Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
Sdb - mb 8 e - crofab - englisch.doc
Serum-Depot Berlin e. V. Merkblatt 8 - E CROFAB TM CROTALIDAE POLYVALENT IMMUNE FAB (OVINE)
DESCRIPTION CroFabTM [Crotalidae Polyvalent Immune Fab (Ovine)] is a sterile, nonpyrogenic, purified, lyophilized preparation of ovine Fab (monovalent) immunoglobulin fragments obtained from the blood of healthy sheep flocks immunized with one of the following North American snake venoms: Crotalus atrox (Western Diamondback rattlesnake), Crotalus adamanteus (Eastern Diamondback rattlesnake), Crotalus scutulatus (Mojave rattlesnake), and Agkistrodon piscivorus (Cottonmouth or Water Moccasin). To obtain the final antivenin product, the tour different monospecific antivenins are mixed. Each monospecific antivenin is prepared by fractionating the immunoglobulin from the ovine serum, digesting it with papain, and isolating the venom-specific fab fragments on ion exchange and affinity chromatography columns. CroFab is standardized by its abiliry to neutralize the lethal action of each of the fcur venom immunogens following intravenous injection in mice. The potency of the product will vary from batch to batch; however, a minimum number of mouse LD50 neutralizing units against each of the four venoms is included in every vial of final product, as shown in Table t. For comparison, the minimum potency of each monospecitic component in the batches demonstrated to be efficacious in clinical trials is also included in Table 1. Table 1. Minimum Mouse LD50 Neutralizin Units* for Each Venom Component Minimum Potency per Vial of CroFab Minimum Potency per Vial of Clinical Trial Batches [95 % Reference Intervall]
*One neutralizing unit is determined as the amount of the mixed monospecific Fab
proteins necessary to neutralize one LD50 of each of the four venoms, where the LD50 is the amount of venom that would be lethal in 50 % of mice. Each vial of CroFab contains up to 1g of total protein and sodium phosphate buffer consisting of dibasic sodium phosphate USP and sodium chloride USP. Thimerosal is used as a preservative in the manufacturing process, and as such, mercury is carried over into the final product at an amount no greater than 104.5 mcg per vial, which amounts to no more than 1.9 mg of mercury per dose (based on the maximum dose of 18 vials used in clinical studies of SDB; Merkblatt 8 - E
CroFab). The product is intended for intravenous administration after reconstitution with 10 ml of Sterile Water for Injection USP. CLINICAL PHARMACOLOGY Mechanism ot Action: CroFab is a venom-specific Fab fragment of immunoglobulin G (IgG) that works by binding and neutralizing venom toxins, facilitating their redistribution away from target tissues and their elimination from the body. Animal Studies: CroFab was effective in neutralizing the venoms of 10 clinically important North American crotalid snakes in a murine lethality model (see Table 2) [1]. In addition, preliminary data from experiments in mice using whole IgG from the sheep immunized for CroFab production suggest that CroFab might possess antigenic cross-reactivity against the venoms of some Middle Eastern and North African snakes; however, there are no clinical data available to confirm these findings. Table 2. ED50 Values for CroFab in Mice Stody Objective & Endpoint Major Findings and Conclusions Measured
the ED50 for each (Note: Lower numbers represent increased potency againsl
S. m. barbouri 7 C. h. horridus 6 Based on the data from this study in mice, CroFab has relatively good cross-protection against venoms not used in the immunization of flocks used to produce it, except for C. v helleri, where a very high dose is required, and for C. m. molossus, where a moderately high dose is required.
Clinical Pharmacokinetics: The planned pharmacokinetic study of CroFab was not adequately performed. A limited number of samples were collected from three patients. Based on these data, estimates of elimination half-life were made. The elimination half-life for total Fab ranged from approximately 12 to 23 hours. These limited pharmacokinetic estimates of half-life are augmented by data obtained with an analogous ovine Fab product produced by Protherics Inc. using a similar production process. In that study, 8 healthy subjects were SDB; Merkblatt 8 - E
given 1 mg of intravenous digoxin followed by an approximately equimolar neutralizing dose of 76 mg of digoxin immune Fab (ovine). Total Fab was shown to have a volume of distribution of 0.3 L/kg, a systemic clearance of 32 mL/min (approximately 0.4 mL/min/kg) and an elimination half-life of approximately 15 hours. Clinical Studies: No clinical studies have been conducted comparing CroFab with other antivenins, therefore, no comparisons can be made belween CroFab and other antivenins.
Two clinical trials using CroFab have been conducted. They were prospectivefy defined, open-label, muhl-center trials conducted in otherwise healthy patients 11 years of age or older who had suffered from minimal or moderate (as defined in Table 3) North American crotalid envenomation that showed evidence of progression. Progression was defined as the worsening of any evaluation parameter used in the grading of an envenomation: local injury, laboratory abnormality or symptoms and signs attributable to crotalid snake venom poisoning. Both clinical trials excluded patients with Copperhead envenomation. To date, there are no clinical data supporting the efficacy of CroFab in patients presenting with severe envenomation. Table 3. Definitian of Minimal, Moderate, and Severe Envenomation in Clinical Studies of CroFab Envenomalian Definition Category
Swelling, pain and ecchymosis limited to the immediate bite site;
Coagulation parameters normal with no clinical evidence of bleeding.
Swelling, pain, and ecchymosis involving less than a full extremity or, if
bite was sustained on the trunk, head or neck, extending less than 50 cm; Systemic signs and symptoms may be present but not life threatening, including but not limited to nausea, vomiting, oral paresthesia or unusual tastes, mild hypotension (systolic blood pressure <90 mmHg), mild tachycardia (heart rate <150), and tachypnea; Coagulation parameters may be abnormal, but no clinical evidence of bleeding present. Minor hematuria, gum bleeding and nosebleeds are ailowed if they are not considered severe in the investigatof`s judgment.
Swelling pain, and ecchymosis involving more than an entire extremity or
threatening the airway; Svstemic signs and symptoms are markedly abnormal, including severe alteration of mental status, severe hypotension, severe tachycardia, tachypnea, or respiratory insufficiency; Coagulation parameters are abnormal, with serious bleeding or severe threat of bleeding.
In both clinical studies, efficacy was determined using a Snakebite Severity Score (SSS) [2] (referred to as the efficacy score or ES in these clinical studies) and an investigator's clinical assessment (ICA) of efficacy. The SSS (referred to as the ES) is a tool used to measure the severity of envenomation based on six body categories; local wound (e.g.,.pain, swelling and ecchymosis), pulmonary, cardiovascular, gastrointestinal, hematological, and nervous system
SDB; Merkblatt 8 - E
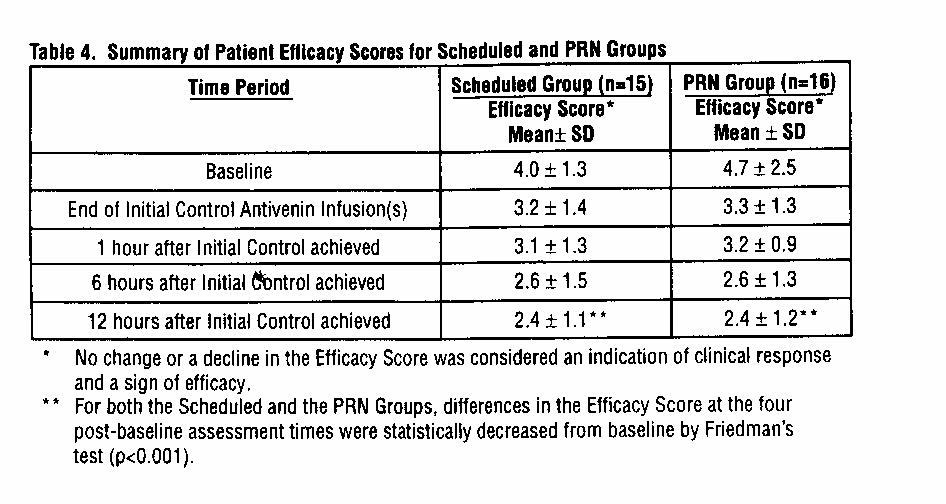
effects. A higher score indicates worse symptoms. In a retrospective study using medical records of 108 snakebite victims [2], the SSS has been shown to correlate well with physi- cians' assessment of the patient's condition at presentation (Pearson correlation coefficient: r=0.63, p<0.0001) and when the patient's condition was at its worst (r=0.70, p<0.0001). In this study, the condition of 87/108 patients worsened during hospitalization. Changes in the physicians' assessment of condition correlated well with changes in SSS. CroFab was required to prevent an increase in the ES in order to demonstrate efficacy. The ICA was based on the investigator's clinical judgment as to whether the patient had a: · Clinical response (pre-treatment signs and symptoms of envenomation were arrested or improved after treatment) · Partial response (signs and symptoms of envenomation worsened, but at a slower rate than expected after treatment) · Non-response (the patient's condition was not favorably affected by the treatment). Safety was assessed by monitoring for early allergic events, such as anaphylaxis and early serum reactions during CroFab infusion, and late events, such as late serum reactions. TAb001: In the first clinical study of CroFab, 11 patients received an intravenous dose of 4 vials of CroFab over 60 minutes. An additional 4-vial dose of CroFab was administered affer completion of the first CroFab infusion, if deemed necessary by the investigator. At the 1- hour assessment, 10 out of 11 patients had no change or a decrease in their ES. Ten of 11 patients were also judged to have a clinical response by the ICA. Several patients, after initial clinical response, subsequently required additional vials of CroFab to stem progressive or recurrent symptoms and signs. No patient in this first study experienced an anaphylactic or anaphylactoid response or evidence of an early or late serum reaction as a result of administration of CroFab. TAb002: Based on observations from the first study, the second clinical study of CroFab compared two different dosage schedules. Patients were given an initial intravenous dose of 6 vials ot CroFab with an option to retreat with an additional 6 vials, if needed, to achieve initial control of the envenomation syndrome. Initial control was defined as complete arrest of local manifestations, and return of coagulation tests and systemic signs to normal. Once initial control was achieved, patients were randomized to receive additional CroFab either every 6 hours for 18 hours (Scheduled Group) or as needed (PRN Group). In this trial, CroFab was administered safely to 31 patients with minimal or moderate crotalid envenomation. All 31 patients enrolled in the study achieved initial control of their envenomation with CroFab, and 30, 25 and 26 of the 31 patients achieved a clinical response based on the ICA at 1, 6 and 12 hours respectively following initial control. Additionally, the mean ES was significantly decreased across the patient groups by the 12-hour evaluation time point (p=0.05 for the Scheduled Group; p=0.05 for the PRN Group) (see Table 4). There was no statistically significant difference between the Scheduled Group and the PRN Group with regard to the decrease in ES. SDB; Merkblatt 8 - E
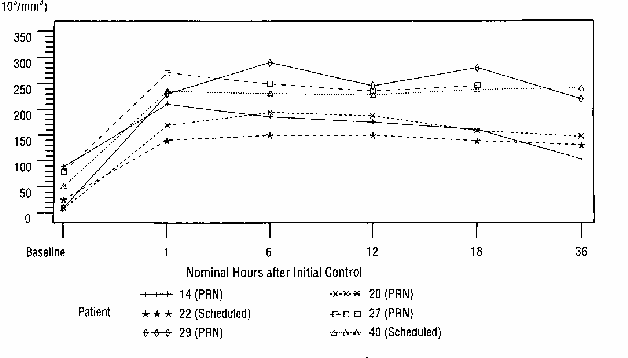
In published literature accounts of rattlesnake bites, it has been noted that a decrease in platelets can accompany moderately severe envenomation, which whole blood transfusions could not correct [3]. These platelet count decreases have been observed to last tor many hours and often several days following the venomous bite [3, 4, 5]. In this clinical study, 6 patients had pre-dosing platelet counts below 100,000/mm³ (baseline average of 44,000/mm³). Of note, the platelet counts for all 6 patients increased to normal levels (average 209,000/mm³) at 1 hour following initial control dosing with CroFab (see Figure 1). Figure 1. Graph of Platelel Counts from Baseline to 36 Hours for Patients with Counts <100,00/mm³ at Baseline (Study TAb002) Plateles
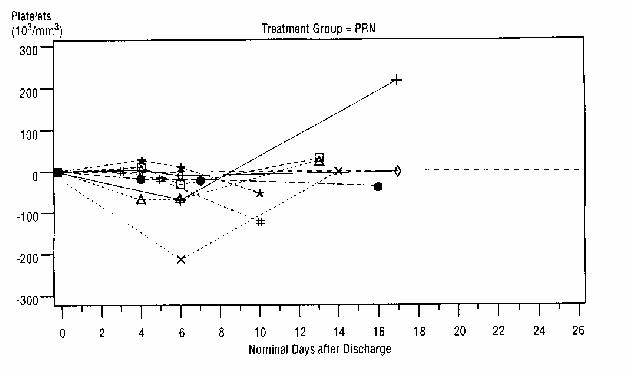
Although there was no significant difference in the decrease in ES-between the two treatment groups, the data suggest that Scheduled dosing may provide better control of envenomation symptoms caused by the continued leaking of venom from depot sites. Scheduled patients experienced a lower incidence of coagulation abnormalities at follow-up compared with PRN patients (see Table 5 and Figure 2). In addition, the need to administer.additional CroFab to patients in the PRN Group after initial control suggests that there is a continued need for antivenin for adequate treatment.
SDB; Merkblatt 8 - E Table 5. Lower Incidence ol Hecurrence of Coagulopalhies ar Follow-Up in Scheduled and PRN Dosing
Groups Schedoled Group (n=14)* PRN Group (n=16) (percent of palienls with abnormal values)^ (percent ol patients with abnormal values)^ Platelet Fibrinogen
^ Numbers are expressed as percent ot patients that had a follow-up platelet count that was less than the count at hospital discharge, or a fibrinogen level less than 50% of the level at hospital discharge. * Follow-up data not available for one patient. ** Statistically significant difterence, p=0.04 by Fisher's Exact test. Figure 2. Change in Platelet Counts in Individual Palients between Follow-Up Visits and Dissharge Patients in the Scheduled and PRN Groups are plotted separately. More patients in the PRN Group showed a reduction in platelet count after discharge than in the Scheduled Group. Only patients showing a reduced platelet count after discharge are shown.
INDICATIONS AND USAGE CroFab is indicated for the management of patients with minimal or moderate North American crotalid envenomation (see Table 3 in Clinical Studies section for definitions). Early use of CroFab (within 6 hours of snakebite) is advised to prevent clinical deterioration and the occurrence of systemic coagulation abnormalities. SDB; Merkblatt 8 - E CONTRAINDICATIONS CroFab should not be administered to patients with a known history of hypersensitivity to papaya or papain unless the benefits outweigh the risks and appropriate management for anaphylactic reactions is readily available. WARNINGS · Coagulopathy is a complication noted in many victims of viper envenomation that arises due to the ability of the snake venom to interfere with the blood coagulation cascade [4, 8, 9]. In clinical trials with CroFab, recurrent coagulopathy (the return of a coagulation abnormality after it has been successfully treated with antivenin), characterized by decreased fibrinogen, decreased platelets, and elevated prothrombin time, occurred in approximately half of patients studied. The clinical significance of these recurrent abnormalities is not known. Recurrent coagulation abnormalities were observed only in patients who experienced coagulation abnormalities during their initial hospitalization. Optimal dosing to completely prevent recurrent coagulopathy has not been determined. Because CroFab has a shorter persistence in the blood than crotalid venoms that can leak from depot sites over a prolonged period of time, repeat dosing to prevent or treat such recurrence may be necessary (see DOSAGE AND ADMINISTRATION). · Recurrent coagulopathy may persist for 1 to 2 weeks or more. Patients who experience coagulopathy due to snakebite during hospitalization for initial treatment should be monitored for signs and symptoms of recurrent coagulopathy for up to 1 week or longer at the physician's discretion. During this period, the physician should carefully assess the need for re-treatment with CroFab and use of any type of anticoagulant or anti-platelet drug. · Papain is used to cleave the whole antibody into Fab and Fc fragments, and trace amounts of papain or inactivated papain residues may be present in CroFab. Patients with allergies to papain, chymopapain, other papaya extracts, or the pineapple enzyme bromelain may also be at risk for an allergic reaction to CroFab. In addition, it has been noted in the literature that some dust mite allergens and some latex allergens share antigenic structures with papain and patients with these allergies may be allergic to papain [6,7] (see CONTRAINDICATIONS). CROFABTM CROTALIDAE POLYVALENT IMMUNE FAB (OVINE) PRECAUTIONS General: CroFab contains mercury in the form of ethyl mercury from thimerosal. The final product contains up to 104.5 mcg or approximately 0.11 mg of mercury per vial, which amounts to no more than 1.9 mg of mercury per dose (based on the maximum dose of 18 vials studied in clinical trials of CroFab). While there are no definitive data on the toxicity of ethyl mercury, literature suggests that information related to methyl mercury toxicities may be applicable. Anaphylaxis, Anaphylactoid Reactions and Allergic Reactions: · The possible risks and side-effects that attend the administration of heterologous animal proteins in humans include anaphylactic and anaphylactoid reactions, delayed allergic reactions (late serum reaction or serum sickness) and a possible febrile response to immune complexes formed by animal antibodies and neutralized venom components [10]. Although no patient in the clinical studies of CroFab has experienced a severe anaphylactic reaction, the possibility of an anaphylactic reaction should be considered. The patient should be informed of the possibility of an anaphylactic reaction and close patient monitoring and readiness with intravenous therapy using epinephrine and diphenhydramine hydrochloride is recommended during the infusion of CroFab. If an anaphylactic reaction occurs during SDB; Merkblatt 8 - E
the infusion, CroFab administration should be terminated at once and appropriate treatment administered. Patients with known allergies to sheep protein would be particularly at risk for an anaphylactic reaction. · All patients treated with antivenin should be carefully monitored for signs and symptoms of an acute allergic reaction (e.g., urticaria, pruritus, erythema, angioedema, bronchospasm with wheezing or cough, stridor, laryngeal edema, hypotension, tachycardia) and treated with appropriate emergency medical care (e.g., epinephrine, intravenous antihistamines and/or albuterol). · All patients should be followed-up for signs and symptoms of delayed allergic reactions or serum sickness (e.g., rash, fever, myalgia, arthralgia) and treated appropriately if necessary. · It has been noted in the literature with the use of other antibody therapies, that reactions during the infusion, such as fever, low back pain, wheezing and nausea are offen related to the rate of infusion and can be controlled by decreasing the rate of administration of the solution [11]. · Patients who receive a course ot treatment with a foreign protein such as CroFab may become sensitized to it. Therefore, caution should be used when administering a repeat course of treatment with CroFab for a subsequent envenomation episode. · Skin testing has not been used in clinical trials of CroFab and is not required. Because snake envenomation can cause coagulation abnormalities, the following conditions, which are also associated with coagulation defects, should be considered: cancer, collagen disease, congestive heart failure, diarrhea, elevated temperature, hepatic disorders, hyperthyroidism, poor nutritional state, steatorrhea, vitamin K deficiency. Information for Patients: · Patients should be advised to contact their physician immediately if they experience any signs and symptoms of delayed allergic reactions or serum sickness (e.g., rash, pruritus, urticaria) affer hospital discharge. · Patients should be advised to contact their physician immediately if they experience unusual bruising or bleeding (e.g., nosebleeds, excessive bleeding affer brushing teeth, the appearance of blood in stools or urine, excessive menstrual 6leeding, petechiae, excessive bruising or persistent oozing from suporficial injuries) affer hospital discharge as they may need additional antivenin treatment. Such bruising or bleeding may occur for up to 1 week or longer following initial treatment, and patients should be advised to follow-up with their physician for monitoring. Drug Interactions: Studies of drug interactions have not been conducted with CroFab. Carcinogenesis, Mutagenesis, Impairment of Fertility: Animal carcinogenicity and reproduction studies have not been conducted with CroFab. Pregnancy: Pregnancy Category C. Animal reproduction studies have not been conducted with CroFab. It is also not known whether CroFab can cause fetal harm when administered to a pregnant woman or can affect reproduction capacity. CroFab should be given to a pregnant woman only if clearly needed. CroFab contains mercury in the form of ethyl memury from thimerosal (see PRECAUTIONS, General). Although there are limited toxicology data on ethyl mercury, high dose and acute exposures to methyl mercury have been associated with SDB; Merkblatt 8 - E neurological and renal toxicities. Developing fetuses and very young children are most susceptible and therefore, at greater risk.
Nursing Mothers: It is not known whether CroFab is excreted in human breast milk. Because many drugs are excreted in human milk, caution should be exercised when CroFab is administered to a nursing woman. Geriatic Use: Specific studies in elderly patients have not been conducted. Pediatric Use: Specific studies in pediatric patients have not been conducted. The absolute venom dose following snakebite is expected to be the same in children and adults, therefore, no dosage adjustment for age should be made. CroFab contains mercury in the form of ethyl mercury from thimerosal (see PRECAUTIONS, General). Although there are limited toxicology data on ethyl mercury, high dose and acute exposures to methyl mercury have been associated with neurological and renal toxicities. Developing fetuses and very young children are most susceptible and therefore, at greater risk.
ADVERSE REACTIONS · The majority of adverse reactions to CroFab reported in clinical studies were mild or moderate in severify. · The most common adverse events reported in the clinical studies were urticaria and rash. Adverse events involving the skin and appendages (primarily rash, urticaria, and pruritus) were reported in 14 of the 42 patients (Table 6). · Of the 25 patients who experienced adverse reactions, 3 patients experienced severe or serious adverse reactions. The 1 patient who experienced a serious adverse event had a recurrent coagulopathy due to envenomation, which required re-hospitalization and additional antivenin administration. This patient eventually made a complete recovery. The other 2 had severe adverse reactions that consisted of 1 patient who developed severe hives following treatment and t patient who developed a severe rash and pruritus several days following treatment. Both patients recovered following treatment with antihistamines and prednisone. · One patient discontinued CroFab therapy due to an allergic reaction. SDB; Merkblatt 8 - E Seite - 10
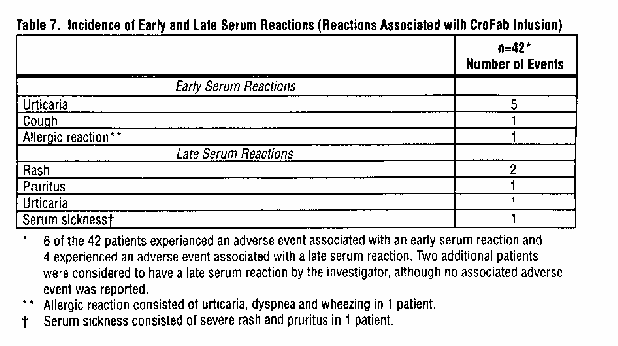
In the 42 patients treated with CroFab for minimal or moderate crotalid envenomations, there were 7 events classified as early serum reactions and 5 events classified as late serum reactions, and none were serious (Table 7). In the clinical studies, serum reactions consisted mainly of urticaria and rash, and all patients recovered without sequelae.
SDB; Merkblatt 8 - E Seite - 11 OVERDOSAGE The maximum amount of CroFab that can safely be administered in single or multiple doses has not been determined. Doses of up to 18 vials (approximately 13.5 g of protein) have been administered without any observed direct toxic effect. DOSAGE AND ADMINISTRATION Each vial of CroFab should be reconstituted with 10 mL of Sterile Water for Injection USP (diluent not included) and mixed by continuous gentle swirling. The contents of the reconstituted vials should be further diluted in 250 mL of 0.9 % Sodium Chloride USP and mixed by gently swirling. The reconstituted and diluted product should be used within 4 hours. Administration of antivenin should be initiated as soon as possible affer crotalid snakebite in patients who develop signs of progressive envenomation (e.g., worsening local injury, coagulation abnormality, or systemic signs of envenomation). CroFab was shown in the clinical studies to be effective when given within 6 hours of snakebite. Ativenin dosage requirements are contingent upon an individual patient's response; however, based on clinical experience with CroFab, the recommended initial dose is 4 to 6 vials. The patient should be observed for up to 1 hour fcllowing the completion of this first dose to determine if initial control ot the envenomation has been achieved (as defined by complete arrest of local manifestations, and return of coagulation tests and systemic signs to normal). If initial control is not achieved by the first dose, an additional dose of 4 to 6 vials should be repeated until initial control of the anvenomation syndrome has been achieved. After initial control has been established, additional 2-vial doses of CroFab every 6 hours for up to 18 hours (3 doses) is recommended. Optimal dosing following the 18-hour scheduled dose of CroFab has not been determined. Additional 2-vial doses may be administered as deemed necessary by the treating physician, based on the patient's clinical course. The initial dose of CroFab diluted in 250 mL of saline should be infused intravencusly over 60 minutes. However, the infusion should proceed slowly over the first 10 minutes at a 25-50 mL/hour rate with careful observation for any allergic reaction. If no such reaction occurs, the infusion rate may be increased to the full 250 mL/hour rate until completion. Close patient monitoring is necessary. Additional Patient Care (Supporlive and Adjunctive Therapy): Supportive measures are often utilized to treat certain man'rfestations of crotalid snake envenomation, such as pain, swelling, hypotension, and wound infection. Poison control centers are a helpful resource for individual treatment advice. HOW SUPPLIED CroFab is supplied as a sterile, nonpyrogenic, purified, lyophilized preparation. Each vial contains up to 1 g of total protein, a maximum of 0.11 mg of mercury, and not less than the indicated number of mouse LD50 neutralizing units:
C. atrox (Western Diamondback rattlesnake)
C. adamanteus (Eastern Diamondback rattlesnake)
A. piscivorus (Cottonmouth or Water Moccasin)
Each box contains 2 vials of CroFab (diluent not included).
SDB; Merkblatt 8 - E Seite - 12 Storage Conditions: The product should be stored at 2° to 8°C (36° to 46°F). Do not freeze. The product must be used within 4 hours after reconstitution. REFERENCES
1. Consroe, P., Egen N.B., Russell, F.E., Gerrish, K., Smith, D.C., Sidki, A., et al. Comparison
of a new ovine antigen binding fragment (Fab) antivenin for United States Crotalidae with the commercial antivenin for protection against venom-induced lethality in mice. J Trop Med Hyg 1995; 53(5):507-510. 2. Dart, R.C., Hurlbut, K.M., Garcia, R., Boren, J., Validation of a severity score for the assessment of Crotalid snakebite. Ann Emerg Med 1996; 2713):321-326. 3. La Grange, R.G., and Russell, F.E., Blood platelet studies in man and rabbits following Crotalus envenomation, Proc West Pharmacol Soc 1970;13:99-105. 4. Lyons, W.J.m Profound thrombocytopenia associated with Crotalus ruber ruber envenomation: a clinical case. Toxicon 1971; 9:237-240. 5. Tallon, R.W., Koch, K.L., Barnes, S.G., Ballard, J.0., Letter to Editor. N Engl J Med 1981;305:1347. 6. Quarre, J.P., Lecomte, J., Lauwers, D., Gilbert, P., Thiriaux, J., Allergy to latex and papain. J Allergy Clin Immunol 1995; 95(4):922. 7. Baur, X., Chen, Z., Rozynek, P., Duser, D., Raulf-Heimsoth, M. Cross-reacting IgE antibodies recognizing latex allergens, including Hev b 1, as well as papain. Allergy 1995; 50(7):604-609. 8. Furlow, T.G., Brennan, L.V., Purpura following timber rattlesnake (Crotalus horridus horridus) envenomation. Cutis 1985; 35:234-236. 9. Budzynski, A.Z., Pandya, B.V., Rubin, R.N., Brizuela, B.S., Soszka, T., Stewart, G.J., Fibrinogenolytic afibrinogenemia after envenomation by western diamondback rattlesnake (Crotalus atrox) Blood 1984; 63(1 ):1-14. 10. Kojis, F.G., Serum sickness and anaphylaxis. Am J Dis Child 1997;93-350. 11. Kirkpatrick, C.H., The Digibind Study Advisory Panel. Allergic histories and reactions of patients treated with digoxin immune Fab (ovine) antibody.Am J Emerg Med 1991; 9(2 Suppl 1):7-10. Rx only Manufactured by: Protherics Inc. Nashville, TN 37212 U.S. License No. 1575 Revised December 2000
Reform / Living to be 500, death by asteroid, and the inevitability of NHS reformReform / Living to be 500, death by asteroid, and the inevitability of NHS reformwhile typically the private sector succeeds by showing how well it is doing, the public sector often declaims its own failure in the hope of extracting more government spending. And, partly, it’s because publicly-funded healthcare
SOLVENCY GUARANTEE FACILITY CHECKLIST: GUARANTEE APPLICATIONS FOR NEW CLIENTS Note: The attached Proposal Form is intended for companies that wish to apply for a guarantee facility with SGI Guarantee Acceptances a division of Constantia Insurance Company Ltd (SGIGA). Existing clients of SGIGA should use the 1 page application form. The Proposal Form attached is to
 SDB; Merkblatt 8 - E
SDB; Merkblatt 8 - E 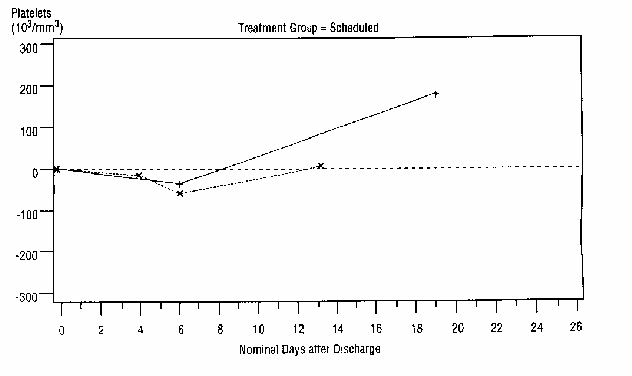
 SDB; Merkblatt 8 - E
SDB; Merkblatt 8 - E 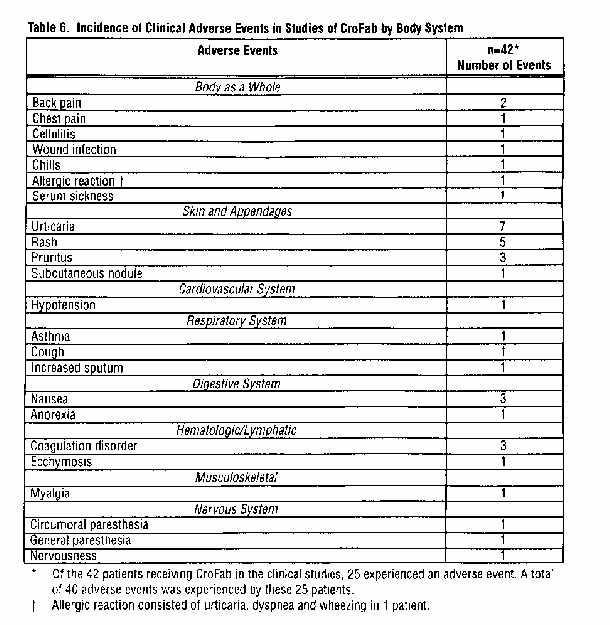
 SDB; Merkblatt 8 - E
SDB; Merkblatt 8 - E