Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
Doi:10.1016/s0140-6736(96)09070-8
George H Elder, Richard J Hift, Peter N Meissner
Public attention has been drawn to the acute porphyrias
in the past few years by speculation that they affected thecharacter of George III and the creative genius of Vincent
Acute intermittent porphyriaAutosomal dominant; acute attacks only; no cutaneous
van Gogh. During the same period, there have been
manifestations. Three families with homozygous/compound
important advances in the understanding of the molecular
basis of the acute porphyrias and in diagnosis and theclinical management of patients and their families. Four
Hereditary coproporphyriaAutosomal dominant; acute attacks with skin lesions (blisters,
types of porphyria are classified as acute because they
fragility) in about one-third of patients; skin lesions without acute
produce acute neurovisceral crises (panel).1 Here, we
attacks are rare. Three families with homozygous/compound
outline current knowledge of the three autosomal
dominant types: acute intermittent porphyria, variegate
porphyria, and hereditary coproporphyria.
Autosomal dominant. Of 61 UK patients, 45 (73%) presented withskin lesions (blisters, fragility) alone, seven (12%) with acute
attacks alone, and nine (15%) with both together. 12 families with
homozygous/compound heterozygous variant reported.
The inherited defect in each of the autosomal dominant
5-aminolaevulinic acid dehydratase deficiency porphyria
acute porphyrias is the complete or near complete
Autosomal recessive; presents at any age with severe acute
inactivation of one of a pair of allelic genes that encodes
attacks, neuropathy or both. Four families reported.
for an enzyme of the biosynthetic pathway for haem(table 1).1 The consequent 50% reduction in enzyme
these mutations decrease enzyme activity in all tissues.
activity provokes a compensatory increase in substrate
concentration, which is brought about through the
deaminase has been solved at 0·176 nm resolution and
negative feedback regulation by haem of the rate-
provides a useful model for predicting the functional
controlling initial enzyme of the pathway, 5-
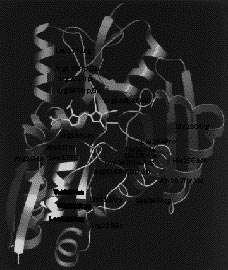
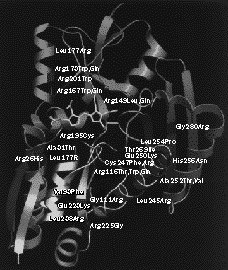
effects of human mutations (figure).6 Most mutations in
aminolaevulinate synthase (ALA-S). Substrate
acute intermittent porphyria are restricted to one or a few
accumulation and increased ALA-S activity in response to
families. However, one mutation (Trp198Stop),
the enzyme deficiency are most prominent in the liver, in
presumably inherited from a common founder, underlies
which haem supply is finely regulated to adjust to internal
the high prevalence of acute intermittent porphyria in
and external stimuli—for example, drugs that induce
northern Sweden (1 per 1500 people). There is no
cytochrome P450s. The increase in synthesis andexcretion of porphobilinogen that characterises the acute
evidence that any specific genotype determines either the
attack reflects primary (acute intermittent porphyria) or
pattern or severity of the acute attack, or major
secondary (variegate porphyria and hereditary
differences in clinical penetrance between families.4
coproporphyria) limitation of the rate of hepatic haem
Preliminary data indicate that variegate porphyria may
synthesis at porphobilinogen deaminase—the enzyme that
be as heterogenous at the DNA level as other porphyrias
has the lowest activity of those that convert
in most countries, with the notable exception of South
Africa. About 10 000 South Africans of Afrikaans descenthave variegate porphyria; genealogical evidence suggeststhat this acute porphyria was inherited from a single
founder, a woman who emigrated from Holland in 1688.7
The porphyrias show extensive allelic heterogeneity.2
These families share the same mutation (Arg59Trp) in
More than 90 mutations that cause acute intermittent
the protoporphyrinogen oxidase gene.8 The existence of
porphyria have been identified in the porphobilinogen
such a large group with the same mutation provides a
deaminase gene.3,4 Mutations in exon 1, which encodes
unique opportunity to study the interaction of other
the additional 17 aminoacids at the N-terminus that
inherited and environmental factors in the acute
distinguish the ubiquitous from the erythroid isoenzyme
of this enzyme,3 are responsible for a rare variant of acute
Homozygous forms of acute intermittent porphyria,
intermittent porphyria in which only the ubiquitous
variegate porphyria, and hereditary coporporphyria, which
isoenzyme is defective.5 Other mutations are distributed
are frequently associated with growth and psychomotor
throughout the gene in exons common to both
retardation, have been reported,1 as has more than one
isoenzymes, with some clustering in exons 10 and 12;
type of acute porphyria in the same individual or family.1,9
Department of Medical Biochemistry, University of Wales College
of Medicine, Heath Park, Cardiff CF4 4XN, UK (Prof G H Elder MD);and MRC/UCT Liver Research Centre, Department of Medicine,
Acute porphyria occurs in all races. In most European
University of Cape Town, Cape Town, South Africa (R J Hift MD,
countries, apart from Sweden, the estimated prevalence of
clinically overt acute porphyria is 1–2 per 100 000
inhabitants.10,11 Most of these individuals have acute
Urine: PBG and ALAFaeces: normal porphyrin ex cretion
Urine: PBG, ALA, coproporphyrin III (acute phase)Faeces: coproporphyrin III
Urine: PBG, ALA (acute phase); coproporphyrin III
Faeces: protoporphyrin IX greater than coproporphyrin IIIPlasma: porphyrin-protein conjugate with fluorescence
PBG=porphobilinogen; ALA=aminolaevulinate.
Table 1: Autosomal dominant acute porphyrias
intermittent porphyria. Variegate porphyria is about one-
opiates frequently lead to unwarranted suspicions of
third as prevalent as acute intermittent porphyria in the
histrionic behaviour or addiction. Yet as the attack remits,
UK; it usually presents with skin lesions alone (panel) and
the need for analgesia disappears, which confirms the
is less often the cause of recurrent attacks. Even in South
Africa, most acute attacks are now caused by acute
Though tachycardia and hypertension are described as
intermittent porphyria. Hereditary coproporphyria is the
features of the acute attack, the pulse rate and blood
pressure are often only moderately raised, and these signs
Gene frequencies for these disorders are higher than the
are of poor diagnostic value. Vomiting and constipation
prevalence of overt cases. Biochemical studies of relatives
are common; the latter is rarely a presenting symptom.
of patients with symptomatic acute porphyria suggest that
These features of acute porphyria—pain, tachycardia,
at least 90% of individuals with acute intermittent
hypertension, and partial ileus—have been attributed to
porphyria or variegate porphyria are clinically latent which
an autonomic neuropathy. Dehydration is common and
gives a frequency of 1–2 per 10 000 individuals for acute
responds rapidly to fluid replacement. Hyponatraemia,
intermittent porphyria. A study by Mustajoki and
probably caused in some patients by inappropriate
colleagues12 showed that screening blood donors for
secretion of vasopressin,1 may also be present. The
inherited porphobilinogen deaminase deficiency gives an
sodium concentration may decline to dangerously low
even higher rate of 1 per 500 donors.12 This prevalence is
levels, which can lead to convulsions.
close to that reported by Tishler et al13 in a similar, but
The severe attack may progress to a motor neuropathy
uncontrolled, study of psychiatric inpatients, which is
which may resemble a Guillain-Barré syndrome. In some
often quoted as evidence of an increased frequency of
patients, onset of the neuropathy may be preceded by
acute intermittent porphyria among such patients. The
disappearance of the abdominal pain, which may lead the
occurrence of homozygous variants, sporadic presentation
physician to erroneously assume that the patient is
of acute intermittent porphyria in about 25% of cases,14
recovering. Mild sensory changes often accompany the
and allelic heterogeneity combined with a low rate of new
motor neuropathy, particularly, a “bathing trunk”
mutations4,14 are all features consistent with a high
distribution of hypoaesthesia over the trunk and thighs. In
prevalence of latent acute porphyria in the population.
milder cases, particularly with repeated attacks of acuteintermittent porphyria, the features are of a distal
Factors that may precipitate the acute attack
neuropathy with foot drop and wrist drop. Occasionally,
Drugs and the menstrual cycle are the most common
sensory or sympathetic features such as dysaethesia or
precipitants of the acute attack,1,10,15,16 and recurrent
causalgia are prominent. Progression to neuropathy is
attacks that occur in the late luteal phase are sometimes a
seen less frequently than in the past (table 2).15 Abnormal
major problem in acute intermittent porphyria. Factors
behaiviour and confusion, with agitation and
such as alcohol, fasting, stress, and infection have also
hallucinations, are common in some patients during the
been implicated. It is impossible to predict accurately
acute attack. There is little evidence that porphyria
whether specific drugs will provoke an acute attack
produces chronic psychiatric illness, apart from
in a particular individual.15 Drugs should be prescribed
only after reference to a drug list,10,16
recommendations are not absolute and do not substitute
for sound clinical judgment. The risk of an attack is
Most difficulties in the diagnosis of an acute attack arise
highest for drugs that are known to have repeatedly
in patients who do not have a family history of porphyria,
provoked acute attacks and for patients who have or have
particularly if the combination of symptoms is atypical. A
high index of clinical suspicion is important to avoiddelayed diagnosis, which may lead to inadvertent use of
contraindicated drugs and a poorer prognosis.
Acute attacks are about five times more common in
Increased urinary excretion of porphobilinogen
women than in men; attacks are most frequent during the
confirms the diagnosis of an acute attack (table 1).
second to fourth decades and are rare before puberty.
Excretion of aminolaevulinate is also increased but to a
Abdominal pain is almost universal in acute porphyria
lesser extent. Screening tests for porphobilinogen based
(table 2). Pain is severe, constant, occurs in any quadrant
on the insolubility of organic solvents of the red product
and commonly in the back, buttocks, and thighs, and may
of its reaction with p-dimethylaminobenzaldehyde in acid
require large amounts of opiates for its control. Pain is
(Ehrlich’s reagent) have been criticised because they lack
sometimes accompanied by guarding, but not by true
sensitivity and produce occasional false-positive results.18
peritonism. The incessant pleas of affected patients for
A positive screening test is useful in an emergency, but
especially in those few patients who become addictedto opiates. In variegate porphyria and hereditarycoporporhyria, porphobilinogen excretion will generallybe normal in the absence of symptoms. In acuteintermittent porphyria, concentratons are often raisedduring the symptomless phase and increase further duringan acute attack.
Pathogenesis of the acute attackIncreased ALA-S activity, overproduction ofaminolaevulinate, and relative haem deficiency in the liverare biochemical featues of all acute porphyrias and also ofthe identical syndrome that occurs in hereditarytyrosinaemia. How these changes are triggered and thepathogenesis of the neuronal dysfunction that producesthe symptoms are little understood.21 Some drugs andalcoholic beverages may increase the intrahepaticrequirement for haem by inducing the synthesis ofcytochrome P450. The mechanisms for other drugs andhormones and the explanation for differences betweenindividuals in their susceptibility to develop acute attacksare not known.15 Investigation of the pathogenesis of theneuropathy has been hampered by lack of an experimentalmodel. Current theories implicate aminolaevulinate as aneurotoxin (for which the evidence is controversial21),neurotransmitter disturbance secondary to deficiency of
Model of human porphobilinogen deaminase with some of the
haem and tryptophan dioxygenase in the liver, or
mutations that cause acute intermittent porphyria
The dipyrromethane cofactor at the active site is shown in yellow. We
development of a transgenic porphobilinogen deaminase
thank N Srinivasan and R Sowdhamini (Birkbeck College, London, UK)for the figure.
deficient mouse provides a system in which thesehypotheses can be tested.22
should always been confirmed by a specific, quantitative
assay.19 A negative screening test does not exclude an
acute attack. If clinical suspicion persists, quantification
Most patients will require admission to hospital. Only
of porphobilinogen and measurement of faecal and
drugs clearly shown to be safe in porphyria should be
plasma porphyrins are essential. Excretion of
prescribed; all others should be withdrawn. Pain will
porphobilinogen may fall below the detection limit of
respond to opiates, though high doses may be required.
screening tests soon after the onset of symptoms,
Sedation with chlorpromazine is often helpful. Vomiting
particularly in variegate porphyria and hereditary
may be suppressed with prochlorperazine or
coporporphyria, and the diagnosis may be missed if this
metaclopramide. Administration of dextrose or laevulose
approach is not followed. The type of acute porphyria is
in large amounts has been shown to suppress synthesis of
established by measurement of faecal and plasma
aminolaevulinate.23 However, intravenous dextrose may
porphyrins (table 1);19 enzyme assays at this stage may
aggravate hyponatraemia and must be used with caution.
mislead and should not be used in place of porphyrin
Maintenance of an adequate calorie intake can be
analysis. Fluorescence emission spectroscopy of plasma
achieved more safely by nasogastric feeding. Intravenous
simplifies the differentiation of variegate porphyria from
haematin has largely replaced carbohydrate as the
specific therapy of choice for the acute attack; it
In patients who have latent porphyria or are in
suppresses hepatic ALA-S by negative feedback and
remission, differentiation of an attack of acute porphyria
is highly effective in reducing aminolaevulinate and
from other causes of abdominal pain may be difficult,
porphobilinogen excretion.21 The only placebo-controlled
Hypertension (diastolic blood pressure >85 mm Hg)
Figures are percentages of number of acute attacks. *See further reading section. †Unpublished data.
Table 2: Symptoms and signs of acute porphyria
study of this therapy suggested that the clinical benefit of
intravenous haematin was modest.24 Uncontrolled data
With improvements in management, severe neuropathy
suggest that haem arginate (Normosang, Leiras Medica,
and death are now less common than in the past.15
Finland) is highly efficacious, but it will not reverse an
Recurrent attacks are more common in acute intermittent
established neuropathy and must be given during the
porphyria than in variegate porphyria. Patients may
develop hypertension or chronic renal failure.28 Acute
Administration of haematin may induce haem
porphyrias may also be associated with an increased risk
oxygenase, with consequent enhanced catabolism.21 We
observed apparent clinical tolerance to haem arginate in afew patients who required repeated courses at short
intervals; efficacy was restored by the coadministration of
Success in caring for patients with the acute porphyrias
tin protoporphyrin, an inhibitor of haem oxygenase.26
lies less in crisis intervention at the time of the acute
However, tin protoporphyrin causes photosensitivity and
attack than it does in enabling affected patients and their
its long-term toxicity is unknown. Zinc mesoporphyrin
families to keep to a minimum the risk of an attack.
may be a safer alternative but requires evaluation.21
Family studies are essential to identify individuals withclinically latent porphyria so that they can be counselled
about the need to avoid drugs and other factors thatprovoke acute attacks.1,16,21
Frequent recurrences of the acute attack are usually
porphyria in children and most adults requires specialised
encountered in patients with acute intermittent porphyria
enzymatic and other methods,19 such as DNA analysis,2–4,30
who have attacks induced by menstruation or who
and is best undertaken in a referral centre. Most of those
repeatedly take inducing agents. With menstrually related
who inherit an acute porphyria will lead a normal life and
attacks, attempts to regulate the menstrual cycle with sex
many will be symptom-free; the lives of only a minority
steroids may exacerbate the porphyria. Some patients
are blighted by the disease. No specific diet is indicated
have responded well to hormonal suppression with
for porphyria, though sudden or prolonged calorie
gonadotrophin-releasing hormone agonists.1,27
restriction may induce an acute attack and should be
functional menopause is induced by these agonists which
avoided, as should alcoholic beverages. Although early
may be accompanied by symptoms of oestrogen
reports suggest a high incidence of acute attacks in
deficiency and accelerated osteoporosis. These effects
pregnancy and the puerperium, pregnancy seems to pose
may be reduced by cyclical adminstration or hormone
little increased risk to patients who are known in advance
replacement, but the safety and efficacy of different
to have porphyria and need not be discouraged.18
regimens need further investigation. In one patient, we
Similarly, general anaesthesia and surgical operations
found that supplemental oestrogen arrested the
carry little increased risk of an acute attack provided prior
oestoporosis and was tolerated, whereas progesterone
knowledge of the diagnosis enables agents that provoke
intermittent acute porphyria in a psychiatric patient population. Am J Psychiatry 1985; 142: 1430–36.
Kappas A, Sassa S, Galbraith RA, Nordmann Y. The porphyrias. In:Scriver CL, Beaudet AL, Sly WS, Valle D, eds. The metabolic basis of
14 Whatley SD, Roberts AG, Elder GH. De-novo mutation and sporadic
inherited disease. New York: McGraw-Hill, 1989: 1305–65.
presentation of acute intermittent porphyria. Lancet 1995; 346:
Elder GH. Molecular genetics of disorders of haem biosynthesis.
J Clin Pathol 1993; 46: 977–81.
15 Kauppinen R, Mustajoki P. Prognosis of acute porphyria: occurrence
Deybach J-C, Puy H. Porphobilinogen gene structure and molecular
of acute attacks, precipitating factors, and associated diseases. Medicine
defects. J Bioenerg Biomembr 1995; 27: 197–205.
1992; 71: 1–13.
Puy H, Deybach J-C, Lamoril J, et al. Molecular epidemiology and
16 Disler PB, Moore MR. Drug therapy in acute porphyrias. Clin
diagnosis of PBG deaminase gene defects in acute intermittent
Dermatol 1985; 3: 112–24.
porphyria. Am J Hum Genet (in press).
17 Patience DA, Blackwood DHR, McColl KEL, Moore MR. Acute
Chen C-H, Astrin KH, Lee G, Anderson KE, Desnick RJ. Acute
intermittent porphyria and mental illness—a family study. Acta Psych
intermittent porphyria: identification and expression of exonic
Scand 1994; 89: 262–67.
mutations in the hydroxymethylbilane synthase gene. J Clin Invest
18 Buttery JE. Is the Watson-Schwartz screening method for
1994; 94: 1927–37.
porphobilinogen reliable? Clin Chem 1995; 41: 1670–71.
Brownlie PD, Lambert R, Louie GV, et al. The three-dimensional
19 Elder GH, Smith SG, Smyth SJ. Laboratory investigation of the
structure of mutants or porphobilinogen deaminase: toward an
porphyrias. Ann Clin Biochem 1990; 27: 395–412.
understanding of the structural basis of acute intermittent porphyria.
20 Poh-Fitzpatrick MB. A plasma porphyrin fluorescence marker for
Protein Sci 1994; 3: 1644–50.
variegate porphyria. Arch Dermatol 1980; 116: 543–47.
Dean G. The porphyrias: a story of inheritance and environment.
21 Bonkovsky HL. Advances in understanding and treating ‘The little
imitator’, acute porphyria. Gastroenterology 1993; 105: 590–94.
Meissner PN, Dailey TA, Hift RJ, et al. A R59W mutation in human
22 Lindberg RLP, Porcher C, Grandchamp B, et al. Porphobilinogen
protoporphyrinogen oxidase results in decreased enzyme activity and is
deaminase deficiency in mice causes a neuropathy resembling that of
prevalent in South Africans with variegate porphyria. Nat Genet 1996;
human hepatic porphyria. Nat Genet 1996; 12: 195–99. 13: 95–97.
23 Brodie MJ, Moore MR, Thompson GG, Goldberg A. The treatment
McColl KEL, Moore MR, Thompson GG, et al. Chester porphyria—
of acute intermittent porphyria with laevulose. Clin Sci Mol Med 1977;
biochemical studies of a new form of acute porphyria. Lancet 1985; ii:
53: 365–71.
24 Herrick AL, McColl KEL, Moore MR, Cook A, Goldberg A.
10 Moore MR, McColl KEL, Rimington C, Goldberg A. Disorders of
Controlled trial of haem arginate in acute hepatic porphyria. Lancet
porphyrin metabolism. New York: Plenum Press, 1987.
11 Mustajoki P, Koskelo P. Hereditary hepatic porphyrias in Finland.
25 Mustajoki P, Nordmann Y. Early administration of heme arginate for
Acta Med Scand 1976; 200: 171–78.
acute porphyric attacks. Arch Intern Med 1993; 153: 2004–08.
12 Mustajoki P, Kauppinen R, Lannfelt L, Lilius L, Koistinen J.
26 Dover SB, Moore MR, Fitzsimmons EJ, Graham A, McColl KEL. Tin
Frequency of low erythrocyte porphobilinogen deaminase activity in
protoporphyrin prolongs the biochemical remission produced by heme
Finland. J Int Med 1992; 231: 389–95.
arginate in acute hepatic porphyria. Gastroenterology 1993; 105:
13 Tishler PV, Woodward B, O’Connor J, et al. High prevalence of
27 Anderson KE, Spitz IM, Bardin CW, Kappas A. A gonadotopin
29 Bengtsson NO, Hardell L, Porphyrias, porphyrins and hepatocellular
releasing hormone analogue prevents cyclical attacks of porphyria. Arch
cancer. Br J Cancer 1986; 54: 115–17. Intern Med 1990; 150: 1469–74.
30 Kauppinen R, Mustajoki S, Pihlaja H, Peltonen L, Mustajoki P. Acute
28 Church SE, McColl KEL, Moore MR, Youngs GR. Hypertension and
intermittent porphyria in Finland: 19 mutations in the
renal impairment as complications of acute porphyria. Nephrol Dial
porphobilinogen deaminase gene. Hum Mol Genet 1995; 4: 215–22. Transplant 1992; 7: 986–90.
Stein JA, Tschudy DP. Acute intermittent porphyria: a clinical and
biochemical study of 46 patients. Medicine 1970; 49: 1–16.
Waldenstrom J. The porphyrias in inborn errors of metabolism. Am J Med
Anderson KE. The porphyrias. In: Z akin D, Boyer TD, eds.
Hepatology: a tex tbook of liver disease. Philadelphia: W B Saunders,
X u W, Solis C, Bermejo AM, Astrin KH, Desnick RJ. Clinical and
molecular delineation of severe homozygous dominant acute
Arnold WN. Vincent Van Gogh: chemicals, crises and creativity.
intermittent porphyria. Pediatric Res 1995; 37: A155.
Macalpine I, Hunter R. George III and the mad business. New York:
Bont A, Steck AJ, Meyer UA. The acute hepatic porphyrias and their
Warren MJ, Jay M, Hunt DM, Elder GH, Röhl JC. The maddening
neurologic syndromes. Schweiz Med Wochenschr 1996; 126: 6–14.
business of King George III and porphyria. Trends Biochem Sci 1996;
Litman DA, Correia MA. L-tryptophan: a common demoninator of
biochemical and neurological events of acute hepatic porphyria. Science 1983; 222: 1031–33.
Puy H, Deybach J-C, Bogdan A, et al. Increased delta-aminolevlinic acid
Grandchamp B, Lanoril J, Puy H. Molecular abnormalities of
and decreased pineal melatonin production—a common event in
coproporphyrinogen ox idase in patients with hereditary
acute porphyria: studies in the rat. J Clin Invest 1996; 97: 104–10.
coproporphyria. J Bioenerg Biomembr 1995; 27: 215–20.
Jenkins T. The South African malady. Nat Genet 1996; 13: 7–9.
Wood S, Lambert R, Jordan PM. Molecular basis of acute intermittent
Dover SB, Plenderleith L, Moore MR, McColl KEL. Safety of general
porphyria. Mol Med Today 1995; 1: 232–39.
anaesthesia and surgery in acute hepatic porphyria. Gut 1994; 35:1112–15.
Harrison GG, Meissner PN, Hift RJ. Anaesthesia for the porphyric
Eales L, Day RS, Blekkenhorst GH. The clinical and biochemical features
patient. Anaesthesia 1993; 48: 417–21.
of variegate porphyria—an analysis of 300 cases studied at Groote
Lip GY, McColl KE, Goldberg A, Moore MR. Smoking and recurrent
Schuur Hospital, Cape Town. Int J Biochem 1980; 12: 837–53.
attacks of acute intermittent porphyria. BMJ 1991; 302: 507–08.
Goldberg A. Acute intermittent porphyria: a study of 50 cases. QJM
Meissner PN, Hift RJ, Schmid R, Porphyria. In: Kirsch RE, Robson CR,
Trey C, eds. Diagnosis and management of liver disease. London:
Hift RJ, Meissner PN, Todd G, et al. Homozygous variegate porphyria: an
evolving clinical syndrome. Postgrad Med J 1993; 69: 781–86.
Robert TL, Varella L, Meguid MM. Nutrition managment of acute
Llewellyn DH, Smyth SJ, Elder GH, et al. Homozygous acute intermittent
intermittent porphyria. Nutrition 1994; 10: 551–55.
porphyria caused by adjacent base transitions in the same codon of
Sassa S. Diagnosis and therapy of acute intermittent porphyria. Blood
the porphobilinogen deaminase gene. Hum Genet 1992; 89: 97–98.
III -7 Buenas maneras para la convivencia: 1. Convivir con los japoneses: Para vivir en Japón lo primero que hay que tener en cuenta son las normas de cortesía y las costumbres diarias, de esta manera podrá irse acostumbrando a ellas y aplicarlas. Es importante no llegar tarde a las citas. En caso de llegar tarde o no poder acudir, hay que avisárselo sin falta. La forma de saludar
 especially in those few patients who become addictedto opiates. In variegate porphyria and hereditarycoporporhyria, porphobilinogen excretion will generallybe normal in the absence of symptoms. In acuteintermittent porphyria, concentratons are often raisedduring the symptomless phase and increase further duringan acute attack.
especially in those few patients who become addictedto opiates. In variegate porphyria and hereditarycoporporhyria, porphobilinogen excretion will generallybe normal in the absence of symptoms. In acuteintermittent porphyria, concentratons are often raisedduring the symptomless phase and increase further duringan acute attack.