________ Home Address: __________________________________ __________________________________ ________
 9th Annual Conference of the International FES Society
assessments
9th Annual Conference of the International FES Society
assessments