Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
Sastm.org.za
Healthcare challenges from the developing world: post-immigration refugee medicine Kristina M Adams, Lorin D Gardiner, Nassim Assefi
Worldwide, there are approximately 13 million
refugees and asylum seekers.1 Flight of refugees often
Summary points
occurs in the setting of war, famine, or human rights
violations, resulting from a “well-founded fear of being
The complex medical needs of refugees are often
persecuted for reasons of race, religion, nationality,
unmet owing to inadequate training of healthcare
membership in a particular social group, or political
opinion.”2 Physicians in host countries increasingly
encounter refugees in their practices and, owing to
Medical problems include infectious diseases,
inadequate training, may not fully meet their complex
psychiatric disorders, and complications from
HarborviewMedical Center,School of Medicine,
Sources and selection criteria
Symptoms of infectious diseases and history of
exposure to trauma and ritual female genital
Limited evidence exists to support many aspects of
surgery should be sought in the medical history
refugee health care. When scientific evidence is not
available, recommendations stem from our experience
Routine laboratory screening for infectious
in caring for a diverse group of refugees (East African,
diseases may detect parasites, sexually transmitted
Balkan, and South East Asian) in a multidisciplinary
setting involving primary care physicians, obstetrician-
gynaecologists, psychiatrists, nurses, cultural interpret-
Further information on post-traumatic stress
ers, and social workers. This article is based on clinical
disorder, somatisation, and ritual female genital
expertise and a review of the literature obtained from a
surgery may enable physicians to care better for
Medline search using the key words “refugee” and
“asylum seekers.” We suggest an approach to obtaining
the refugee history, screening for infectious diseases
and common psychiatric disorders, and dealing with
mal), and testing for syphilis and HIV. Enhanced health
special problems such as ritual female genital surgery
assessments may also be done to identify prevalent dis-
eases that may serve as future public health targets
before immigration. For example, frequent diagnoses
Refugee camps and medical
of malarial (7%) and intestinal (38%) parasites in
Barawan Somali refugees led the Centers for Disease
interventions before embarkation
Control to recommend mass treatment for all
Refugee camps represent the first point of escape, but
non-pregnant refugees older than 2 years; this
continued interethnic strife, sexual violence, and
consisted of single oral doses of sulfadoxine-
disease epidemics often perpetuate the dangerous
pyrimethamine and albendazole before departure.3
environment from which people fled. Although theUnited Nations High Commission for Refugees prom-
Medical history and physical
ises protection and basic medical care, refugees may
examination
actually have higher mortality in camps than in theirhome country. Major causes of mortality in refugee
Interpreter services are essential for obtaining the
camps include diarrhoeal diseases, measles, acute
medical history and caring effectively for refugees. The
respiratory tract infections, tuberculosis, and malaria.
lack of translators, particularly for new or small groups
Mandated medical screening of refugees before arrival
of refugees, is an important barrier to health care. Ide-
in the United States identifies those with “inadmissible
ally, the interpreter not only translates but also acts as a
conditions,” including active infections such as
mediator to explain the cultural context of a patient’s
tuberculosis, leprosy, and HIV infection. Typical
symptoms. On first meeting the refugee, we clarify the
screening of adult refugees involves a physical
purpose of a routine visit to a physician, the role of the
examination, brief mental health assessment, chest
interpreter, and the concept of preventive screening.
radiograph (sputum testing for tuberculosis if abnor-
Eliciting sensitive information, such as exposure to
BMJ VOLUME 328 26 JUNE 2004
from the Harvard trauma questionnaire (box 1).6 Manytranslations of the questionnaire exist to facilitate
Box 1: Medical history*
taking the trauma history. Questions about depressive
Life story
symptoms may need modification for each refugee
group, and medical interpreters are helpful in this
• Country of origin and reason for escape
regard. For example, one direct translation of “depres-
• Life and employment before immigration
sion” into Somali is “wal-wal,” which also means “crazy.”
• Medical problems or stress in home country
A complete physical examination may reveal
pathological and non-pathological conditions, includ-
• Time spent in refugee camps, location of the
ing lymphadenopathy, goitre, and evidence of previous
traditional medicine techniques. African and South
East Asian refugees often have circular scars consistent
• Losses of family members or friends and reasons
with dermabrasion from coining or moxibustion. Signs
of torture may be subtle and include occult fractures
Infectious diseases
from beatings or 1-2 mm clustered scars from electrical
• History of disease or exposure: tuberculosis, malaria,
parasites, hepatitis, and sexually transmitted infections• Review of systems:
• Recurrent fevers, night sweats, weight loss
Routine screening
Guidelines for screening of refugees are mainly based
• Diarrhoea, visible parasites in stool
on studies documenting a high prevalence of
infectious diseases and medical disorders.8 9 Obtaining
• Vaccine status: previous records and history of
records from overseas refugee screening may prevent
repetitive testing. We begin with a complete blood
Traditional medicine and substance misuse
count with differential and infectious disease screening
(box 2). Common causes of anaemia among refugeesinclude deficiencies of iron and other nutritional
• Acupuncture, moxibustion, coining, other modalities
• Use of substances other than tobacco and alcohol
and glucose-6-phosphate dehydrogenase deficiency. Sexual history and genital surgery
Eosinophilia warrants investigation for pathogenic
parasites, even in mild cases. In a group of South East
• Gravidity, parity, outcome of previous childbirths
Asian refugees with eosinophilia and negative stool
• Sexual activity, desire for testing for sexually
ova and parasite testing, a parasite was eventually
transmitted infections, contraception or pregnancy
Screening for infectious diseases includes testing
• Ability to have intercourse, dyspareunia
for tuberculosis, intestinal parasites, hepatitis, and
• Chronic urinary tract infections, pelvic pain, scar
sexually transmitted infections. Whether to give
empirical treatment or to screen for parasites remains
• Desire for revision of circumcision (defibulation)
controversial. Estimates of cost effectiveness are based
Trauma history†
on a five day course of albendazole, whereas many
• Deprivation of food, water, or shelter• Being lost, kidnapped, or imprisoned• Enforced isolation• Undergoing torture or serious injury
Box 2: Screening*
• Complete blood count with differential
• Rubella IgG (women of reproductive age)
• Syphilis, gonorrhoea, chlamydia, and HIV-1
*Contents of the box are based on clinical expertise as
guided by limited scientific evidence†Components of the trauma history are adapted from
• Stool ova and parasite examination (three morning
specimens, different days)• Oral examination and dental referral• Vision and hearing screen
trauma, may begin by asking the patient’s “life story”
Optional
and focusing sequentially on life in the home country,
reason for flight, details of escape, and status of family
members (box 1).4 5 We also do a complete review of
• Urinalysis (if concern about schistosomiasis)
infectious diseases by body system and inquire about
• Peripheral blood smear (if concern about malaria)
use of traditional or herbal medicines. We ask African
• PPD = purified protein derivative as used with
women about ritual female genital surgery, as it can
have important implications for gynaecological health.
*Screening items are in addition to recommended tests
After rapport and trust have been established, we
for healthcare maintenance (pap smear, mammogram,
directly inquire about torture, rape, or other physical or
psychological trauma by using an approach adapted
BMJ VOLUME 328 26 JUNE 2004
(Trichuris trichiura), roundworm (Ascaris lumbricoides),and Giardia lamblia.9 Classic complications of parasi-taemia
obstruction (roundworm), Loeffler’s syndrome (pul-monary hypersensitivity or infiltrates due to Strong-yloides and Ascaris), cholangiocarcinoma (Opisthorchissinensis), and bladder cancer (Schistosomiasis hemato-bium). A screening urinalysis for urinary schistosomia-sis is indicated in refugees from areas of highprevalence such as West Africa. Malaria is uncommonin refugees, as most are empirically treated; however,untreated pregnant refugees are at risk.
Hepatitis B is endemic in Africa and South East
Asia, with rates of current or past infection as high as50-80%. Death from cirrhosis or hepatoma occurs inup to one third of carriers who acquired hepatitis Bperinatally. We screen for hepatitis C in any patientwho has had a previous blood transfusion, ritualfemale genital surgery, or surgical procedure, and weroutinely screen African and South East Asianrefugees (prevalence of 5% and 2.5%).16
Mental health and trauma
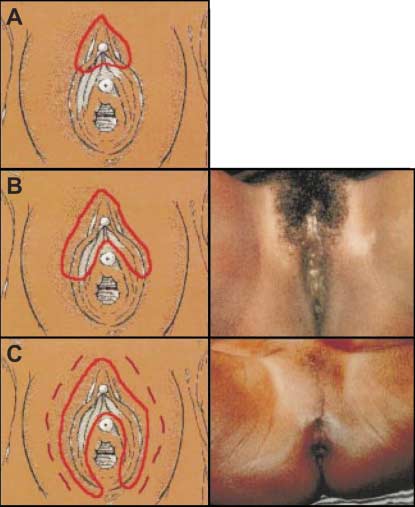
World Health Organization classification for ritual female genital
Tackling the complex mental health needs of refugees
surgery. A (type I or Sunna): excision of the prepuce with or without
is particularly challenging for both primary care
excision of the clitoris. B (type II): excision of the prepuce andclitoris and partial or total excision of the labia minora. C (type III or
providers and mental health professionals. Many stud-
pharaonic): excision of part or all of the external genitalia and
ies report refugees to be at a higher risk of psychiatric
stitching or narrowing of the vaginal opening. Type IV circumcision
disorders such as depression, suicide, psychosis,
(not pictured) describes procedures that do not fit the previous
post-traumatic stress disorder, and substance misuse,
classifications: piercing, cauterisation, or stretching of the clitoris orlabia with the aim of narrowing the vagina. Reproduced courtesy of
often directly related to past physical or psychological
Nahid Toubia, president of the RAINBO organisation
trauma.17–20 Understanding a patient’s trauma history iscritical to treating psychiatric and medical disorders.
centres administer a single dose.11 Depending on the
Approximately 5-10% of refugees in the United States
history of sexual activity, testing should include screen-
have experienced a form of torture, including electric
ing for gonorrhoea, chlamydia, syphilis, and HIV-1
shocks, beatings, caning of the soles of the feet, rape,
(and HIV-2 for West African refugees). In lieu of vacci-
and forced witnessing of torture or executions.21 Sexual
nation records, testing for antibodies to indicate expo-
violence is prominent in the torture of women and
sure to or vaccination against disease should be done.
may be spontaneous or systematic (“rape camps”). The
Antibody testing is more cost effective than varicella
problems of many refugees, however, may not be
vaccination in refugees older than 5 years.12 However,
adequately described by Western psychiatric catego-
the positive predictive value of a varicella history is
ries.22 Demoralisation and bereavement may be
93-100% and may be adequate for documentation in
incorrectly labelled as depression. An effort should be
certain refugee groups. Additional components of
made to simultaneously explore psychiatric symptoms,
screening include an oral examination, dental referral,
exposure to trauma, and potential social and economic
and screening of vision and hearing.
factors contributing to a refugee’s mental health. Referral to social workers, cultural case mediators, and
Tuberculosis, parasites, and hepatitis
community organisations may be appropriate.
Tuberculosis is the third leading cause of mortality
Post-traumatic stress disorder
from infectious diseases after HIV/AIDS and diar-rhoeal diseases; for example, one in three people in
Post-traumatic stress disorder is the most common
Africa are infected.13 In one study, 7% of newly arrived
consequence of violence and describes at least one
refugees had active tuberculosis, and the risk of devel-
month of recurrent, painful re-experiencing of a trau-
oping tuberculosis remains high years after immigra-
matic event, emotional numbing or hyperarousal, and
tion.14 15 At the United States Center for International
avoidance of trauma related memories.23 Critical
Health, 23% of tuberculosis cases were extrapulmo-
factors in developing post-traumatic stress disorder
nary.8 For example, back pain (Pott’s disease) or
include severity, duration, and closeness of exposure to
menorrhagia (endometrial tuberculosis) may be the
the trauma. Although studies of drug treatment in
presenting symptoms of tuberculosis. Other extrapul-
refugees with post-traumatic stress disorder are rare,
monary sites include the prostate, parotid, chest wall,
selective serotonin reuptake inhibitors are considered
a good first line treatment.24 25 Earlier studies
Despite mass treatment before embarkation,
recommended an 8-12 week drug trial, but recent
persistent parasitaemia is relatively common. The most
studies have found symptomatic improvement as soon
common parasites detected include hookworm (Neca-
as 2-5 weeks. However, severely traumatised refugees
tor americanus and Ancylostoma duodenale), whipworm
may fail to respond to drugs alone. Both exposure
BMJ VOLUME 328 26 JUNE 2004
logical findings, and mental health, focusing care onfunctional improvement rather than cure. Additional educational resources Journal articles Ritual female genital surgery
Walker PF, Jaranson J. Refugee and immigrant healthcare. Med Clin North Am 1999;83:1103-20
Ritual female genital surgery, also known as female cir-
Burnett A, Peel M. Health needs of asylum seekers and
cumcision or genital mutilation, is mainly done in
Africa and affects 130 million women and girls world-
Burnett A, Peel M. Asylum seekers and refugees inBritain: the health of survivors of torture and
wide.32 Ritual female genital surgery continues to be
organised violence. BMJ 2001;322:606-9
done for complex cultural reasons, although con-demned by the World Health Organization because of
Websites
its serious health consequences. In 1990 the Centers
US Committee for Refugees (www.refugees.org)—Listsstatistics, news, and information pertinent to refugees,
for Disease Control estimated that 168 000 girls and
and lists international refugee assistance organisations
women in the United States were likely to have under-
EthnoMed (www.ethnomed.org)—Provides culture
gone ritual female genital surgery, and subsequent
specific information on health beliefs and healthcare
Somali immigration greatly increased this number.
barriers for multiple refugee and immigrant groups.
Although discrete WHO classifications of ritual female
Factsheets on hepatitis, breast cancer, and diabetes are
genital surgery exist, people doing the procedure are
informally trained, resulting in inexact surgical
Harvard Program in Refugee Trauma(hprt-cambridge.org)—Provides questionnaires and
outcomes (figure). Physicians in host countries may
checklists for assessment of mental health in several
encounter long term complications of ritual female
genital surgery, including dyspareunia, inability to have
questionnaire, Hopkins symptom checklist-25, and a
intercourse, chronic pelvic inflammatory disease,
recurrent urinary tract infection, and scar abscesses.
Research Action and Information Network for the
Gynaecology referral for defibulation (take down or
Bodily Integrity of Women (www.rainbo.org)—Aninternational non-governmental organisation working
revision of ritual female genital surgery) may be
to eliminate the practice of ritual female genital
indicated for pelvic examination or treatment of result-
surgery. The website provides information on
ing medical complications, or before labour and
obtaining technical manuals for healthcare providers
Conclusion
therapy and cognitive behaviour therapy have been
Providing culturally sensitive and competent health
found to be beneficial for post-traumatic stress
care to refugee populations can be as rewarding as it is
disorder in refugees.26 27 Treatment may begin with an
challenging and often has a major impact on the life of
adequate trial of a selective serotonin reuptake inhibi-
a new refugee. Primary care for refugees begins with
tor; if minimal response occurs, consultation with a
understanding reasons for flight and a group’s particu-
psychiatrist is indicated to determine if additional
lar exposure to infectious disease and psychological
drugs ( blocker), therapy, or both should be added.
trauma, which may focus medical history and
Psychologists specialising in the mental health of refu-
screening. Increased knowledge about the complex
gees may represent an additional source of expertise,
medical needs of refugees can help the primary care
particularly with a form of therapy. Lack of availability
physician to care more effectively for this special popu-
of psychiatric care appropriate to culture and language
lation. A society’s moral strength can be measured by
may, however, represent a barrier to effective
how it treats its most vulnerable citizens.
Contributors: KMA and NA made substantial contributions tothe intellectual content of the entire text of the manuscript and
Somatisation
took active roles in its drafting and revision. LDG’s contributionto the manuscript was limited to the content and drafting of sec-
Psychological trauma may present as somatic com-
tions related to the trauma history and psychiatric diseases.
plaints in refugees. A diagnosis of somatisation
KMA is the guarantor of the manuscript.
disorder requires symptoms of pain (at least four sites),
Funding: Supported in part by HD-01264 from the National
two gastrointestinal symptoms, one sexual symptom,
Institutes of Health. The funding source represents a career
and one pseudoneurological symptom.23 Physical
development award for KMA and had no influence on the con-tents of the manuscript. LDG’s contribution was independent of
complaints must begin before age 30, result in consid-
a funding source. NA is now working for a non-governmental
erable impairment, and lack a medical cause. Refugees
organisation in Afghanistan to improve women’s health. Her
may be at risk for somatisation because psychiatric dis-
contribution to the manuscript predated her current position,
ease is often not culturally accepted, and somatic rather
and this organisation had no influence on her contribution tothe manuscript.
than psychiatric complaints increased their previous
chances of accessing health care. In addition, painthresholds may be lower in this population as a result
U.S. Committee for Refugees. World refugee survey 2003. (Available from
of psychological distress and depression. Somatisation
occurs more commonly in unemployed and less
Convention relating to the status of refugees. New York:
educated refugees.29 30 Epstein suggests an approach
Miller JM, Boyd HA, Ostrowski SR, Cookson ST, Parise ME, Gonzaga PS,
for patients with unexplained somatic symptoms that
et al. Malaria, intestinal parasites, and schistosomiasis among BarawanSomali refugees resettling to the United States: a strategy to reduce mor-
includes acceptance of suffering, tolerance of uncer-
bidity and decrease the risk of imported infections. Am J Trop Med Hyg
tainty, and limitation of iatrogenic harm.31 The
Kinzie JD. Evaluation and psychotherapy of Indochinese refugee patients.
physician simultaneously considers symptoms, patho-
Am J Psychother 1981;35:251-61. BMJ VOLUME 328 26 JUNE 2004
Mollica RF. The trauma story: a phenomenological approach to the trau-
19 Gorst-Unsworth C. Adaptation after torture: some thoughts on the long-
matic life experiences of refugee survivors. Psychiatry 2001;64:60-3.
term effects of surviving a repressive regime. Med War 1992;8:164-8.
Mollica RF, Caspi-Yavin Y, Bollini P, Truong T, Tor S, Lavelle J. The Har-
20 World Health Organization. WHO/UNHCR mental health of refugees.
vard trauma questionnaire: validating a cross-cultural instrument for
measuring torture, trauma, and posttraumatic stress disorder in Indochi-
21 Pincock S. Exposing the horror of torture. Lancet 2003;362:1462-3.
nese refugees. J Nerv Ment Dis 1992;180:111-6.
22 Watters C. Emerging paradigms in the mental health care of refugees. Soc
Goldfeld AE, Mollica RF, Pesavento BH, Faraone SV. The physical and
psychological sequelae of torture: symptomatology and diagnosis. JAMA
23 Diagnostic and statistical manual of mental disorders, 4th ed. Washington,
DC: American Psychiatric Association, 1994.
Walker PF, Jaranson J. Refugee and immigrant health care. Med Clin North
24 Friedman M, Davidson J, Mellman T, Southwick S. Pharmacotherapy. In:
Foa E, Keane T, Friedman M, eds. Effective treatments for PTSD: practice
Stauffer WM, Kamat D, Walker PF. Screening of international
guidelines from the International Society for Traumatic Stress Studies. New
immigrants, refugees, and adoptees. Prim Care 2002;29:879-905.
10 Nutman TB, Ottesen EA, Ieng S, Samuels J, Kimball E, Lutkoski M, et al.
25 Smajkic A, Weine S, Djuric-Bijedic Z, Boskailo E, Lewis J, Pavkovic I. Ser-
Eosinophilia in Southeast Asian refugees: evaluation at a referral center.
traline, paroxetine, and venlafaxine in refugee posttraumatic stress disor-
J Infect Dis 1987;155:309-13.
der with depression symptoms. J Trauma Stress 2001;14:445-52.
11 Muennig P, Pallin D, Sell RL, Chan MS. The cost effectiveness of strategies
26 Otto MW, Hinton D, Korbly NB, Chea A, Ba P, Gershuny BS, et al. Treat-
for the treatment of intestinal parasites in immigrants. N Engl J Med
ment of pharmacotherapy-refractory posttraumatic stress disorder
among Cambodian refugees: a pilot study of combination treatment with
12 Figueira M, Christiansen D, Barnett ED. Cost-effectiveness of serotesting
cognitive-behavior therapy vs sertraline alone. Behav Res Ther
compared with universal immunization for varicella in refugee children
from six geographic regions. J Travel Med 2003;10:203-7.
27 Paunovic N, Ost LG. Cognitive-behavior therapy vs exposure therapy in
13 World Health Organization. The world health report 2004—changing
the treatment of PTSD in refugees. Behav Res Ther 2001;39:1183-97.
history. www.who.int/whr/2004/en (accessed 16 June 2004).
28 Redwood-Campbell L, Fowler N, Kaczorowski J, Molinaro E, Robinson S,
14 DeRiemer K, Chin DP, Schecter GF, Reingold AL. Tuberculosis among
Howard M, et al. How are new refugees doing in Canada? Comparison of
immigrants and refugees. Arch Intern Med 1998;158:753-60.
the health and settlement of the Kosovars and Czech Roma. Can J Public
15 Zuber PL, McKenna MT, Binkin NJ, Onorato IM, Castro KG. Long-term
risk of tuberculosis among foreign-born persons in the United States.
29 Lin EH, Carter WB, Kleinman AM. An exploration of somatization
among Asian refugees and immigrants in primary care. Am J Public
16 Debonne JM, Nicand E, Boutin JP, Carre D, Buisson Y. [Hepatitis C in
tropical areas.] Med Trop (Mars) 1999;59(4 pt 2):508-16. (In French.)
30 Westermeyer J, Bouafuely M, Neider J, Callies A. Somatization among
17 Kinzie JD, Boehnlein JK, Leung PK, Moore LJ, Riley C, Smith D. The
refugees: an epidemiologic study. Psychosomatics 1989;30:34-43.
prevalence of posttraumatic stress disorder and its clinical significance
31 Epstein R. Somatization reconsidered: incorporating the patient’s experi-
among Southeast Asian refugees. Am J Psychiatry 1990;147:913-7.
ence of illness. Arch Intern Med 1999;159:215-22.
18 Bhui K, Abdi A, Abdi M, Pereira S, Dualeh M, Robertson D, et al.
32 Toubia N. Caring for women with circumcision: a technical manual for provid-
Traumatic events, migration characteristics and psychiatric symptoms
ers. New York: Rainbo Publishers, 1999.
among Somali refugees—preliminary communication. Soc Psychiatry Psy-chiatr Epidemiol 2003;38:35-43. Lesson of the week Charles Bonnet syndrome—elderly people and visual hallucinations Anu Jacob, Sanjeev Prasad, Mike Boggild, Sanjeev Chandratre Not all elderly
When a patient presents with vivid visual hallucina-
His medical problems included chronic lymphatic
tions, a doctor probably considers common diagnoses
leukaemia, which had been in remission for the past
presenting with
such as delirium, dementia, psychoses, or a drug
five years. He was registered blind and had been diag-
related condition. Charles Bonnet syndrome, however,
nosed as having gross bilateral macular degeneration. hallucinations
is a condition characterised by visual hallucinations
He had never had hallucinations before. He also had
have dementia
alongside deteriorating vision, usually in elderly
chronic obstructive airways disease and essential
people.1 The correct diagnosis of this distressing but
hypertension. He had had no other neurological
not uncommon condition is of utmost importance,
illness and no mental health problems. He did not
considering the serious implications of the alternative
drink alcohol or smoke. He had been taking
oxprenolol for hypertension for the past 10 years. He
Case report
His cognitive examination was normal for his age,
after the loss of vision was taken into account. His
Neighbours brought an 87 year old white widower—
visual acuity in both eyes was 1/60 with loss of central
who lived alone in a flat—to the medical assessment
field. Fundi showed macular degeneration. The rest of
unit of a district general hospital. They were concerned
the neurological examination was normal.
that he was becoming demented. Apparently he had
Detailed investigations (including a full blood
reported seeing people and animals in his house—
count; glucose; electrolytes; and tests for renal hepatic
including bears and Highland cattle. He verified these
statements and said he had been seeing them for the
and thyroid function, vitamin B-12, and folate levels)
previous six weeks. He had also often seen swarms of
yielded normal results. Detailed psychiatric assess-
flies and blue fish darting across the room.
ment did not pinpoint a cause and suggested more
He knew that these visions were not real and they
detailed investigations for delirium. As a metabolic
didn’t bother him much, but he thought he might be
and infection screen was normal and he was otherwise
losing his mind. The visions lasted for minutes to
well oriented, delirium did not seem a likely diagnosis.
hours, and the cattle used to stare at him while quietly
Electroencephalography and magnetic resonance
munching away at the grass. The visions tended to
imaging showed no important abnormalities. No
occur more in the evenings before he switched on the
diagnosis was apparent even after a week of inpatient
tests and ward rounds. An early dementia seemed to
BMJ VOLUME 328 26 JUNE 2004
<< SHOULD HEALTHY PEOPLE TAKE STATINS TOO? Rosuvastatin appears to lower the risk of heart disease in healthy people. Even healthy people seem to benefit from taking statins.Science The results of a study examining whether a potent cholesterol-lowering drug decreases the risk of heart disease are out1. Rosuvastatin was given to 17,802 seemingly healthy people, and their chance o
STATUS OF MISSION AGREEMENT (SOMA) ON THE ESTABLISHMENT AND MANAGEMENT OF THE HDC ACEH MONITORING MISSION (HAMM) In accordance with the cessation of hostilities (COH) agreement, the Government of the Republic of Indonesia (hereinafter referred to as the GOI) and the Free Aceh Movement (hereinafter referred to as the GAM) have requested the Henry Dunant Centre for Humanitarian Dialogue
 (Trichuris trichiura), roundworm (Ascaris lumbricoides),and Giardia lamblia.9 Classic complications of parasi-taemia
obstruction (roundworm), Loeffler’s syndrome (pul-monary hypersensitivity or infiltrates due to Strong-yloides and Ascaris), cholangiocarcinoma (Opisthorchissinensis), and bladder cancer (Schistosomiasis hemato-bium). A screening urinalysis for urinary schistosomia-sis is indicated in refugees from areas of highprevalence such as West Africa. Malaria is uncommonin refugees, as most are empirically treated; however,untreated pregnant refugees are at risk.
(Trichuris trichiura), roundworm (Ascaris lumbricoides),and Giardia lamblia.9 Classic complications of parasi-taemia
obstruction (roundworm), Loeffler’s syndrome (pul-monary hypersensitivity or infiltrates due to Strong-yloides and Ascaris), cholangiocarcinoma (Opisthorchissinensis), and bladder cancer (Schistosomiasis hemato-bium). A screening urinalysis for urinary schistosomia-sis is indicated in refugees from areas of highprevalence such as West Africa. Malaria is uncommonin refugees, as most are empirically treated; however,untreated pregnant refugees are at risk.