Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
Pediatricheartnetwork.org
T h e n e w e ng l a n d j o u r na l o f m e dic i n e
port-wine stains through greater vessel heating The Authors Reply: With ongoing research in
and deeper vascular injury.2 The improved tech- medicine, investigating the 10-year follow-up re-
nology targets the heterogeneity in blood-vessel sults of any medical treatment inevitably leads to
sizes that is characteristic of port-wine stains.3
somewhat outdated results at the time of presen-
Any study evaluating the response of port-wine tation. This is especially the case in a field that is
stains to treatment should include an analysis subject to continuous development, such as pulsed-
based on the location of the anatomical malfor- dye–laser treatment of port-wine stains. As Nelson
mation and the patient’s age. As compared with and Geronemus point out, the results with newer
other areas of the face and neck, port-wine stains pulsed-dye lasers have been reported to be prom-
on the center of the face have been shown to re- ising and superior to the results with the laser
spond less effectively to treatment and are more used in our study. However, to date no controlled
likely to recur.4 An aggressive approach to treat- comparative studies have shown improved clinical
ing infants and young children can also allow for efficacy. Whether the new lasers have improved
long-term efficacy remains to be reported; in
light of our observation of the recurrence of port-
wine stains, we certainly hope they do.
Beckman Laser Institute Irvine, CA 92612
No differences or trends in responses to treat-
ment related to the anatomical locations of the
port-wine stains were observed in either the origi-
nal study1,2 or the current follow-up study, possi-
New York University Medical Center New York, NY 10016
bly because of the relatively small number of pa-
tients. Furthermore, in the original study, age was
1. Huikeshoven M, Koster PHL, de Borgie CAJM, Beek JF, van shown to have no influence on the response to
Gemert MJC, van der Horst CMAM. Redarkening of port-wine
stains 10 years after pulsed-dye–laser treatment. N Engl J Med treatment. Therefore, we refrained from perform-
ing age-dependent analyses in the current long-
2. Nelson JS, Milner TE, Anvari B, Tanenbaum BS, et al. Dy-
namic epidermal cooling during pulsed laser treatment of port
wine stain: a new methodology with preliminary clinical evalu- Menno Huikeshoven, M.D., Ph.D.
ation. Arch Dermatol 1995;131:695-700.
Chantal M.A.M. van der Horst, M.D., Ph.D. 3. Barsky SH, Rosen S, Geer DE, Noe JM. The nature and evolu-
tion of port wine stains: a computer-assisted study. J Invest Der- Academic Medical Center
4. Renfro L, Geronemus RG. Anatomical differences of port-
wine stains in response to treatment with the pulsed dye laser. 1. van der Horst CMAM, Koster PHL, de Borgie CAJM, Bossuyt
PMM, van Gemert MJC. Effect of the timing of treatment of port-
5. Geronemus RG, Quintana AT, Lou WW, Kauvar A. High-flu-
wine stains with the flash-lamp–pumped pulsed-dye laser.
ence modified pulsed dye laser photocoagulation with dynamic N Engl J Med 1998;338:1028-33.
cooling of port-wine stains in infancy. Arch Dermatol 2000;136: 2. Kauvar AN, Geronemus RG. Treatment of port-wine stains. Treatment of Kawasaki Disease To the Editor: In their trial of pulsed cortico- effect, which could therefore be associated with
steroid therapy for primary treatment of Kawa- a secondary increase in inflammation.
saki disease, Newburger et al. (Feb. 15 issue)1
On the basis of nearly 10 years of clinical
report that, as compared with placebo, a single experience,2 we designed a regimen involving a
pulsed dose of corticosteroid resulted in a shorter short intravenous course of prednisolone and
initial period of hospitalization but that the total subsequent oral administration of prednisolone
numbers of days of fever and hospitalization, the followed by tapering.3 In a randomized trial per-
rates of retreatment, and the coronary-artery out- formed to test the effectiveness of the regimen
comes did not differ significantly between the two as an adjunct to intravenous immune globulin,
groups. The use of a single-dose regimen without the incidences of retreatment and coronary-artery
tapering most likely contributed to their results. abnormalities within 1 month after the start of
A single application of a corticosteroid, even at a treatment were less frequent in the corticosteroid
high dose, may have a strong but only short-lived group than in the group receiving immune globu-
n engl j med 356;26 www.nejm.org june 28, 2007
Downloaded from www.nejm.org at HARVARD UNIVERSITY on July 26, 2007 .
Copyright 2007 Massachusetts Medical Society. All rights reserved.
lin alone. Our regimen therefore appears to be Andrea Taddio, M.D.
more efficacious than the control regimen. Never- Institute of Child Health
theless, the optimal corticosteroid regimen re- 34100 Trieste, Italy
mains an issue in the primary therapy of Kawa-
Carlos D. Rosé M.D. Thomas Jefferson University
1. Hashino K, Ishii M, Iemura M, Akagi T, Kato H. Re-treat-
ment for immune globulin-resistant Kawasaki disease: a com-
Gunma University Graduate School of Medicine
parative study of additional immune globulin and steroid pulse
2. Lang BA, Yeung RS, Oen KG, et al. Corticosteroid treatment
of refractory Kawasaki disease. J Rheumatol 2006;33:803-9. 1. Newburger JW, Sleeper LA, McCrindle BW, et al. Random- 3. Sundel RP, Baker AL, Fulton DR, Newburger JW. Corticoste-
ized trial of pulsed corticosteroid therapy for primary treatment roids in the initial treatment of Kawasaki disease: report of a
of Kawasaki disease. N Engl J Med 2007;356:663-75.
randomized trial. J Pediatr 2003;142:611-6. 2. Shinohara M, Sone K, Tomomasa T, Morikawa A. Cortico-
steroids in the treatment of the acute phase of Kawasaki disease.
To the Editor: Although the study by Newburger 3. Inoue Y, Okada Y, Shinohara M, et al. A multicenter prospec-
tive randomized trial of corticosteroids in primary therapy for et al. involved assessment of coronary-artery out-
Kawasaki disease: clinical course and coronary artery outcome. comes with the use of transthoracic echocardi-
ography, we were quite surprised by the inclusion
of an example of a coronary aneurysm seen on
To the Editor: Newburger et al. studied the ef- multidetector computed tomography (CT) in the
fects of adding intravenous methylprednisolone to accompanying Perspective article by Burns.1
conventional therapy for Kawasaki disease. The
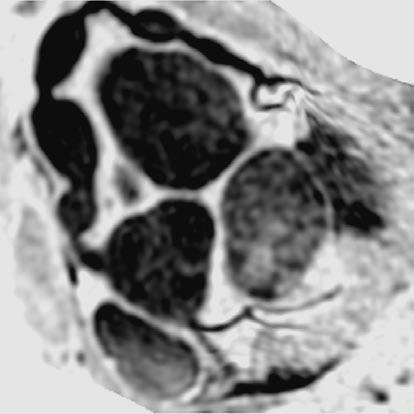
We and others2,3 have shown the efficacy of
authors found a significantly lower frequency of noninvasive magnetic resonance imaging (MRI)
coronary-artery abnormalities in the intravenous- of the heart for both the identification and char-
methylprednisolone group than in the placebo acterization of coronary artery disease in patients
group within the subgroup of patients who re- with Kawasaki disease (Fig. 1). Patients with
quired retreatment with intravenous immune Kawasaki disease require frequent observation
over many decades. Given the relatively high doses
The identification of predictors of coronary ab- of ionizing radiation associated with multidetector
normalities in Kawasaki disease is still problem-
atic. Failure of initial treatment with intravenous
immune globulin remains the most consistent
risk factor for cardiac abnormalities.1 Adminis-
tration of intravenous methylprednisolone after
the failure of initial treatment with intravenous
immune globulin does not seem to be effective in
reducing the risk of coronary damage,2 although
the current data suggest that this might not be the
case for patients who do not have a response to
intravenous immune globulin and who have pre-
viously received intravenous methylprednisolone.
Since intravenous methylprednisolone admin-
istered as a single dose appears to be safe,3 and
given our inability to identify a priori the patients
who will not have a response to intravenous im-
mune globulin, it seems obvious that the concur-
rent use of a single dose of intravenous methyl-
prednisolone and intravenous immune globulin
Figure 1. Three-Dimensional Steady-State Free-Precession
may be our best choice at the moment. It is un-
MRI of the Whole Heart in an 8-Year-Old Boy with Kawasaki Disease and Serial Aneurysms (A) in the
realistic to expect that trials powered to show
Right Coronary Artery.
the effectiveness of intravenous methylpredniso-
No contrast material was administered.
lone could be accomplished anytime soon. AUTHOR, PLEASE NOTE: Figure has been redrawn and type has been reset. Please check carefully.
Downloaded from www.nejm.org at HARVARD UNIVERSITY on July 26, 2007 .
Copyright 2007 Massachusetts Medical Society. All rights reserved.
T h e n e w e ng l a n d j o u r na l o f m e dic i n e
CT 4 and the heightened potential for radiation- therapy, findings that have been shown to be er-
induced fatal cancer in children,5 we believe that, roneous in subsequent prospective trials.2 Chil-
if transthoracic echocardiography is inadequate, dren with Kawasaki disease can be characterized
these younger patients are best served by the use at the time of presentation with respect to their
risk of resistance to intravenous immune globu-
lin.3 Until further studies are conducted in high-
risk patients, we do not believe that corticosteroid
therapy should be used in the primary treatment
1. Burns JC. The riddle of Kawasaki disease. N Engl J Med jane.newburger@cardio.chboston.org 2. Greil GF, Stuber M, Botnar RM, et al. Coronary magnetic
resonance angiography in adolescents and young adults with New England Research Institutes
Kawasaki disease. Circulation 2002;105:908-11. 3. Mavrogeni S, Papadopoulos G, Douskou M, et al. Magnetic 1. Pfeffer MA, Jarcho JA. The charisma of subgroups and the
resonance angiography, function and viability evaluation in pa- subgroups of CHARISMA. N Engl J Med 2006;354:1744-6.
tients with Kawasaki disease. J Cardiovasc Magn Reson 2006;8: 2. Rothwell PM. Treating individuals 2: subgroup analysis in
randomised controlled trials: importance, indications, and inter-
4. Coles DR, Smail MA, Negus IS, et al. Comparison of radia-
tion doses from multislice computed tomography coronary angi- 3. Kobayashi T, Inoue Y, Takeuchi K, et al. Prediction of intra-
ography and conventional diagnostic angiography. J Am Coll venous immunoglobulin unresponsiveness in patients with Kawa-
saki disease. Circulation 2006;113:2606-12. 5. Brenner D, Elliston C, Hall E, Berdon W. Estimated risks of
radiation-induced fatal cancer from pediatric CT. AJR Am J
Dr. Burns Replies: Imaging of the coronary ar-
teries is important in the long-term management
The Authors Reply: Inoue and colleagues de- of aneurysms in patients with Kawasaki disease.
scribe the results of their open trial using a pro- Transthoracic echocardiography can be used only
longed course of corticosteroids, which we discuss to image the proximal arteries, is dependent on a
in our article. We found that clinically significant high level of technical skill, and cannot reliably
coronary-artery abnormalities were infrequent in detect stenosis. Advantages of multidetector CT
patients in both of our study groups. For this are the assessment of calcification and soft plaque,
reason, although the optimal corticosteroid regi- rapid collection of data, and straightforward in-
men may be unknown, we believe that cortico- terpretation of images. With proper gating to the
steroid regimens requiring a prolonged course of cardiac cycle and lowering of the heart rate with
treatment would be difficult to rationalize for the beta-adrenergic blockade, exposures of approxi-
primary treatment of all patients with Kawasaki mately 0.67 mSv have been documented for coro-
nary-artery studies of children involving multi-
Taddio and Rosé highlight an important ques- detector CT (Larkin G, GE Healthcare: personal
tion arising from our analyses. Our study was de- communication) (for comparison, one chest radio-
signed to test the hypothesis that the addition of graph results in exposure to 0.02 mSv). MRI is safe,
intravenous methylprednisolone to conventional but many centers cannot image the coronary ar-
primary treatment of Kawasaki disease would im- teries with sufficient precision. All these ap-
prove coronary-artery outcomes; the study groups proaches require general anesthesia for young
had similar overall coronary outcomes. A post hoc patients, and MRI requires a longer time to cap-
subgroup analysis suggested that primary cortico- ture images than does multidetector CT and thus
steroid therapy reduced the incidence of coronary- increases the time under anesthesia and associat-
artery abnormalities in a high-risk subgroup of ed risks. Clearly, this is an area of medicine that
patients in our study who required retreatment is in flux. We look forward to the time when safe,
with intravenous immune globulin because of noninvasive imaging methods are widely avail-
persistent or recrudescent fever. However, such able at all centers for these children.
subgroup analyses must be interpreted with cau- Jane C. Burns, M.D.
tion1; the literature is replete with subgroup University of California, San Diego
analyses suggesting differential responses to La Jolla, CA 92093-0830
n engl j med 356;26 www.nejm.org june 28, 2007
Downloaded from www.nejm.org at HARVARD UNIVERSITY on July 26, 2007 .
Copyright 2007 Massachusetts Medical Society. All rights reserved.
MRSA in Schools Methicillin-resistant Staphylococcus aureus (MRSA) is a form of Staphylococcus aureus, a common bacterium that has developed resistance to several forms of antibiotics. MRSA has been around for many years, mostly in health care settings but has moved into the community in recent years. Infections can be seen anywhere but are mostly seen in settings where people have close cont
TONGUE PIERCING AFTERCARE A piercing is healed by your body, not by the cleaning agents you put on it. Aftercare helps your body be in an optimum state for healing. This meanskeeping the area clean and free of contaminants. Independent of the care you give thepiercing, you should eat well and be well rested to help your body heal. A healthy dietincluding a multivitamin with up to 3000 mg. of
 lin alone. Our regimen therefore appears to be Andrea Taddio, M.D.
lin alone. Our regimen therefore appears to be Andrea Taddio, M.D.