Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
Horseback riding in children with cerebral palsy: effect on gross motor function
We define sports therapy as the enjoyment of any sport whichresults in improvements in gross motor function for individ-
uals having neurological disorders or developmental disabil-ities. The introduction of sports therapy in the early formativeyears may have a significant impact on accelerating the reha-
bilitation of children with neurological disorders or develop-mental disabilities, such as cerebral palsy (CP).
CP is a chronic condition often requiring lifelong participa-
tion in physical and occupational therapy (PT, OT). In additionto standard PT and OT to improve motor function, it has beenour clinical experience that parents often inquire about sports
John A Sterba* MD PhD, Center for Sports Therapy
therapy programs for their children. Recommendations for
sports therapy should consider safety, enjoyment, and results
of published evidence-based research on its effectiveness.
Unfortunately, there are very few published studies measuring
Deborah A Vokes OTR, Robert Warner Rehabilitation Center,
the effects of sports therapy programs, such as horseback rid-
Children’s Hospital of Buffalo, Buffalo, NY, USA.
ing, on improving gross motor function in children with neuro-logical disorders or developmental disabilities.
*Correspondence to first author at Center for Sports
In adults with mental retardation,* horseback riding has
Therapy Research, Inc., 226 Center Road, East Aurora,
been demonstrated to result in improvements in standing and
quadruped balance (Biery et al. 1989). In adults with various
disabilities, including CP, horseback riding has also beenshown to produce improvements in arm and leg coordination(Brock 1988). Bertoti (1988), using a self-designed, posturalassessment scale, documented improvement in posture ineight of 11 children with CP following a horseback riding peri-
The effects of recreational horseback riding therapy (HBRT)
od of 10 weeks, with riding conducted in twice-weekly one
on gross motor function in children with cerebral palsy (CP:
hour sessions. Bertoti recommended further studies to inves-
spastic diplegia, spastic quadriplegia, and spastic hemiplegia)
tigate the effect of horseback riding on range of motion, bal-
were determined in a blinded study using the Gross Motor
ance, weight shift, and strength in children with CP.
Function Measure (GMFM). Seventeen participants (nine
The purpose of our study was to measure the effect of
females, eight males; mean age 9 years 10 months, SE 10
horseback riding on gross motor function in children with
months) served as their own control. Their mean Gross Motor
CP using an accepted and validated outcome measure: the
Function Classification System score was 2.7 (SD 0.4; range 1
Gross Motor Function Measure (GMFM; Russell et al. 1989,
to 5). HBRT was 1 hour per week for three riding sessions of
6 weeks per session (18 weeks). GMFM was determined every
6 weeks: pre-riding control period, onset of HBRT, every 6
weeks during HBRT for 18 weeks, and 6 weeks following
HBRT. GMFM did not change during pre-riding control
Seventeen children diagnosed with CP who were aged 4 years
period. GMFM Total Score (Dimensions A–E) increased 7.6%
or older were identified as candidates for horseback riding
(p<0.04) after 18 weeks, returning to control level 6 weeks
therapy (HBRT) through the Center for Sports Therapy
following HBRT. GMFM Dimension E (Walking, Running,
Research, in conjunction with two local therapeutic horse-
and Jumping) increased 8.7% after 12 weeks (p<0.02), 8.5%
back riding centers in western New York State, USA. Four years
after 18 weeks (p<0.03), and remained elevated at 1.8% 6
was determined as the ideal age to begin horseback riding by a
weeks following HBRT (p<0.03). This suggests that HBRT
multidisciplinary group of administrators in both health and
may improve gross motor function in children with CP, which
education and therapeutic horseback riding instructors with
may reduce the degree of motor disability. Larger studies are
the North American Riding for the Handicapped Association
needed to investigate this further, especially in children.
(NARHA 1998). Seventeen was the maximum number of chil-
with more severe disabilities. Horseback riding should be
dren with CP that the two horseback riding centers could
considered for sports therapy in children with CP.
Participants comprised nine females and eight males, mean
age 9 years 10 months, SE 10 months with a diagnosis of spas-tic diplegic (n=12), spastic quadriplegic (n=3), or spastichemiplegic (n=2) CP. Mean GMFCS score was 2.7 (SE 0.4)range 1 (higher function) to 5 (lower function). The numberof children for each GMFCS Level was: Level I (n=3); Level II(n=7); Level III (n=2); Level IV (n=2); and Level V (n=3). Amajority of riders (n=12) were ambulatory (GMFCS Levels I toIII) and five were non-ambulatory (GMFCS Levels IV and V). Demographic and clinical data are summarized in Table I.
*North American usage. UK usage: learning disability. Developmental Medicine & Child Neurology 2002, 44: 301–308
Families of the participants were advised about the study,
for 18 weeks, and 6 weeks following the completion of horse-
including risks and benefits, before giving written consent.
back riding. Individual riders served as their own control par-
Approval for this study was obtained from the Institutional
ticipants in this study. After the age of 6 years, children with CP
Review Board of the Children’s Hospital of Buffalo, USA. In
do not usually make substantial changes in their gross motor
conjunction with the Children’s Hospital of Buffalo and the
abilities as measured by the GMFM (Palisano et al. 2000),
Robert Warner Rehabilitation Center of Buffalo, the children
therefore, our study attempted to determine if horseback rid-
were screened and examined by a developmental pediatrician
ing over a relatively brief period of time (18 weeks) would
who performed a health history and physical examination.
The degree of disability for all riders was determined by the
Treatment was conducted at two local therapeutic horse-
Gross Motor Function Classification System (GMFCS; Palisano
back riding centers in western New York State. Therapeutic
et al. 1997). The GMFCS was reported to be quick and easy to
riding instruction was conducted by trained individuals,
use, valid, and reliable among 48 physical and occupational
accredited by NARHA, based on their knowledge of the rid-
therapists and developmental pediatricians, all with expertize
ers’ disabilities and in the methods for safely using trained,
therapeutic riding horses. Both riding centers followed the
The Children’s Functional Independence Measure (WeeFIM;
same comprehensive therapeutic riding lesson plans set forth
Braun et al. 1991) was used to determine the riders’ level
by the NARHA Curriculum for Riding Therapy and therapeutic
of independence in self-care, sphincter control, transfer ability
riding procedures, precautions, and contraindications by
(e.g. to and from a wheelchair), locomotion, communication,
the NARHA Operating Center Standards and Accreditation
and social cognition (Braun et al. 1991). When compared with
(NARHA 1999). (NARHA resource information available at:
the Vineland Adaptive Behavior Scale (Sparrow et al. 1984),
the WeeFIM has high sensitivity and specificity (Dittmar et al.
In this study, both therapeutic riding centers conducted
1997) and is both valid and reliable (McCabe et al. 1990).
only recreational, therapeutic horseback riding, not hip-
To study the effect of horseback riding on gross motor
potherapy. The term hippotherapy, derived from the Greek
function in children with CP required a systematic assess-
word ‘hippos’ meaning horse, is defined by the NARHA Special
ment of each child in a standardized manner to evaluate
Interest Section, the American Hippotherapy Association as a
functional activities and gross motor milestones. The GMFM
form of treatment performed by health professionals, such
has been demonstrated to have high levels of validity, reliabil-
as physical and occupational therapists and others, in which
ity, and responsiveness in assessing motor function and the
the horse is used as a therapeutic intervention (NARHA
effects of physical therapy in children with CP (Russell et al.
1989, Bjornson et al 1998). Therefore, the GMFM was cho-
Horseback riding therapy was conducted at both horseback
sen as the tool to measure any clinical changes in the partici-
riding centers for 1 hour per week, 6 weeks per session for
three consecutive riding sessions: totaling 18 weeks of riding.
Specifically, the GMFM consists of 88 items organized into
All 17 riders achieved 18 riding sessions with replacement ses-
five Dimensions: (A) Lying and Rolling; (B) Sitting; (C) Crawling
sions being attended if there was any absence. In each riding
and Kneeling; (D) Standing; and (E) Walking, Running, and
class, the instructor followed target objectives for developing
Jumping. The levels of each item are explicitly defined and
sensory–motor and perceptual–motor skills. These objectives
scored on a scale of 0 to 3. Item scores are summed to yield
were used by the instructors to select various tasks and activi-
scores for each Dimension that reflect the percent of the total
ties during each riding class, following the Developmental
possible score for that Dimension achieved by each child. The
Riding Therapy methods of Spink (1993): riders sit directly on
Total GMFM score is derived by averaging the percent scores
a horse blanket or a saddle, while the instructors select various
for all five Dimensions (A through E), in accordance with the
tasks that are based on the child’s individual needs (see below).
GMFM training manual (Russell et al. 1993).
Riders were seated on the horse and directed by the
The GMFM measurements were conducted at the Children’s
instructor to touch various parts of the horse’s body, such as
Hospital of Buffalo by physical and occupational therapists
the horses’ mane, or flank, or reach behind to touch the hors-
trained and clinically experienced in the GMFM. All thera-
es’ back with either hand. The riders could also lie prone
pists in our study surpassed the interrater reliability testing
over the horse’s back, comfortably positioned on a horse
criterion (0.80), achieving a score of 0.95. All therapists also
blanket with a handhold by use of a vaulting surcingle. The
maintained clinical competency using the GMFM before test-
horse initially remained still and then began walking slowly.
ing any of the children in our study. To eliminate bias, these
While seated on a horse blanket or saddle, the riders reached
therapists were not involved in HBRT. Furthermore, none of
for an object or patted the horse on either side of the its mid-
the authors of this paper were present during the GMFM
line. Riders reached for an object, such as a ring, across their
evaluations. All therapists were kept blinded to the horse-
midline and the horse’s body using one or both hands
back riding conditions and regimen for the children as well
together. Riders imitated movements first made by the instruc-
tor such as arms abducted or bilateral arm circles, forward orbackward (Fig. 1). Riders were directed to hold a stick hori-
zontally with both hands, raising and lowering the stick with
The independent variable was the introduction of horseback
proper postural alignment. While the rider held two sticks in
riding as an additional therapy, beyond traditional PT and OT.
both hands, the instructor transferred rings between the
The 17 riders were evaluated by GMFM 6 weeks before riding,
sticks. Road construction cones were placed in the riding
at the onset of riding, every 6 weeks during the riding period
area and while the horse was led, the rider attempted to hit
Developmental Medicine & Child Neurology 2002, 44: 301–308
the cones by tossing beanbags or place large rings around
ers for assistance and support. Instructors determined that the
five non-ambulatory children required back-riders or double
All riders’ safety was always ensured: they wore fitted
side-walkers for assistance in postural, truncal support, and
helmets and used chinstraps. One or two side walkers used
hand-over-hand encouragement when reaching, grasping,
various side-helping techniques. If the rider was more physi-
twisting, or performing other maneuvers during the therapeu-
cally challenged, a back-rider was used to sit directly behind
tic riding session. The five non-ambulatory riders performed
the child, helping to maintain upright posture. The instruc-
all the same tasks as the other participants with less disability
tor stood nearby and directed the therapy, always monitor-
(GMFCS Levels I to III), none of whom used a back-rider.
ing the movement and behavior of the horse. A waist straparound the rider was occasionally used by side-walkers or
the back-rider to provide a comfortable handgrip .
One-way ANOVA with repeated measures using actual scores
The horse was led at a controlled walk by a trained assis-
for each child and the post-hoc Bonferroni test was used to
tant directing the horse with a lead line attached to its halter.
determine statistical significance which was set at p<0.05.
As therapy progressed, less support was needed from theside-walkers or the back-rider. While the rider was most
often lying or sitting directly on the warm horse blanket or
Analysis of the relation between GMFCS Level and changes in
occasionally using a saddle, the instructor directed various
GMFM could not be performed due to the small numbers of
exercises of stretching, balance, and posture as detailed
above. These exercises were performed as the horse was led
For all riders, PT frequency was consistently 2.5 (SD 0.2)
in a slow, steady walk, with the rider responding to the three-
times per week and OT frequency was 2.2 (SD 0.2) times per
week throughout the entire study. Of 17 riders, a majority
The five riders who were non-ambulatory (GMFCS Levels
(n=13) had previous horseback riding experience. Five riders
IV and V) were positioned on the horse in the straddle posi-
had previous orthopedic surgeries, many with multiple ortho-
tion using a horse blanket and a surcingle, not a saddle.
pedic surgeries: three riders with hamstring lengthening, two
Two of these five riders (both GMFCS Level V) needed a back
riders with Achilles tendon lengthening, two riders with hip
rider, whereas the other three riders (two riders GMFCS Level
osteotomies, and one rider with femoral hip resection and
IV and one rider GMFCS Level V) only required two side-walk-
adductor release. Four of the children had neurological surg-
Figure 1: Rider performs arm exercises during horseback riding therapy, assisted by two side-walkers and a lead walker. (Photo from Equistar Therapeutic Riding Center, Appleton, NY. Reproduced with permission.)
Horseback Riding and Gross Motor Function John A Sterba et al.
eries, including three with selective rhizotomies and one with a
WeeFIM (Braun et al. 1991) Motor, Cognitive, and Total
ventricular peritoneal shunt. Ten of the riders wore ankle–foot
scores did not change before, during, or following HBRT.
orthoses. Only two of the children were on medication: one
Absolute values for pre-riding WeeFIM Scores for all 17 riders
rider was taking sodium valproate and valproic acid, acetazo-
were: WeeFIM Motor, 58.1 (SD 7.4); WeeFIM Cognitive, 22.4
lamide, sodium cromoglycate, and albuterol; the other rider
(SD 3.2); WeeFIM Total Score, 80.5 (SD 22.4).
was taking phenobarbital, baclofen, and ranitidine.
From 6 weeks before riding to the onset of riding therapy,
Table I: Participant characteristics (n=17)
O, orthopedic; bilat, bilateral; N, neurological; VP, ventricular peritoneal; AFO, ankle–foot orthosis; sd valp/valp ac, sodium valproate andvalproic acid; sd cromogly, sodium cromoglycate. Developmental Medicine & Child Neurology 2002, 44: 301–308
there were no differences in any of the five GMFM Dimension
control the horse but is directly influenced by, and responds to
scores or the GMFM Total Score, averaged as control data. After
movements by the horse (Potter et al. 1994). The warmth of
one session (6 weeks), there was no difference, but after two
the horse through the blanket plus the rhythmical movements
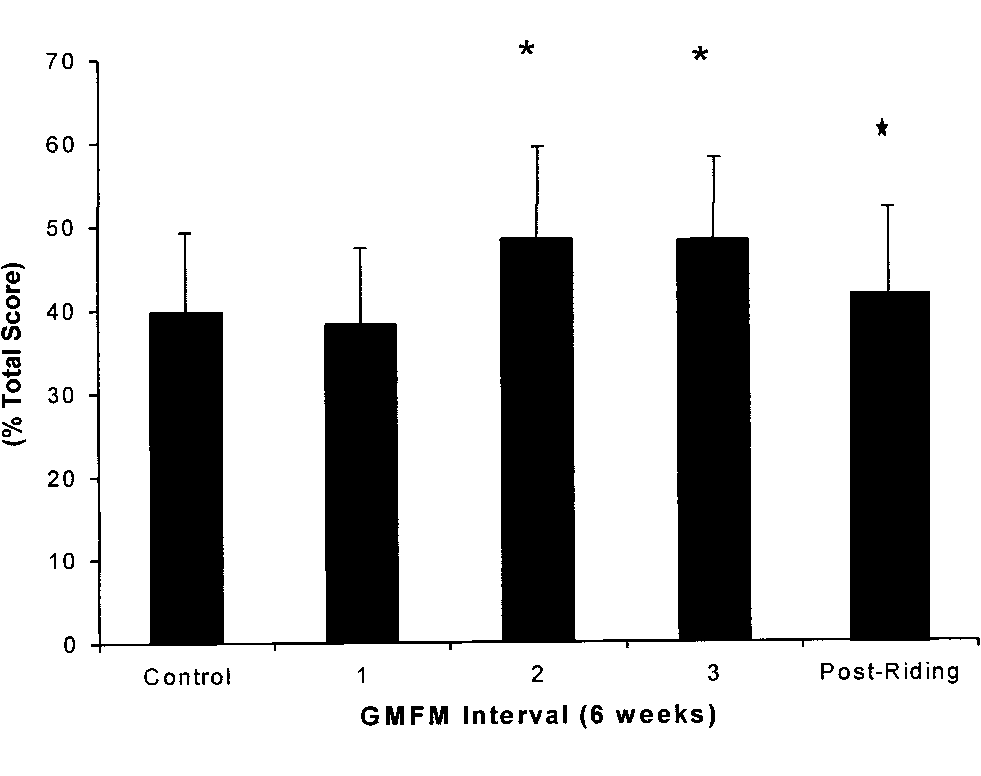
sessions (12 weeks) of HBRT, GMFM Dimension E (Walking,
of the horse have been speculated to improve circulation,
Running, and Jumping) increased significantly (8.7%; p<0.02)
reduce abnormally high muscle tone, and promote relaxation
and remained elevated (8.5%; p<0.03) after three sessions (18
in children with spastic CP (DePauw 1986, Bertoti 1988). In
weeks). Six weeks following the HBRT post-riding period,
addition, the sensation of rhythmic movement along with
GMFM Dimension E remained elevated (1.8%; p<0.03; see Fig
other therapy techniques on the horse can be used to facilitate
2). The power of the performed test with alpha=0.05 was
and improve co-contraction, joint stability, weight shift, and
0.803, which was above the desired power of 0.8.
postural and equilibrium responses in children with CP
After 3 sessions (18 weeks) of HBRT, GMFM Total Score
(Bertoti 1988). In our study, GMFM Dimension B (Sitting),
(Dimensions A–E) increased (7.6%; p<0.04) but returned to
which is related to posture, showed only a 4.1%, non-signifi-
pre-riding levels 6 weeks following HBRT in the post-riding
cant (p<0.1) improvement. We speculate that evaluating a
period (pre-riding: 62.4% [SD 7.8]; post-riding: 60.5% [SD9.3] ns; see Fig 3). The power of the performed test withalpha=0.05 was 0.759, which was just below the desiredpower of 0.8.
Table II summarizes the results of GMFM Dimension E
There were no significant changes in GMFM Dimension
A (Lying and Rolling), Dimension B (Sitting), Dimension C
(Crawling and Kneeling), or Dimension D (Standing). Closeinspection of the data revealed that GMFM Dimension B
appeared to steadily increase from pre-riding levels (75.2%, SD8.2) to the end of 18 weeks of HBRT (79.3%, SD 8.4). This 4.1%
increase, however, did not quite reach statistical significance
(p=0.1). Six weeks following HBRT, GMFM Dimension B was
observed to decrease (74.2%, SD 8.7), but was not significantly
different from pre-riding levels (75.2%, SD 8.2).
Historically, horseback riding has been subjectively described
by physicians and therapists in medical literature dating backto the second century (e.g. Galen c129 to c200, Oribasius 1555,
Figure 2: GMFM Dimension E (Walking, Running, and
Fuller 1705, Quellmaltz 1735, van Swienten 1776, Chassaigne
Jumping). After two, 6-week long riding sessions, GMFM
1870: see Baine 1965) as a beneficial form of therapy for
Dimension E increased 8.7% (*p<0.02) and after three
patients with various neurological disabilities. Without a sensi-
sessions increased 8.5% (**p<0.03). Six weeks post-riding,
tive tool such as the GMFM, none of these authors were able to
Dimension E remained elevated at 1.8% (***p<0.03).
measure the clinical efficacy of horseback riding as therapy.
There are no further references in the literature to the use
of horseback riding as a form of therapy until two serious epi-demics of paralytic poliomyelitis in Scandinavia in 1946. These events led to the founding of the first two centers oftherapeutic horseback riding in Copenhagen, Denmark and
Oslo, Norway for the treatment of children with neuromus-
cular disorders, especially poliomyelitis and CP (Baine 1965).
From 1953 onward, therapeutic horseback riding was
actively promoted by the International Polio Fellowship in
England (Baine 1965). This international momentum for
HBRT led to the development of the first therapeutic riding
program in North America established in Toronto, Canada in1965 as the Community Association for Riding for the
Disabled (CARD; Brock 1988, Mackay-Lyons et al. 1988). The
North American Riding for the Handicapped Association
(NARHA) was founded in 1969 to support riders from both
Horseback riding therapy is directed towards improving
the rider’s ability to receive and process body-wide sensoryinformation from the smooth, rhythmical movements madeby the horse (Spink 1993). By placing the rider on the horse
Figure 3: GMFM Total Score (Dimensions A–E) after three, 6-
using a soft blanket in various body positions (e.g. prone,
week long riding sessions. GMFM Total Score increased 7.6%
supine, side lying, side sitting, or sitting) the rider does not
(*p<0.04), returning to pre-riding 6 weeks post-riding (ns).
Horseback Riding and Gross Motor Function John A Sterba et al.
larger number of children in future HBRT may reveal signifi-
the trunk of the rider, likely activating lateral flexors (Spink
cant improvement in GMFM Dimension B.
1993). According to Spink (1993), the four functional stages
Although similar to the use of therapeutic devices used in
of motor control detailed by Bobath and Bobath (1975),
the clinic, such as the bolster swing or Swiss ball, horseback
namely uncontrolled mobility, proximal mobility on distal
riding offers more sensory–motor stimulation and a bond
stability, distal mobility on proximal stability, and locomotion,
between rider and horse that cannot be simulated artificially
may all be stimulated with therapeutic horseback riding.
in the clinic or with an inanimate horse. As suggested by
Following our study, we inquired with each family which
MacKinnon and colleagues (1995), horseback riding pro-
factors, such as program costs or time, influenced or limited
vides the rider who has a disability with a sensory–motor
further participation in HBRT. All riders and their families
experience that contributes to the development, mainte-
thoroughly enjoyed the horseback riding experience. Our
nance, rehabilitation, and enhancement of various sensory
informal survey revealed the most important limiting factor
was available time, not registration fees, transportation costs,
Those who have supported therapeutic horseback riding
or accessibility issues. Families uniformly complained about
have collectively suggested these possible therapeutic benefits:
not having enough time for daily care issues with consider-
(1) mobilization of the pelvis, lumbar spine, and hip joints, (2)
able time being lost driving their children to and from various
normalization of muscle tone, (3) development of head and
therapy and physician appointments. Lack of medical insur-
trunk postural control, and (4) development of equilibrium
ance reimbursement for HBRT was not an issue in our study.
reactions in the trunk (Chassaigne 1870, Baine 1965; Harpoth
Our research grant paid for GMFM evaluations and reimbursed
1970; Haskin et al. 1974; Freeman 1984; Bertoti 1988, 1991).
parents for the horseback riding registration fees. All parents,
Our results using the GMFM now demonstrate that horseback
however, inquired whether medical insurance would ever pay
riding as therapy is associated with improvements in total gross
for this form of sports therapy. They also agreed that they
would pay privately for HBRT, despite the lack of medical insur-
In the 17 children with CP, HBRT was associated with
ance reimbursement, due to observable improvements that
improvements in gross motor function, not only in the
were seen not only in gross motor function, but in speech, self-
GMFM Total Score but with improvements in the GMFM
esteem, and emotional well-being as well as a perceived high
Dimension E (Walking, Running, and Jumping), which per-
degree of enjoyment by all the children in our study. These
sisted 6 weeks after the completion of horseback riding.
other benefits of horseback riding are very important and have
It is hypothesized that the complex movement of the
been previously described in children and adults (Brock 1988,
horse influences the rider by passive and active stretching
Spink 1993, MacKinnon 1995). All families suggested that once
and stimulation of the rider’s balance and postural control.
per week would be the maximum time their child would be
The movement of the rider’s pelvis in response to the horse’s
able to participate in future HBRT, due to personal time con-
gait has been described to resemble the movement of the
straints. This is also the usual regimen for recreational HBRT in
pelvis during normal human gait (Bertoti 1988, Spink 1993,
Potter et al. 1994, MacPhail et al. 1998). It is hypothesized
Our results extend a recently reported finding in a pilot
that these movements enhance the rider’s function during
study of hippotherapy in five children with CP by McGibbon
gait and gait-related activity. The primary horse movements
and coworkers (1998). They demonstrated that after 8
have been found to be correlated with the automatic physical
weeks of hippotherapy (conducted twice weekly, one hour
reaction of the rider in the three components of movement
per session), there was a significant improvement in GMFM
of the human body, i.e. static/dynamic, weight-shift, and rota-
Dimension E. However, there was no improvement seen in
tional components (Spink 1993). During the horse’s slow
the GMFM Total Score and no documented percent change
walk, all three components occur within the rider’s trunk
was reported for GMFM Dimension E. No follow-up study
and pelvis simultaneously (Spink 1993). The horse’s gait
was conducted to determine any carry-over effects following
moves the rider forward and backward, causing anterior and
hippotherapy. This pilot study may also have been limited by
posterior tilt of the pelvis. This process is thought to stimu-
a small sample size (n=5) and biased with the the physical
late the rider to develop control of the trunk via flexors and
therapist conducting both the hippotherapy and the GMFM
extensors. Likewise, the horse’s movement side-to-side causes
reciprocal activation of the rider’s lateral flexors of the trunk
Confounding variables may have also influenced our
and may develop further trunk stability. The rotational compo-
results. We questioned whether the novelty of the horseback
nent of the horse’s movement are believed to cause rotation in
riding experience might have contributed to the measurable
Developmental Medicine & Child Neurology 2002, 44: 301–308
improvements in total gross motor function and persistent
changes in walking, running, and jumping. However, a
Sports therapy is the enjoyment of a sport, such as horseback
majority of the children in our study (13 of 17) had previous
riding, which results in significant improvements in gross
horseback riding experience. It is possible that children not
motor function. In a heterogeneous group of children with
yet exposed to horseback riding may demonstrate an even
mild to severe CP, horseback riding clinically improved over-
greater improvement in gross motor function.
all gross motor function, especially walking, running, and
Our data cannot be explained as a therapeutic effect from
jumping, which persisted following HBRT. These significant
ongoing PT or OT. Horseback riding was introduced as an
results, which should be confirmed in further research, have
independent variable, in addition to PT and OT which were
provided clinical evidence of a possible reduction in gross
consistently conducted throughout the entire study. In addi-
motor disability in children with CP. Horseback riding should
tion, repetitive GMFM measurements would not produce any
be considered for sports therapy for the medical rehabilita-
training effect to increase GMFM scores systematically over
the 6-week intervals used in our 30-week study (Rosenbaum,personal communication, 2000). Accepted for publication 14th November 2001.
We considered a criticism of whether this observed thera-
peutic effect from recreational horseback riding might be due
to ‘fun only’ and not the therapeutic effect of movement on the
This research was supported by a medical rehabilitation research
horse. When we inquired whether these and other families
grant from the Children’s Guild, Inc., Buffalo, NY. We would like toextend our appreciation to Mrs Gloria A Favero, Administrative
would consider allowing their children to participate in a
Secretary of the Department of Occupational and Physical Therapy,
future experiment with simulated horse movements, using a
Children’s Hospital of Buffalo, for assisting families and scheduling
wooden horse with ropes and pulleys, all families declined. If it
all the GMFM appointments. We would also like to thank Mary Lane
isn’t ‘fun’, children will not participate in therapy, which most
Dip P & OT, for GMFM training and Peter L Rosenbaum MD for
pediatric physical and occupational therapist know.
reviewing our manuscript. This research was presented at the 54thAnnual Meeting of the American Academy for Cerebral Palsy and
Initially, we questioned whether lack of a control group of
Developmental Medicine, Toronto, Ontario, Canada, 20–23
non-riders might have limited our study design. All of the rid-
ers in this study served as their own control. This is a verysensitive way to determine even small therapeutic changes,
such as the observed improvement in GMFM Dimension E
Baine A. (1965) Pony riding for the disabled. Physiotherapy51: 263–5.
(Walking, Running, and Jumping) of only 1.8% (p<0.03), 6
Bertoti DB. (1988) Effect of therapeutic horseback riding on posture
weeks following horseback riding. This study design of an
in children with cerebral palsy. Physical Therapy8: 1505–12.
interventional, before–after trial with participants serving as
Bertoti DB. (1991) Clinical suggestions. Effect of therapeutic
their own control is useful in the GMFM evaluation of sports
horseback riding on extremity weight bearing in a child withhemiplegic cerebral palsy: a case report as an example of clinical
research. Pediatric Physical Therapy 3: 219–24.
Our study represents a functional clinical gain in walking,
Biery MJ, Kauffman N. (1989) The effects of therapeutic horseback
running, and jumping plus an overall improvement in gross
riding on balance. Adapted Physical Activity Quarterly 6: 221–9.
motor function in a heterogeneous group of 17 riders, five of
Bjornson KF, Graubert CS, Buford VL, McLaughlin J. (1998) Validity of
the Gross Motor Function Measure. Pediatric Physical Therapy
whom were non-ambulatory (GMFCS Levels IV and V). In
these five, non-ambulatory riders, no changes were observed
Bobath B, Bobath K. (1975) Motor Development in the Different
in Dimension E (Walking, Running, and Jumping) or in the
Types of Cerebral Palsy. London: White Friars.
other GMFM Dimensions, collectively. Excluding the GMFM
Braun S, Msall ME, Granger CV. (1991) Manual for the Functional
data from these five non-ambulatory children did not
Independence Measure for Children (WeeFIM) Version 1.4. Buffalo, New York: Center for Functional Assessment Research,
demonstrate any further significant changes in our results.
Uniform Data System for Medical Rehabilitation, State University of
Although non-ambulatory children may be less likely to show
improvements in Dimension E, future studies are needed
Brock BJ. (1988) Effect of therapeutic horseback riding on physically
with larger numbers of children to investigate specifically the
disabled adults. Therapeutic Recreation Journal 2: 34–43.
Chassaigne R. (1870) Physiologie de l’equitation, de son
functional gains of horseback riding in a group of children
application a l’hygiene et a la therapeutic. Thesis. University of
with more severe disabilities in GMFCS Levels IV and V.
We also recommend further research with a greater num-
DePauw KP. (1986) Horseback riding for individuals with
ber of riders with CP in each of the GMFCS Levels for two rea-
disabilities: programs, philosophy, and research. Adapted
sons: to confirm our observed positive clinical effects of
Physical Activity Quarterly 3: 217–26.
Dittmar SS, Gresham GE, editors. (1997) Functional Assessment
horseback riding as sports therapy and to determine whether
and Outcome Measures for the Rehabilitation Professional.
the severity of the child’s motor impairment (GMFCS Level)
Gaithersburg, MD: Aspen Publication.
is related statistically to the changes detected by GMFM.
Heipertz W. (1981) Therapeutic Riding: Medicine, Education,
Furthermore, a longer post-riding recovery phase is needed
Sports. Ottawa, Canada: National Printers.
Freeman G. (1984) Hippotherapy/therapeutic horseback riding.
to determine how much longer this observed clinical
Clinical Management in Physical Therapy 4: 20–5.
improvement in GMFM Dimension E (Walking, Running,
Harpoth U. (1970) Horseback riding for handicapped children. Physical Therapy 50: 235–6.
CP is a chronic condition that often results in lifelong
Haskin MR, Erdman WJ, Bream J. (1974) Therapeutic horseback
participation in physical and occupational therapy. Sports ther-
riding for the handicapped. Archives of Physical MedicalRehabilitation 55: 473–4.
apy, such as HBRT, offers additional opportunities for children
MacKay-Lyons M, Conway C, Roberts W. (1988) Effects of
with CP to have fun and receive medical rehabilitation with a
therapeutic riding on patients with multiple sclerosis: a
preliminary trial. Physiotherapy Canada 40: 104–9.
Horseback Riding and Gross Motor Function John A Sterba et al.
MacKinnon JR, Noh S, Lariviere J, MacPhail A, Allen DE, Laliberte D.
Palisano R, Rosenbaum P, Walter S, Russell D, Wood E, Galuppi B.
(1995) A study of therapeutic effects of horseback riding for
(1997) Development and reliability of a system to classify gross
children with cerebral palsy. Physical and Occupational Therapy
motor function in children with cerebral Palsy. DevelopmentalMedicine & Child Neurology 39: 214–23.
MacPhail AHE, Edwards J, Golding J, Miller K, Mosier C, Zwiers T.
Palisano RJ, Hanna SE, Rosenbaum PL, Russell DJ, Walter SD, Wood EP,
(1998) Trunk postural reactions in children with and without
Raina PS, Galuppi BE. (2000) Validation of a Model of Gross Motor
cerebral palsy during therapeutic horseback riding. Pediatric
Function for Children with Cerebral Palsy. Physical Therapy Physical Therapy 10: 143–7.
McCabe MA, Granger CV. (1990) Content validity of a pediatric
Potter JT, Evans JW, Nolt Jr, BH. (1994) Therapeutic horseback riding.
functional independence measure. Applied Nursing ResearchJournal of the American Veterinary Association 204: 131–4.
Rosenbaum PL, Russell DJ, Cadman DJ. (1990) Issues in measuring
McGibbon NH, Andrade C-K, Widener G, Cintas HL. (1998) Effect of
change in motor function in children with cerebral palsy: a special
an equine-movement therapy on gait, energy expenditure, and
communication. Physical Therapy 70: 125–31.
motor function in children with spastic cerebral palsy: a pilot study.
Russell DJ, Rosenbaum PL, Cadman, Gowland C, Hardy S, Jarvis S. Developmental Medicine & Child Neurology 40: 754–62.
(1989) The gross motor function measure: a means to evaluate the
North American Riding for the Handicapped Association (NARHA).
effects of physical therapy. Developmental Medicine & Child
(1998) NARHA Membership Brochure, P.O. Box 33150, Denver,
Russell DJ, Rosenbaum PL, Gowland C, Hardy S, Lane M, Plews N,
North American Riding for the Handicapped Association (NARHA)
McGavin H, Cadman D, Jarvis S (1993) Gross Motor Function
(1999) Curriculum for Riding Therapy and Operating Center
Measure Manual. Hamilton, Ontario: Chedoke-McMaster
Standards and Accreditation, P.O. Box 33150, Denver, CO 80233,
Sparrow S, Balla P, Cilcchetti D. (1984) Vineland Adaptive Behavior
North American Riding for the Handicapped Association
Scales, Interview edition: Survey form manual. Circle Pines, MN:
(NARHA)(2000) American Hippotherapy Association, A Special
Interest Section of NARHA Brochure, P.O. Box 33150, Denver, CO
Spink J. (1993) Developmental Riding Therapy: A Team Approach toAssessment and Treatment. Tucson, AZ: Therapy Skill Builders. Developmental Medicine & Child Neurology 2002, 44: 301–308
Management of Alcohol Withdrawal Delirium An Evidence-Based Practice Guideline Michael F. Mayo-Smith, MD, MPH; Lee H. Beecher, MD; Timothy L. Fischer, DO; David A. Gorelick, MD, PhD;Jeanette L. Guillaume, MA; Arnold Hill, MD; Gail Jara, BA; Chris Kasser, MD; John Melbourne, MD;for the Working Group on the Management of Alcohol Withdrawal Delirium,Practice Guidelines Committee, American So
POSTTRANSPLANT TREATMENT AND MEDICATIONS Methylprednisolone (Solu-Medrol®)/Prednisone Day 1: 2 x 50 mg Day 2: 2 x 40 mg Day 3: 2 x 30 mg Day 4: 2 x 20 mg Day 5: 2 x 10 mg Day 6 to end of third week: 20 mg Week 4: 17.5 mg Month 2: 15 mg Month 3: 10 mg Month 4: 7.5 mg Month 6: 5 mg which is then titrated down to 2.5 mg at a time every two weeks until disconti
 the cones by tossing beanbags or place large rings around
ers for assistance and support. Instructors determined that the
five non-ambulatory children required back-riders or double
All riders’ safety was always ensured: they wore fitted
side-walkers for assistance in postural, truncal support, and
helmets and used chinstraps. One or two side walkers used
hand-over-hand encouragement when reaching, grasping,
various side-helping techniques. If the rider was more physi-
twisting, or performing other maneuvers during the therapeu-
cally challenged, a back-rider was used to sit directly behind
tic riding session. The five non-ambulatory riders performed
the child, helping to maintain upright posture. The instruc-
all the same tasks as the other participants with less disability
tor stood nearby and directed the therapy, always monitor-
(GMFCS Levels I to III), none of whom used a back-rider.
ing the movement and behavior of the horse. A waist straparound the rider was occasionally used by side-walkers or
the back-rider to provide a comfortable handgrip .
One-way ANOVA with repeated measures using actual scores
The horse was led at a controlled walk by a trained assis-
for each child and the post-hoc Bonferroni test was used to
tant directing the horse with a lead line attached to its halter.
the cones by tossing beanbags or place large rings around
ers for assistance and support. Instructors determined that the
five non-ambulatory children required back-riders or double
All riders’ safety was always ensured: they wore fitted
side-walkers for assistance in postural, truncal support, and
helmets and used chinstraps. One or two side walkers used
hand-over-hand encouragement when reaching, grasping,
various side-helping techniques. If the rider was more physi-
twisting, or performing other maneuvers during the therapeu-
cally challenged, a back-rider was used to sit directly behind
tic riding session. The five non-ambulatory riders performed
the child, helping to maintain upright posture. The instruc-
all the same tasks as the other participants with less disability
tor stood nearby and directed the therapy, always monitor-
(GMFCS Levels I to III), none of whom used a back-rider.
ing the movement and behavior of the horse. A waist straparound the rider was occasionally used by side-walkers or
the back-rider to provide a comfortable handgrip .
One-way ANOVA with repeated measures using actual scores
The horse was led at a controlled walk by a trained assis-
for each child and the post-hoc Bonferroni test was used to
tant directing the horse with a lead line attached to its halter.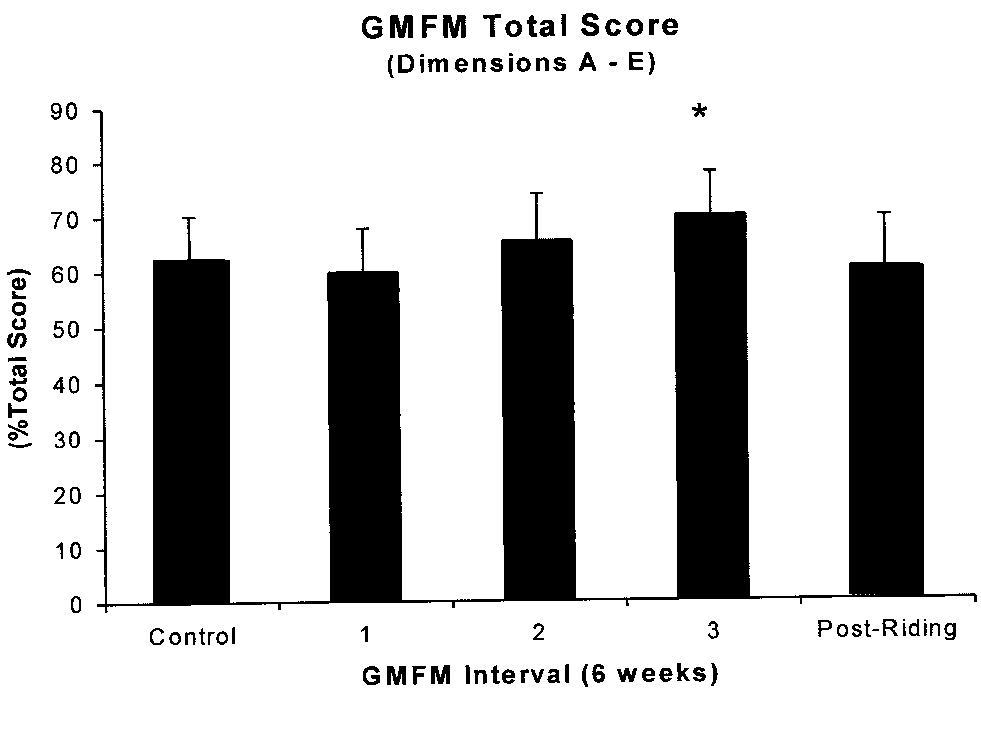
 there were no differences in any of the five GMFM Dimension
control the horse but is directly influenced by, and responds to
scores or the GMFM Total Score, averaged as control data. After
movements by the horse (Potter et al. 1994). The warmth of
one session (6 weeks), there was no difference, but after two
the horse through the blanket plus the rhythmical movements
sessions (12 weeks) of HBRT, GMFM Dimension E (Walking,
of the horse have been speculated to improve circulation,
Running, and Jumping) increased significantly (8.7%; p<0.02)
reduce abnormally high muscle tone, and promote relaxation
and remained elevated (8.5%; p<0.03) after three sessions (18
in children with spastic CP (DePauw 1986, Bertoti 1988). In
weeks). Six weeks following the HBRT post-riding period,
addition, the sensation of rhythmic movement along with
GMFM Dimension E remained elevated (1.8%; p<0.03; see Fig
other therapy techniques on the horse can be used to facilitate
2). The power of the performed test with alpha=0.05 was
and improve co-contraction, joint stability, weight shift, and
0.803, which was above the desired power of 0.8.
there were no differences in any of the five GMFM Dimension
control the horse but is directly influenced by, and responds to
scores or the GMFM Total Score, averaged as control data. After
movements by the horse (Potter et al. 1994). The warmth of
one session (6 weeks), there was no difference, but after two
the horse through the blanket plus the rhythmical movements
sessions (12 weeks) of HBRT, GMFM Dimension E (Walking,
of the horse have been speculated to improve circulation,
Running, and Jumping) increased significantly (8.7%; p<0.02)
reduce abnormally high muscle tone, and promote relaxation
and remained elevated (8.5%; p<0.03) after three sessions (18
in children with spastic CP (DePauw 1986, Bertoti 1988). In
weeks). Six weeks following the HBRT post-riding period,
addition, the sensation of rhythmic movement along with
GMFM Dimension E remained elevated (1.8%; p<0.03; see Fig
other therapy techniques on the horse can be used to facilitate
2). The power of the performed test with alpha=0.05 was
and improve co-contraction, joint stability, weight shift, and
0.803, which was above the desired power of 0.8.