Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
Priftin (rifapentine)
HIGHLIGHTS OF PRESCRIBING INFORMATION ————————————— WARNINGS AND PRECAUTIONS ————————————— These highlights do not include all the information needed to use PRIFTIN® safely and
• Do not use as a once weekly Continuation Phase regimen with isoniazid in HIV seropositive
effectively. See full prescribing information for PRIFTIN.
patients due to the risk of failure and/or relapse with rifampin-resistant organisms. (5.1, 14)
• Co-administration with Protease Inhibitors and Reverse Transcriptase Inhibitors. (5.2, 7.1)
Priftin (rifapentine) Tablets
• Higher relapse rates occur in patients with cavitary pulmonary lesions and/or positive sputum
Initial U.S. Approval: 1998
cultures after the initial phase of treatment or those with evidence of bilateral pulmonarydisease: Use cautiously. (5.3)
—————————————— INDICATIONS AND USAGE ——————————————
• Hepatotoxicity: In patients with abnormal liver tests/disease monitor liver tests prior to therapy
• Rifapentine is a rifamycin antimycobacterial indicated for the treatment of pulmonary tuber-
and every 2–4 weeks during therapy. If signs of disease occur or worsen, discontinue therapy.
culosis caused by Mycobacterium tuberculosis in combination with one or more antitubercu-
• Hyperbilirubinemia: Repeat testing and reassess patient. (5.5)
• Discoloration of body fluids: May permanently stain contact lenses or dentures red-orange. ————————————— DOSAGE AND ADMINISTRATION —————————————
• PRIFTIN has been studied for the treatment of tuberculosis caused by drug-susceptible
• Porphyria: Avoid use in these patients. (5.7)
organisms as part of regimens consisting of an initial 2 month phase followed by a 4 month
• Clostridium difficile-associated colitis: Evaluate if diarrhea occurs. (5.8)
——————————————— ADVERSE REACTIONS ———————————————
• PRIFTIN should not be used alone in either the initial or the continuation phases of
The most common adverse reactions (≥10%) are hyperuricemia, pyuria, hematuria, urinary tract
infection, proteinuria, lymphopenia, neutropenia, anemia, and hypoglycemia. (6.2)
• Initial Phase (2 Months): 600 mg twice weekly for two months by direct observation of therapy,
with an interval of no less than 3 consecutive days (72 hours) between doses, in combination
To report SUSPECTED ADVERSE REACTIONS, contact sanofi-aventis U.S. LLC at 1-800- 633-1610 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch
• Continuation Phase (4 Months): 600 mg once weekly for 4 months by direct observation
therapy with isoniazid or another appropriate antituberculous agent. (2.1)
——————————————— DRUG INTERACTIONS ———————————————
• Concomitant administration of pyridoxine (Vitamin B6) is recommended in order to avoid
• Protease Inhibitors and Reverse Transcriptase Inhibitors. (5.2, 7.1)
INH-associated peripheral neuropathy. (2.2)
• Hormonal Contraceptives: Use another means of birth control. (7.2)
• May increase metabolism and decrease the activity of drugs metabolized by cytochrome P450
3A4 and 2C8/9. Dosage adjustments may be necessary if given concomitantly. (7.3)
———————————— DOSAGE FORMS AND STRENGTHS ———————————— ———————————— USE IN SPECIFIC POPULATIONS ————————————
• Pediatrics: The safety and effectiveness under the age of 12 has not been established. (8.4)
——————————————— CONTRAINDICATIONS ——————————————— See 17 for PATIENT COUNSELING INFORMATION
Known hypersensitivity to any rifamycin. (4.1)
Revised: 05/2010 FULL PRESCRIBING INFORMATION: CONTENTS* USE IN SPECIFIC POPULATIONS INDICATIONS AND USAGE DOSAGE AND ADMINISTRATION DOSAGE FORMS AND STRENGTHS OVERDOSAGE CONTRAINDICATIONS DESCRIPTION WARNINGS AND PRECAUTIONS CLINICAL PHARMACOLOGY
Protease Inhibitors and Reverse Transcriptase Inhibitors
NONCLINICAL TOXICOLOGY
Carcinogenesis, Mutagenesis, Impairment of Fertility
CLINICAL STUDIES Clostridium difficile-Associated Diarrhea
REFERENCES ADVERSE REACTIONS HOW SUPPLIED/STORAGE AND HANDLING
Serious and Otherwise Important Adverse Reactions
PATIENT COUNSELING INFORMATION DRUG INTERACTIONS
Protease Inhibitors and Reverse Transcriptase Inhibitors
*Sections or subsections omitted from the full prescribing information are not listed
FULL PRESCRIBING INFORMATION
PRIFTIN should not be used as monotherapy in either the initial or the continuation phases of
INDICATIONS AND USAGE PRIFTIN® is indicated for the treatment of pulmonary tuberculosis caused by Mycobacterium DOSAGE AND ADMINISTRATION tuberculosis. PRIFTIN must always be used in combination with one or more antituberculosis drugs to which the isolate is susceptible depending on the phase of treatment [see Dosage and Administration
PRIFTIN has been studied for the treatment of tuberculosis caused by drug-susceptible organisms as
Limitations of Use
part of regimens consisting of an initial 2 month phase followed by a 4 month continuation phase.
PRIFTIN should not be used as a once weekly Continuation Phase regimen in combination with
These recommendations apply only to the treatment of patients with drug-susceptible organisms.
isoniazid in HIV seropositive patients with pulmonary tuberculosis because of a higher rate of failure
Initial Phase (2 Months) of short course treatment for pulmonary tuberculosis:
and/or relapse documented with the presence of rifampin-resistant organisms [see Warnings and
PRIFTIN should be administered at a dose of 600 mg (4 × 150 mg tablets) twice weekly for two months
Precautions (5.1) and Clinical Studies (14)].
by direct observation of therapy, with an interval of no less than 3 consecutive days (72 hours) between
PRIFTIN has not been studied as part of the Initial Phase treatment regimen in HIV seropositive
doses, in combination with other antituberculosis drugs as part of an appropriate regimen which
patients with pulmonary tuberculosis.
includes daily companion drugs such as ethambutol, pyrazinamide, and streptomycin.
The determination of the companion drugs to be used should be made by the treating physician and
ADVERSE REACTIONS
depends on the results of susceptibility testing as well as the phase of treatment. PRIFTIN has been
Serious and Otherwise Important Adverse Reactions
studied as part of the initial regimen with isoniazid, pyrazinamide and ethambutol [see Clinical Studies
The following serious and otherwise important adverse drug reactions are discussed in greater detail
Continuation Phase (4 Months) of short course treatment for pulmonary tuberculosis:
• Hypersensitivity [see Contraindications (4.1)]
Following the Initial Phase (2 months), Continuation Phase (4 months) treatment may consist of
• Hepatotoxicity [see Warnings and Precautions (5.4)]
PRIFTIN 600 mg once weekly for 4 months in combination with isoniazid or an appropriate
• Hyperbilirubinemia [see Warnings and Precautions (5.5)]
antituberculosis agent for susceptible organisms by direct observation therapy.
• Discoloration of Body Fluids [see Warnings and Precautions (5.6)]
PRIFTIN was studied as a component of a 4 month continuation phase in conjunction with INH 900
• Porphyria [see Warnings and Precautions (5.7)]
mg once a week in two clinical studies [see Clinical Studies (14)].
• Clostridium difficile-Associated Diarrhea [see Warnings and Precautions (5.8)]
The prescribing physician is directed to current guidelines for further direction on other possible
Clinical Trials Experience
components of the Continuation Phase regimen as well as for directions on extending this phase.
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed
Administration
in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug
Take PRIFTIN with meals. Administration of rifapentine with a meal increases oral bioavailability and
and may not reflect the rates observed in practice.
may reduce the incidence of gastrointestinal upset, nausea, and/or vomiting. [see Clinical Pharma-
The data described below reflect exposure to PRIFTIN in a randomized, open label, active-controlled
trial of patients with pulmonary tuberculosis, excluding those with HIV-infection. The population
In patients with conditions which predispose them to neuropathy (e.g., nutritional deficiency, HIV
consisted of primarily of male subjects with a mean age of 37 ± 11 years. In the initial 2 month phase
infection, renal failure, alcoholism, as well as pregnant and breastfeeding women), concomitant
of treatment (60 days), 361 patients received rifapentine 600 mg twice a week in combination with daily
administration of pyridoxine (Vitamin B6) is recommended in order to avoid INH-associated peripheral
isoniazid, pyrazinamide, and ethambutol and 361 subjects received rifampin in combination with
neuropathy (see American Thoracic Society/Centers for Disease Control/Infectious Disease Society of
isoniazid, pyrazinamide and ethambutol all administered daily. Ethambutol was discontinued when drug
America Guideline for the Treatment of Tuberculosis and Tuberculosis Infection in Adults and Children).
susceptibly testing was completed. During the 4 month continuation phase, 321 patients in the
DOSAGE FORMS AND STRENGTHS
rifapentine group continued to receive rifapentine 600 mg dosed once weekly with isoniazid and 307
PRIFTIN is supplied as 150 mg round normal convex dark-pink film-coated tablets debossed ″Priftin″
patients in the rifampin arm received twice weekly rifampin and isoniazid. Both treatment groups
received pyridoxine (Vitamin B6) over the 6 month treatment period. CONTRAINDICATIONS
Twenty-two deaths occurred in the study (eleven in the rifampin combination therapy group and eleven
Hypersensitivity
in the rifapentine combination therapy group).
PRIFTIN is contraindicated in patients with a history of hypersensitivity to rifamycins.
In the study, 18/361 (5.0%) rifampin combination therapy patients discontinued the study due to an
WARNINGS AND PRECAUTIONS
adverse reaction compared to 11/361 (3.0%) rifapentine combination therapy patients. Three patients
HIV Seropositive Patients
(two rifampin combination therapy patients and one rifapentine combination therapy patient) were
PRIFTIN should not be used as a once weekly Continuation Phase regimen in combination with
discontinued in the Initial Phase as a result of hepatitis with increased liver function tests (ALT, AST,
isoniazid in HIV seropositive patients with pulmonary tuberculosis because of a higher rate of failure
LDH, and bilirubin). Concomitant medications for all three patients included isoniazid, pyrazinamide,
and/or relapse documented with the presence of rifampin-resistant organisms [see Clinical Studies
ethambutol, and pyridoxine. The two rifampin patients and one rifapentine patient recovered without
PRIFTIN has not been studied as part of the Initial Phase treatment regimen in HIV seropositive
As shown in Table 1, hyperuricemia was the most frequently reported reaction and was most likely
patients with pulmonary tuberculosis.
related to the pyrazinamide since only two cases were reported in the Continuation Phase when this
Protease Inhibitors and Reverse Transcriptase Inhibitors
drug was no longer included in the treatment regimen.
Rifapentine is an inducer of CYP450 enzymes. Concomitant use of PRIFTIN with other drugsmetabolized by these enzymes, such as protease inhibitors and reverse transcriptase inhibitors, may
Seven patients had adverse reactions associated with an overdose. In the rifampin combination group
cause a significant decrease in plasma concentrations and loss of therapeutic effect of the protease
these reactions included hematuria, anorexia, back pain, arthralgia, and myalgia. In the rifapentine
inhibitor or reverse transcriptase inhibitor. [see Drug Interactions (7.1 and 7.2) and Clinical Pharma-
combination group these reactions included hematuria, neutropenia, hyperglycemia, ALT increased,
hyperuricemia, pruritus, and arthritis. Relapse of Tuberculosis
The following table (Table 1) presents treatment-emergent adverse reactions associated with the use
PRIFTIN should be used cautiously in subjects with cavitary pulmonary lesions and/or positive sputum
of any of the four drugs in the regimens (rifapentine/rifampin, isoniazid, pyrazinamide, or ethambutol)
cultures after the initial phase of treatment or in those with evidence of bilateral pulmonary disease due
which occurred in ≥1% of patients during treatment and post-treatment through the first three months
to higher rates of relapse. [see Clinical Studies (14)].
Poor compliance with the dosage regimen, particularly during the initial phase in the companionantituberculosis drugs administered with rifapentine, is associated with late sputum conversion and a
Table 1. Treatment-Emergent Adverse Reactions Occurring in ≥1% of Patients
high relapse rate. Therefore, compliance with the full course of therapy must be emphasized, and the
Initial Phase* Continuation Phase† Total‡
importance of not missing any doses must be stressed [see Patient Counseling Information (17)]. Higher relapse rates have also been seen in HIV positive patients receiving PRIFTIN during the
Rifapentine Rifampin Rifapentine Rifampin Rifapentine Rifampin System Organ
continuation phase. Risk factors for relapse included the presence of both pulmonary and extrapul-
Combina- Combina- Combina- Combina- Combina- Combina- Class
monary disease at baseline, low CD4 counts, use of azole antifungals and age (younger) [see Clinicaltion tion tion tion tion tion Preferred (N=361) (N=361) (N=304) (N=317) (N=361) (N=361) Term Hepatotoxicity N(%) N(%) N(%) N(%) N(%) N(%)
Since antituberculous multidrug treatments, including the rifamycin class, are associated with serious
RENAL &
hepatic events, patients with abnormal liver tests and/or liver disease should only be given rifapentine
in cases of necessity and then with caution and under strict medical supervision. In these patients,careful monitoring of liver tests (especially serum transaminases) should be carried out prior to therapy
and then every 2 to 4 weeks during therapy. If signs of liver disease occur or worsen, rifapentine shouldbe discontinued. Hepatotoxicity of other antituberculosis drugs (eg, isoniazid, pyrazinamide) used in
combination with rifapentine should also be taken into account. Hyperbilirubinemia
Hyperbilirubinemia resulting from competition for excretory pathways between rifapentine and bilirubin
cannot be excluded since competition between the related drug rifampin and bilirubin can occur. An
isolated report showing a moderate rise in bilirubin and/or transaminase level is not in itself an indicationfor interrupting treatment; rather, the decision should be made after repeating the tests, noting trends
in the levels and considering them in conjunction with the patient’s clinical condition. Discoloration of Body Fluids
PRIFTIN may produce a predominately red-orange discoloration of body tissues and/or fluids (eg, skin,
METABOLIC &
teeth, tongue, urine, feces, saliva, sputum, tears, sweat, and cerebrospinal fluid). NUTRITIONAL
Contact lenses or dentures may become permanently stained. Porphyria
PRIFTIN should not be used in patients with porphyria. Rifampin has enzyme-inducing properties,
including induction of delta amino levulinic acid synthetase. Isolated reports have associated porphyriaexacerbation with rifampin administration. Based on these isolated reports with rifampin, it may be
assumed that rifapentine has a similar effect. Clostridium difficile-Associated Diarrhea Clostridium difficile-associated diarrhea (CDAD) has been reported with use of nearly all antibacterial
agents, including the rifamycins, and may range in severity from mild diarrhea to fatal colitis. Treatmentwith antibacterial agents alters the normal flora of the colon leading to overgrowth of C. difficile. C. difficile produces toxins A and B which contribute to the development of CDAD. Hypertoxin producingstrains of C. difficile cause increased morbidity and mortality, as these infections can be refractory to
antimicrobial therapy and may require colectomy. CDAD must be considered in all patients who present
with diarrhea following antibiotic use. Careful medical history is necessary since CDAD has been
reported to occur over two months after the administration of antibacterial agents. If CDAD is suspected or confirmed, ongoing antibiotic use not directed against C. difficile may need
HEMATOLOGIC
to be discontinued. Appropriate fluid and electrolyte management, protein supplementation, antibiotic
treatment of C. difficile, and surgical evaluation should be instituted as clinically indicated.Table 1. Treatment-Emergent Adverse Reactions Occurring in ≥1% of Patients Table 1. Treatment-Emergent Adverse Reactions Occurring in ≥1% of Patients (continued) (continued) Initial Phase* Continuation Phase† Total‡ Initial Phase* Continuation Phase† Total‡ Rifapentine Rifampin Rifapentine Rifampin Rifapentine Rifampin Rifapentine Rifampin Rifapentine Rifampin Rifapentine Rifampin System Organ System Organ Combina- Combina- Combina- Combina- Combina- Combina- Combina- Combina- Combina- Combina- Combina- Combina- Class Class tion tion tion tion tion tion tion tion tion tion tion tion Preferred Preferred (N=361) (N=361) (N=304) (N=317) (N=361) (N=361) (N=361) (N=361) (N=304) (N=317) (N=361) (N=361) Term Term N(%) N(%) N(%) N(%) N(%) N(%) N(%) N(%) N(%) N(%) N(%) N(%) INFECTIOUS DISEASE HEPATIC & BODY AS A WHOLE - NEUROLOGIC PSYCHIATRIC MUSCULOSKE- LETAL DERMATOLO- CARDIOVASC- OPHTHALMO-
Note: ≥1% refers to rifapentine in the TOTAL column.
*Initial Phase consisted of therapy with either rifapentine or rifampin combined with isoniazid,
pyrazinamide, and ethambutol administered daily (rifapentine twice weekly) for 60 days.
†Continuation Phase consisted of therapy with either rifapentine or rifampin combined with isoniazid
for 120 days. Rifapentine patients were dosed once weekly; rifampin patients were dosed twice
RESPIRATORY
‡A patient may have experienced the same adverse reaction more than once during the course of the
study, therefore, patient counts across the columns may not equal the patient counts in the TOTAL
In addition to the adverse reactions reported in Table 1, adverse reactions were reported post-treatment
during the 3 month through 24 month follow-up period. Although the protocol for this study specifiedcollection of serious adverse reactions during this period, some non-serious adverse reactions were
reported as well. For the rifapentine combination group these included the following: hematuria,infection tuberculosis, proteinuria, urinary casts, hyperkalemia, hypoglycemia, injury accident, skin
disorder, respiratory disorder, stupor, prostatic disorder.
Treatment-emergent adverse reactions reported during treatment and post-treatment through the firstthree months of follow-up in <1% of the rifapentine combination therapy patients are presented below
by body system in order of frequency. GASTROINTES- Renal & Urinary: urethral disorder, dysuria, pyelonephritis, urinary incontinence, urination disorder. Metabolic & Nutritional: weight decrease, BUN increased, diabetes mellitus, alkaline phosphatase increased, hypophosphatemia, hypercalcemia, hypovolemia, weight increase. Hematologic: lymphocytosis, hematoma, purpura, anemia hypochromic, anemia normocytic, throm- bosis. Body as a Whole - General: laboratory test abnormal, edema legs, asthenia, edema face, abscess,
edema peripheral, malaise. Dermatologic: skin ulceraction, urticaria, dry skin, furunculosis, skin discoloration, dermatitis fungal,
nail disorder, alopecia, rash erythematous. Respiratory: abnormal breath sounds, pneumothorax, pneumonia, pleural effusion, rhinitis, dyspnea, pneumonitis, sinusitis, sputum increased, pulmonary fibrosis, upper respiratory congestion, asthma, chest x-ray abnormal, bronchospasm, laryngeal edema, laryngitis, respiratory disorder. Gastrointestinal: tooth disorder, gastroenteritis, gastritis, esophagitis, cheilitis, dry mouth, pancreatitis, Table 2. Drug Interactions with PRIFTIN: Dosage Adjustment may be Necessary
proctitis, salivary gland enlargement, tenesmus, gastrointestinal disorder not specified. (continued) Infectious Disease: infection fungal, infection parasitic, infection protozoan. Hepatic & Biliary: bilirubinemia, hepatomegaly, jaundice. Drug Class Examples of Drugs Within Class Neurologic: somnolence, seizure not specified, dysphonia, hypoesthesia, torticollis, hypertonia,
hyporeflexia, meningitis, migraine headache, stupor. Psychiatric: anxiety, confusion, drug abuse, aggressive reaction, agitation. Musculoskeletal: myalgia, myositis, bone fracture, muscle weakness, muscle spasm. Cardiovascular: syncope, tachycardia, palpitation, hypotension orthostatic, pericarditis. Reproductive Disorders: penis disorder, vaginitis, vaginal hemorrhage, cervical smear test positive,
Sulfonylureas (e.g., glyburide, glipizide)
leukorrhea, mastitis male, prostatic disorder. Hearing & Vestibular: ear disorder not specified, otitis media, earache, otitis externa, tympanic
membrane perforation. Ophthalmologic: eye pain, eye abnormality. Neoplasms: pulmonary carcinoma, neoplasm not specified, carcinoma, lipoma. Vascular (Extracardiac): thrombophlebitis deep, vascular disorder, vasodilation. Special Senses Other: taste loss. Pregnancy, puerperium and perinatal conditions: abortion
In another randomized, open-label trial in 1075 HIV seronegative and seropositive patients withpulmonary tuberculosis the overall adverse event rate did not differ substantially from the previous trial.
Patients who had completed an initial 2 month phase of treatment with 4 drugs were randomly assignedto receive either rifapentine 600 mg and isoniazid once weekly or rifampin and isoniazid twice weekly
for the 4 month continuation phase. In the rifapentine arm, 502 HIV seronegative and 36 HIV seropositive patients were randomized and
Other Interactions
in the rifampin arm 502 HIV seronegative and 35 HIV seropositive patients were randomized to
The conversion of rifapentine to 25-desacetyl rifapentine is mediated by an esterase enzyme. There
is minimal potential for rifapentine metabolism to be inhibited or induced by another drug, or for
The death rate among all study participants was 71/1075 (6.6%) and did not differ between the two
rifapentine to inhibit the metabolism of another drug based upon the characteristics of the esterase
treatment groups (6.5% for the rifapentine combination regimen compared to 6.7% for the rifampin
Rifapentine does not induce its own metabolism [see Clinical Pharmacology (12.3)].
There were 526 treatment-emergent adverse events regardless of causality reported from 251 patientstreated with the rifapentine combination regimen and 513 adverse events reported from 248 patients
Since rifapentine is highly bound to albumin, drug displacement interactions may also occur [see
treated with the rifampin combination regimen. On both study arms the most frequently reported
adverse events were hyperglycemia, pneumonia, liver toxicity, and death and were consistent with
Interactions with Laboratory Tests
concurrent underlying conditions that included alcohol abuse, pancreatitis and HIV.
Therapeutic concentrations of rifampin have been shown to inhibit standard microbiological assays for
There was a greater percentage of patients in the rifampin combination arm who developed hepatic
serum folate and Vitamin B . Similar drug-laboratory interactions should be considered for rifapentine;
adverse events (35/513; 6.8 %) compared to 20/526 (3.8%) in the rifapentine combination arm. The
thus, alternative assay methods should be considered.
types of other adverse events were similar between the treatment arms. USE IN SPECIFIC POPULATIONS
Hyperuricemia was not reported as an adverse reaction in this study of continuation phase therapy. Pregnancy
In the previous study which evaluated initial therapy containing pyrazinamide, hyperuricemia was
Pregnancy Category C: There are no adequate and well controlled studies of rifapentine use during
reported in 32% of rifapentine and 23% of rifampin combination treated patients (see Table 1).
pregnancy. In animal reproduction and developmental toxicity studies, rifapentine produced fetal harm
DRUG INTERACTIONS
and was teratogenic. However, because animal studies are not always predictive of human response,
Protease Inhibitors and Reverse Transcriptase Inhibitors
rifapentine should be used during pregnancy only if the potential benefit justifies the potential risk to
Rifapentine is an inducer of CYP450 enzymes. Concomitant use of PRIFTIN with other drugs
metabolized by these enzymes, such as protease inhibitors and reverse transcriptase inhibitors, maycause a significant decrease in plasma concentrations and loss of therapeutic effect of the protease
When administered during the last few weeks of pregnancy, rifampin, another rifamycin, may increase
inhibitor or reverse transcriptase inhibitor. [see Warnings and Precautions (5.2) and Clinical Pharma-
the risk for maternal postpartum hemorrhage and bleeding in the exposed infant. Therefore, pregnant
women and their infants, who are exposed to rifapentine during the last few weeks of pregnancy, should
Hormonal Contraceptives
have appropriate monitoring of clotting parameters. Treatment with Vitamin K may be indicated.
PRIFTIN may reduce the effectiveness of hormonal contraceptives. Therefore, patients using oral,
Six patients randomized to rifapentine became pregnant during a study of initial treatment of
transdermal patch, or other systemic hormonal contraceptives should be advised to change to
tuberculosis. Two delivered normal infants; two had first trimester spontaneous abortions; one had an
non-hormonal methods of birth control.
elective abortion; and one patient was lost to follow-up. The two patients who spontaneously aborted
Cytochrome P450 3A4 and 2C8/9
had co-morbid conditions: One patient abused ethanol and the other patient was HIV positive.
Rifapentine is an inducer of cytochromes P4503A4 and P4502C8/9. Therefore, rifapentine may
Animal studies in rats and rabbits revealed embryofetal toxicity in both species. Pregnant rats given
increase the metabolism of other coadministered drugs that are metabolized by these enzymes.
rifapentine during organogenesis at doses 0.6 times the human dose (based on body surface area),
Induction of enzyme activities by rifapentine occurred within 4 days after the first dose. Enzyme
produced pups with cleft palates, right aortic arch, increased incidence of delayed ossification, and
activities returned to baseline levels 14 days after discontinuing rifapentine. In addition, the magnitude
increased numbers of ribs. When rifapentine was administered to mated female rats late in gestation,
of enzyme induction by rifapentine was dose and dosing frequency dependent; less enzyme induction
at 0.3 times the human dose (based on body surface area), pup weights and gestational survival (live
occurred when 600 mg oral doses of rifapentine were given once every 72 hours versus daily.
pups born/pups born) were reduced compared to controls. Increased resorptions and post implantation
In vitro and in vivo enzyme induction studies have suggested rifapentine induction potential may be
loss, decreased mean fetal weights, increased numbers of stillborn pups, and slightly increased pup
less than rifampin but more potent than rifabutin.
mortality during lactation were also noted. When pregnant rabbits received rifapentine at doses 0.3 to
Rifampin has been reported to accelerate the metabolism and may reduce the activity of the following
1.3 times the human dose (based on body surface area), major fetal malformations occurred including:
drugs; hence, rifapentine may also increase the metabolism and decrease the activity of these drugs.
ovarian agenesis, pes varus, arhinia, microphthalmia and irregularities of the ossified facial tissues. At
Dosage adjustments of the drugs in Table 2 or of other drugs metabolized by cytochrome P4503A4
the higher dose, there were increases in post-implantation loss and the incidence of stillborn pups.
or P4502C8/9 may be necessary if they are given concurrently with rifapentine. Nursing Mothers
It is not known whether rifapentine is excreted into human milk. Because many drugs are excreted in
Table 2. Drug Interactions with PRIFTIN: Dosage Adjustment may be Necessary
human milk and because of the potential for serious adverse reactions in nursing infants, a decisionshould be made whether to discontinue nursing or discontinue the drug, taking into account the
Drug Class Examples of Drugs Within Class
importance of the drug to the mother and the benefits of breastfeeding. Since rifapentine may produce
Disopyramide, mexiletine, quinidine, tocainide
a red-orange discoloration of body fluids, there is a potential for discoloration of breast milk. A slight increase in rat pup mortality was observed during lactation when dams were dosed late in
Chloramphenicol, clarithromycin, dapsone,
Pediatric Use
The safety and effectiveness of rifapentine in pediatric patients under the age of 12 have not been
established. In a pharmacokinetic study conducted in 2 to 12 year-old pediatric patients, the exposureto rifapentine (i.e., AUC and C
) was lower compared with that observed in healthy adults [seeClinical Pharmacology (12.3)]. Another pharmacokinetic study was conducted in 12 to 15 year-oldhealthy volunteers and the pharmacokinetics of rifapentine were similar to those observed in healthy
adults [see Clinical Pharmacology (12.3)].Geriatric Use
The Clinical studies of PRIFTIN did not include sufficient numbers of subjects aged 65 and over to
determine whether they respond differently from younger subjects. Other reported clinical experiencehas not identified differences in responses between the elderly and younger patients. In general, dose
selection for an elderly patient should be cautious, usually starting at the low end of the dosing range,
reflecting the greater frequency of decreased hepatic, renal, or cardiac function and of concomitantdisease or other drug therapy [see Clinical Pharmacology (12.3)].OVERDOSAGE
There is no experience with the treatment of acute overdose with rifapentine at doses exceeding 1200mg per dose.
In a pharmacokinetic study involving healthy volunteers (n=9), single oral doses up to 1200 mg have
Metabolism/Excretion
been administered without serious adverse events. The only adverse events reported with the 1200
Following a single 600 mg oral dose of radiolabeled rifapentine to healthy volunteers (n=4), 87% of the
mg dose were heartburn (3/8), headache (2/8) and increased urinary frequency (1/8). In clinical trials,
total 14C rifapentine was recovered in the urine (17%) and feces (70%). Greater than 80% of the total
tuberculosis patients ranging in age from 20 to 74 years accidentally received continuous daily doses
14C rifapentine dose was excreted from the body within 7 days. Rifapentine was hydrolyzed by an
of rifapentine 600 mg. Some patients received continuous daily dosing for up to 20 days without
esterase enzyme to form a microbiologically active 25-desacetyl rifapentine. Rifapentine and 25-
evidence of serious adverse effects. One patient experienced a transient elevation in SGPT and
desacetyl rifapentine accounted for 99% of the total radioactivity in plasma. Plasma AUC(0–∞) and
glucose (the latter attributed to pre-existing diabetes); a second patient experienced slight pruritus.
values of the 25-desacetyl rifapentine metabolite were one-half and one-third those of the
While there is no experience with the treatment of acute overdose with rifapentine, clinical experience
rifapentine, respectively. Based upon relative in vitro activities and AUC(0–∞) values, rifapentine and
with rifamycins suggests that gastric lavage to evacuate gastric contents (within a few hours of
25-desacetyl rifapentine potentially contributes 62% and 38% to the clinical activities against M.
overdose), followed by instillation of an activated charcoal slurry into the stomach, may help adsorb
any remaining drug from the gastrointestinal tract. Special Populations
Rifapentine and 25-desacetyl rifapentine are 97.7% and 93.2% plasma protein bound, respectively. Gender: In a population pharmacokinetics analysis of sparse blood samples obtained from 351
Rifapentine and related compounds excreted in urine account for only 17% of the administered dose,
tuberculosis patients who received 600 mg rifapentine in combination with isoniazid, pyrazinamide and
therefore, neither hemodialysis nor forced diuresis is expected to enhance the systemic elimination of
ethambutol, the estimated apparent oral clearance of rifapentine for males and females was 2.51 ± 0.14
unchanged rifapentine from the body of a patient with PRIFTIN overdose.
L/h and 1.69 ± 0.41 L/h, respectively. The clinical significance of the difference in the estimated
DESCRIPTION
apparent oral clearance is not known.
PRIFTIN (rifapentine) for oral administration contains 150 mg of the active ingredient rifapentine per
Elderly: Following oral administration of a single 600 mg dose of rifapentine to elderly (≥65 years) male
healthy volunteers (n=14), the pharmacokinetics of rifapentine and 25-desacetyl metabolite were similar
The 150 mg tablets also contain, as inactive ingredients: calcium stearate, disodium EDTA, FD&C Blue
to that observed for young (18 to 45 years) healthy male volunteers (n=20).
No. 2 aluminum lake, hydroxypropyl cellulose, hypromellose USP, microcrystalline cellulose, polyeth-
Pediatric (Adolescents): In a pharmacokinetic study in pediatric patients (age 2 to 12 years), a single
ylene glycol, pregelatinized starch, propylene glycol, sodium ascorbate, sodium lauryl sulfate, sodium
oral dose of 150 mg rifapentine was administered to those weighing <30 kg (n=11) and a single oral
starch glycolate, synthetic red iron oxide, and titanium dioxide.
dose of 300 mg was administered to those weighing >30 kg (n=12). The mean estimates of AUC and
Rifapentine is a rifamycin derivative antibiotic and has a similar profile of microbiological activity to
were approximately 30% to 50% lower in these pediatric patients than those observed in healthy
rifampin (rifampicin). The molecular weight is 877.04.
adults administered single oral doses of 600 mg and 900 mg.
In another pharmacokinetics study of rifapentine in healthy adolescents (age 12 to 15 years), 600 mg
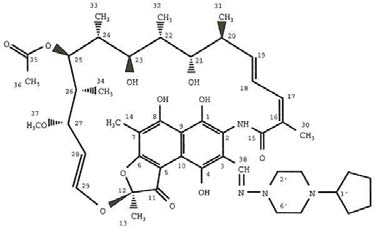
The chemical name for rifapentine is rifamycin, 3-[[(4-cyclopentyl-1-piperazinyl)imino]methyl]- or
rifapentine was administered to those weighing ≥45 kg (n=10) and 450 mg was administered to those
3-[N-(4-Cyclopentyl-1-piperazinyl)formimidoyl] rifamycin or 5,6,9,17,19,21-hexahydroxy-23-methoxy-
weighing <45 kg (n=2). The pharmacokinetics of rifapentine were similar to those observed in healthy
2,4,12,16,18,20,22-heptamethyl-8-[N-(4-cyclopentyl-l-piperazinyl)-formimidoyl]-2,7-(epoxypentadeca
[1,11,13]trienimino)naphtho[2,1-b]furan-1,11(2H)-dione 21-acetate. It has the following structure:
Renal Impaired Patients: The pharmacokinetics of rifapentine have not been evaluated in renal impaired patients. Although only about 17% of an administered dose is excreted via the kidneys, the clinical significance of impaired renal function on the disposition of rifapentine and its 25-desacetyl metabolite is not known. Hepatic Impaired Patients: Following oral administration of a single 600 mg dose of rifapentine to mild to severe hepatic impaired patients (n=15), the pharmacokinetics of rifapentine and 25-desacetyl metabolite were similar in patients with various degrees of hepatic impairment and to that observed in another study for healthy volunteers (n=12). Since the elimination of these agents are primarily via the liver, the clinical significance of impaired hepatic function on the disposition of rifapentine and its 25-desacetyl metabolite is not known. Asymptomatic HIV-Infected Volunteers: Following oral administration of a single 600 mg dose of rifapentine to asymptomatic HIV-infected volunteers (n=15) under fasting conditions, mean C
AUC(0–∞) of rifapentine were lower (20–32%) than that observed in other studies in healthy volunteers
(n=55). In a cross-study comparison, mean C
and AUC values of the 25-desacetyl metabolite of
rifapentine, when compared to healthy volunteers were higher (6–21%) in one study (n=20), but lower(15–16%) in a different study (n=40). The clinical significance of this observation is not known. Food
CLINICAL PHARMACOLOGY
(850 total calories: 33 g protein, 55 g fat, and 58 g carbohydrate) increases the mean AUC and Cmax
12.1 Mechanism of Action
of rifapentine observed under fasting conditions in asymptomatic HIV-infected volunteers by about 51%and 53%, respectively.
Rifapentine, a cyclopentyl rifamycin, is an antimycobacterial agent [see Clinical Pharmacology,Microbiology (12.4)]. Drug-Drug Interactions: Rifapentine is an inducer of cytochrome P4503A4 and 2C8/9. Therefore, it 12.3 Pharmacokinetics
may increase the metabolism and decrease the activity of other co-administered drugs that aremetabolized by these enzymes. Dosage adjustments of the co-administered drugs may be necessary
Absorption
if they are given concurrently with rifapentine [see Drug Interactions (7.3)].
The absolute bioavailability of rifapentine has not been determined. The relative bioavailability (with an
Indinavir: In a study in which 600 mg rifapentine was administered twice weekly for 14 days followed
oral solution as a reference) of rifapentine after a single 600 mg dose to healthy adult volunteers was
by rifapentine twice weekly plus 800 mg indinavir 3 times a day for an additional 14 days, indinavir C
70%. The maximum concentrations were achieved from 5 to 6 hours after administration of the 600
decreased by 55% while AUC reduced by 70%. Clearance of indinavir increased by 3-fold in the
presence of rifapentine while half-life did not change. But when indinavir was administered for 14 days
The administration of rifapentine with a high fat meal (850 total calories: 33 g protein, 55 g fat and 58
followed by coadministration with rifapentine for an additional 14 days, indinavir did not affect the
g carbohydrate) increased AUC(0–∞) and C
by 43% and 44%, respectively over that observed when
pharmacokinetics of rifapentine [see Warnings and Precautions (5.2) and Drug Interactions (7.1)].
administered under fasting conditions. 12.4 Microbiology
When oral doses of rifapentine were administered once daily or once every 72 hours to healthy
Mechanism of Action
volunteers for 10 days, single dose AUC(0–∞) value of rifapentine was similar to its steady-state AUCss
Rifapentine, a cyclopentyl rifamycin, inhibits DNA-dependent RNA polymerase in susceptible strains of
(0–72h) values, suggesting no significant auto-induction effect on steady-state
Mycobacterium tuberculosis but not in mammalian cells. At therapeutic levels, rifapentine exhibits
pharmacokinetics of rifapentine. Steady-state conditions were achieved by day 10 following daily
bactericidal activity against both intracellular and extracellular M. tuberculosis organisms. Both
administration of rifapentine 600 mg.
rifapentine and the 25-desacetyl metabolite accumulate in human monocyte-derived macrophages with
The pharmacokinetic parameters of rifapentine and 25-desacetyl rifapentine (active metabolite) on day
intracellular/extracellular ratios of approximately 24:1 and 7:1, respectively.
10 following oral administration of 600 mg rifapentine every 72 hours to healthy volunteers are
In Vitro Activity
Rifapentine and its 25-desacetyl metabolite have demonstrated in vitro activity against rifamycin-
Table 3. Pharmacokinetics and rifapentine and 25-desacetyl rifapentine in healthy
susceptible strains of Mycobacterium tuberculosis including cidal activity against phagocytized M.volunteers. tuberculosis organisms grown in activated human macrophages. The correlation between rifapentine MICs and clinical cure has not been established. Interpretive
Parameter Rifapentine 25-desacetyl Rifapentine
criteria/breakpoints to determine whether clinical isolates of M. tuberculosis are susceptible or resistantto rifapentine have not been established. Mean ± SD (n=12) In Vivo Activity
In mouse infection studies a therapeutic effect, in terms of enhanced survival time or reduction of organ
bioburden, has been observed in M. tuberculosis-infected animals treated with various intermittent
rifapentine containing regimens. Animal studies have shown that the activity of rifapentine is influencedby dose and frequency of administration. Drug Resistance
In the treatment of tuberculosis, a small number of resistant cells present within large populations of
susceptible cells can rapidly become predominant. Rifapentine resistance development in M. tuber-culosis strains is principally due to one of several single point mutations that occur in the rpoB portionof the gene coding for the beta subunit of the DNA-dependent RNA polymerase. The incidence of
Distribution
rifapentine resistant mutants in an otherwise susceptible population of M. tuberculosis strains is
In a population pharmacokinetic analysis in 351 tuberculosis patients who received 600 mg rifapentine
approximately one in 107 to 108 bacilli.
in combination with isoniazid, pyrazinamide and ethambutol, the estimated apparent volume of
Cross Resistance
distribution was 70.2 ± 9.1 L. In healthy volunteers, rifapentine and 25-desacetyl rifapentine were 97.7%
M. tuberculosis organisms resistant to other rifamycins are likely to be resistant to rifapentine. A high
and 93.2% bound to plasma proteins, respectively. Rifapentine was mainly bound to albumin. Similar
level of cross-resistance between rifampin and rifapentine has been demonstrated with M. tuberculosis
extent of protein binding was observed in healthy volunteers, asymptomatic HIV-infected subjects and
strains. Cross-resistance does not appear between rifapentine and non-rifamycin antimycobacterial
NONCLINICAL TOXICOLOGY
treatment. Enrollment of HIV seropositive patients was stopped when 4 of 36 patients in the rifapentine
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
combination group developed rifampin monoresistance. Fertility, Carcinogenesis, Mutagenesis
Table 5 below contains assessments of sputum conversion at the end of treatment (6 months total: 2
Hepatocellular carcinomas were increased in male NMRI mice (Harlan Winklemann) which were treated
months of initial and 4 months of randomized continuation treatment) and relapse rates at the end of
orally with rifapentine for two years at or above doses of 5 mg/kg/day (equivalent to a human dose
follow-up (24 months) in all HIV seronegative patients randomized to treatment. The failure and relapse
of 0.4 mg/kg/day or 1/5 th of the recommended human dose, in the intensive phase, based on body
rates reported in this study could be underestimated due to the limitation of the microbiologic methods
surface area conversions). In a two year rat study, there was an increase in nasal cavity adenomas
used in the study. Positive culture was based on either one sputum sample with >10 colonies on solid
in Wistar rats treated orally with rifapentine at 40 mg/kg/day (equivalent to a human dose of 6.5
media OR at least 2 positive sputum samples on liquid or solid media. However, only one sputum
mg/kg/day or 3 times the recommended human dose in the intensive phase, based on body surface
sample was collected at each visit in a majority of patients.
area conversions). Rifapentine was negative in the following genotoxicity tests: in vitro gene mutation assay in bacteria
Table 5: Clinical Outcome in HIV Negative Patients with Pulmonary Tuberculosis
(Ames test); in vitro point mutation test in Aspergillus nidulans; in vitro gene conversion assay in
Rifapentine Combination Rifampin Combination Saccharomyces cerevisiae; host-mediated (mouse) gene conversion assay with SaccharomycesTreatment % (n/N) Treatment % (n/N) cerevisiae; in vitro Chinese hamster ovary cell/hypoxanthineguanine-phosphoribosyl transferase (CHO/
Status at End of 4 Months Continuation Phase
HGPRT) forward mutation assay; in vitro chromosomal aberration assay utilizing rat lymphocytes; and
in vivo mouse bone marrow micronucleus assay. The 25-desacetyl metabolite of rifapentine was positive in the in vitro mammalian chromosome
aberration test in V79 Chinese Hamster cells, but was negative in the in vitro gene mutation assay in
bacteria (Ames test), the in vitro Chinese hamster ovary cell/hypoxanthine-guanine-phosphoribosyl
transferase (CHO/HGPRT) forward mutation assay, and the in vivo mouse bone marrow micronucleus
assay. Fertility and reproductive performance were not affected by oral administration of rifapentine to
male and female rats at doses of up to one-third of the human dose (based on body surface areaconversions). CLINICAL STUDIES
Rifapentine was studied in two randomized, open-label controlled clinical trials.
The first trial was an open-label, prospective, parallel group, active controlled trial in patients with
*Treatment response was defined as subjects who responded successfully after 16 doses of rifampin
pulmonary tuberculosis, excluding those with HIV-infection. The population was mostly comprised of
and isoniazid or after 8 doses of rifapentine and isoniazid, and remained sputum negative through the
Black (> 60%) or Multiracial (>31%) patients. Treatment groups were comparable for age and sex and
consisted primarily of male subjects with a mean age of 37 ± 11 years. In the initial 2 month phase
†Due to drug toxic effects, non-adherence, withdrawal of consent, receipt of nonstudy regimen, other.
of treatment (60 days), 361 patients received rifapentine 600 mg twice a week in combination with dailyisoniazid, pyrazinamide, and ethambutol and 361 subjects received rifampin 600 mg in combinationwith isoniazid, pyrazinamide and ethambutol all administered daily. The doses of the companion drugs
Higher relapse rates in HIV seronegative patients were seen in patients with a positive sputum culture
were the same in both treatment arms during the initial phase: isoniazid 300 mg, pyrazinamide 2000
at 2 months (i.e., at the time of study randomization), cavitation on chest x-ray, and bilateral pulmonary
mg, and ethambutol 1200 mg. For patients weighing less than 50 kg, the doses of rifampin (450 mg),
pyrazinamide (1500 mg) and ethambutol (800 mg) were reduced. Ethambutol was discontinued when
Seventy-one HIV seropositive patients were enrolled into the study. There were no treatment failures
isoniazid and rifampin susceptibility testing results were confirmed. During the 4 month continuation
during the study phase therapy. Sixty-one patients completed therapy and were assessed for relapse.
phase, 321 patients in the rifapentine group continued to receive rifapentine 600 mg dosed once weekly
The rates of relapse were 16.7% (5/30) in the rifapentine group and 9.7% (3/31) in the rifampin group.
with isoniazid 300 mg and 307 patients in the rifampin arm received twice weekly rifampin and isoniazid
Risk factors that predisposed to relapse in the HIV seropositive patients included the presence of both
900 mg. For patients weighing less than 50 kg, the doses of rifampin (450 mg) and isoniazid (600 mg)
pulmonary and extrapulmonary disease at baseline, low CD4 counts, use of azole antifungals and
were reduced. Both treatment groups received pyridoxine (Vitamin B6) over the 6 month treatment
period. Treatment was directly observed. Despite observed therapy, 65/361 (18%) of patients in the
In HIV seropositive patients, 4 of the 5 relapses from the rifapentine combination group involved M.
rifapentine arm and 34/361 (9%) in the rifampin arm received overdoses of one or more of the
tuberculosis strains with rifampin monoresistance (RMR). No relapse strain in the twice weekly
administered study medications during the initial or continuation phase of treatment. Only seven of
rifampin/isoniazid group had acquired drug resistance. These data are consistent with other docu-
these patients had adverse reactions reported with the overdose (5 in the rifapentine group and 2 in
mented acquired rifampin monoresistance in HIV seropositive adults who fail or relapse after treatment
with intermittent regimens with isoniazid and other rifamycins (rifampin and rifabutin).
Table 4 below contains assessments of sputum conversion at end of treatment (6 months) and relapse
The death rate among all study participants did not differ between the two treatment groups.
rates at the end of follow-up (24 months). References
1. Clinical and Laboratory Standards Institute. M24-A Susceptibility Testing of Mycobacteria,
Table 4. Clinical Outcome in HIV Negative Patients with Pulmonary Tuberculosis
Nocardiae, and Other Aerobic Actinomycetes; Approved Standard. 23 ed. 2003. Clinical Labo-ratory Standards Institute, Wayne, PA
Rifapentine Combination Rifampin Combination HOW SUPPLIED/STORAGE AND HANDLING Treatment % and (n/N*) Treatment % and (n/N*) How Supplied
PRIFTIN is supplied as 150 mg round normal convex dark-pink film-coated tablets debossed ″Priftin″
on top and ″150″ on the bottom, packaged in aluminum formable foil blister strips placed in cartons
of 32 tablets (4 strips of 8). Each strip of 8 tablets is inserted into an aluminum foil laminated pouch.
(NDC 0088-2100-03). Storage
Store at 25°C (77°F); excursions permitted 15–30°C (59–86°F) (see USP Controlled Room Tempera-
ture). Protect from excessive heat and humidity. PATIENT COUNSELING INFORMATION 17.1 Compliance Compliance with the full course of therapy must be emphasized to the patient, and the importance of
*All data for patients with confirmed susceptible M. tuberculosis (rifapentine combination treatment,
not missing any doses of the daily administered companion medications in the Initial Phase must be
N=286; rifampin combination treatment, N=283).
†Twenty-two (22) deaths occurred during the study; 11 in each treatment arm
17.2 Drug Interactions Rifapentine may increase the metabolism and decrease the activity of other drugs that are metabolized
Risk of relapse was greater in the group treated with the rifapentine combination. Higher relapse rates
by the P4503A4 and 2C8/9 pathways. Dosage adjustments of the co-administered drugs may be
were associated with a lower rate of compliance with the companion antituberculosis drugs as well as
necessary. Patients should be advised to discuss with their physician the other medications they are
a failure to convert sputum cultures at the end of the initial 2 month treatment phase. Relapse rates
taking before starting treatment with rifapentine.
were also higher for males in both regimens. Relapse in the rifapentine group was not associated with
Concomitant use of rifapentine with protease inhibitors or reverse transcriptase inhibitors may cause
development of mono-resistance to rifampin.
a significant decrease in plasma concentrations and loss of therapeutic effect of the protease inhibitor
In vitro susceptibility testing was conducted against M. tuberculosis isolates recovered from 620
patients enrolled in the study. Rifapentine and rifampin MIC values were determined employing the
Rifapentine may reduce the effectiveness of hormonal contraceptives. Therefore, patients using oral,
radiometric susceptibility testing method utilizing 7H12 broth at pH 6.8 (CLSI procedure M24-A; (1)).
transdermal patch, or other systemic hormonal contraceptives should be advised to change to
Six hundred and twelve patients had M. tuberculosis isolates that were susceptible to rifampin (MIC
non-hormonal methods of birth control.
< 0.5 µg/ml). Of these patients, six hundred and ten had M. tuberculosis isolates (99.7%) with
17.3 Discoloration of Body Fluids
rifapentine MICs of < 0.125 µg/ml. The other two patients that had rifampin susceptible M. tuberculosis
The patient should be informed that PRIFTIN may produce a reddish coloration of the urine, sweat,
isolates had rifapentine MICs of 0.25 µg/ml. The remaining eight patients had M. tuberculosis isolates
sputum, tears, and breast milk and the patient should be forewarned that contact lenses or dentures
that were resistant to rifampin (MIC > 8.0 µg/ml). These M. tuberculosis isolates had rifapentine MICs
of > 8.0 µg/ml. In this study high rifampin and rifapentine MICs were associated with multi-drug resistant
17.4 Adverse Reactions M. tuberculosis (MDRTB) isolates. Rifampin monoresistance was not observed in either treatment arm.
Patients should be instructed to notify their physician promptly if they experience any of the following:
This information is provided for comparative purposes only as rifapentine breakpoints have not been
fever, loss of appetite, malaise, nausea and vomiting, darkened urine, yellowish discoloration of the skin
and eyes, and pain or swelling of the joints.
The second trial was a randomized, open-label trial in 1075 HIV seronegative and seropositive patients
17.5 Administration with Food
with pulmonary tuberculosis. Patients with culture-positive, drug-susceptible pulmonary tuberculosis
For those patients with a propensity to experience nausea, vomiting, or gastrointestinal upset, inform
who had completed the initial 2 month phase of treatment with 4 drugs (rifampin, isoniazid,
those patients that administration of PRIFTIN with food may be useful.
pyrazinamide, and either ethambutol or streptomycin) under direct observation were randomly assigned
to receive either rifapentine 600 mg and isoniazid 15 mg/kg (max 900 mg) once weekly or rifampin 10
mg/kg (max 600 mg) and isoniazid 15 mg/kg (max 900 mg) twice weekly for the 4 month continuation
phase. Study drugs were given under direct observation therapy in both arms.
In the rifapentine arm, 502 HIV seronegative and 36 HIV seropositive patients were randomized andin the rifampin arm 502 HIV seronegative and 35 HIV seropositive patients were randomized to
False-positive urine drug screens: What clinicians should know and when the laboratory should be consulted Stacy E. F. Melanson, MD, PhD, FCAP Barbarajean Magnani, MD, PhD, FCAP College of American Pathologists Toxicology Resource Committee Urine drug screens (UDS) are frequently ordered on patients who exhibit symptoms of intoxication, experience trauma or offer a history of drug ingest
Este medicamento está sujeto a seguimiento adicional, lo que agilizará la detección de nueva información sobre su seguridad. Se invita a los profesionales sanitarios a notificar las sospechas de reacciones adversas. Ver la sección 4.8, en la que se incluye información sobre cómo notificarlas. 1. NOMBRE DEL MEDICAMENTO Lyxumia 20 microgramos solución inyectable 2. CO
 In a pharmacokinetic study involving healthy volunteers (n=9), single oral doses up to 1200 mg have
Metabolism/Excretion
In a pharmacokinetic study involving healthy volunteers (n=9), single oral doses up to 1200 mg have
Metabolism/Excretion