Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
Doi:10.1016/j.dmr.2005.07.004
The Role of Public Health Nurses inBioterrorism PreparednessRalitsa B. Akins, MD, PhD, Josie R. Williams, MD, MMM, RN, Rasa Silenas, MD, FACS,and Janine C. Edwards, PhD
Background: Public health nurses have a central
Conclusions: The study’s findings could have
function in the public health system. Nurses
implications for public policy and nursing
conduct disease surveillance, which is an
leadership. Defining the structure of the public
important first step in recognizing diseases
health system and the scope of public health
caused by bioterrorist agents. Unfortunately, the
nurses’ responsibilities will serve as the
cornerstone for improvement of bioterrorism
expectations for public health nurses are not
clearly defined and therefore pose seriousdifficulties for conducting disease surveillance. Increased surveillance activities for bioterrorismpreparedness add more responsibilities to the
issue for public health systems across theUnited States.The US public health system
relies on primary health care providers to recognize
unusual cases or activity levels and notify officials of
surveillance was conducted with public health
their observations. In turn, local, state, and federal
officials at regional and local levels, working in
public health agencies have proscribed roles designed
a variety of urban and rural settings in one large
to help limit the spread of a potentially lethal or
public health region in Texas. Data analysis was
disabling agent. Central to this planning are public
supported by qualitative research software,
health nurses, who are expected to provide any
number of essential services. Planners often assumethat a system is adequately staffed to allow for new or
Results: The study found that the nurses workingat the local level were extremely dedicated toserving their communities, had formed informal
partnerships that are essential for diseasesurveillance, and effectively used informal
communication channels to obtain critical
surveillance information. The study revealed thatnurses had unmet needs and experienced
expanded roles. Unfortunately, insufficient numbers
of specific types of staff, or insufficient staff prepara-
tion, may impede the success of such plans. The
Ralitsa B. Akins is Associate Research Scientist at The Texas
Quality Program, Cooperative Agreement No. 1 U18
A&M University System, Health Science Center, Rural and
Community Health Institute, Quality and Patient Safety
Reprint requests: Ralitsa B. Akins, MD, PhD, The Texas
Initiatives, College Station, Texas. Josie R. Williams is
A&M University System Health Science Center, Rural
Director at the Rural and Community Health Institute,
and Community Health Institute, Quality and Patient
The Texas A&M University System Health Science Center,
Safety Initiatives, 301 Tarrow, 7th Floor, College Station,
College Station, Texas. Rasa Silenas is Medical Director at
TX 77840; E-mail: ralitsa_akins@yahoo.com.
The Texas A&M University System Health Science Center,Office of Homeland Security, College Station, Texas.
Disaster Manage Response 2005;3:98-105.
Janine C. Edwards is Research Professor at The Texas
A&M University System, Health Science Center, Rural
Copyright Ó 2005 by the Emergency Nurses Association.
and Community Health Institute, College Station, Texas.
This research was sponsored by the Agency forHealthcare Research and Quality, Partnerships for
98 Disaster Management & Response/Akins et al
Table 1. Study sites and characteristics of the study interviewees
Epidemiologist, Metropolitan Health District
Emergency Management Coordinator (retired)
Surveillance Director and Senior Staff Scientist
DSHS, Department of State Health Services.
human factor is a necessary and critical asset for health
The interviewed public health officials represented
services functioning and is often missing from national
local and regional public health levels and had diverse
backgrounds including nursing, medicine, epidemiol-
The human factor (eg, staff numbers, availability,
ogy, and emergency management. The characteristics
training, and networking) as it relates to professional
public health nursing demands further exploration. It
Settings. The interviews were conducted at 9 sites
is important to explore the role of public health nurses
within Texas Department of State Health Services
in bioterrorism preparedness and their readiness to
(DSHS) Region 8, which includes 1 large metropolitan
assume that role and to define their new responsi-
area, San Antonio, and 21 surrounding counties, the
bilities in bioterrorism preparedness and disease
majority of which are rural. Texas DSHS Region 8 has
a population of 2,146,154 people and is spread over32,429 square miles. DSHS 8 is larger (both inpopulation numbers and square miles) than the states
of West Virginia, Rhode Island, Delaware, Vermont, orNew Hampshire.The research sites included the
We report the results from a qualitative study on
headquarters of the Texas DSHS, San Antonio
disease surveillance that revealed the importance of
Metropolitan Health District (nationally recognized
monitoring the ability of public health nurses to
for its high bioterrorism preparedness), 5 rural
participate in bioterrorism preparedness and disease
counties with county-based public health departments
surveillance. This study was sponsored by the Agency
(2 of which were testing new surveillance systems),
for Healthcare Research and Quality and was ap-
1 military installation, and 2 border cities (1 in the
proved by the Institutional Review BoarddHuman
United States and 1 in Mexico) with a border crossing
Subjects in Research at Texas A&M University (pro-
A comprehensive set of questions about existing
Interviewees. The interview sample was selected
and emerging disease surveillance systems in the
to present a multifaceted picture of the current public
region was developed by 2 researchers in the study
health system and existing surveillance approaches.
team (RS and JCE). A pilot interview with the staff of
Disaster Management & Response/Akins et al 99
Table 2. Questionnaire for semi-structured inter
What kinds of disease surveillance are practiced in your community? (syndrome and disease reporting,
environmental monitoring, vector monitoring, electronic data mining, etc)
For each surveillance method, please describe who reports, who initiates the reporting, and what happens to
the information after it is reported.
How satisfied are you with each of the surveillance methods in terms of costs and limitations? (timeliness,
accuracy, sensitivity, specificity, personnel, space, infrastructure, etc)
What surveillance information do you receive and what do you do with it? Please describe the internal use and
external reporting of disease surveillance information.
How well does available surveillance information support the needs of senior officials in your community?
What would improve your ability to communicate risk to senior officials?
What method or capability for disease surveillance would you like to add? What kind of information would
What else would you like to say about disease surveillance? (free comments)
)Detailed questionnaire is available upon request.
a county public health office was conducted to test the
could affect a public health department’s ability to
validity of the questionnaire. The questions proved
prepare for bioterrorist events and to conduct disease
satisfactory, and one change to the interview pro-
cedure was made as a result of our experience in thepilot test. presents the major interviewquestions that were used in this study.
Lack of a Standard Education for PublicHealth Providers
Providers enter a public health career through
The study data were collected during the period
a variety of different venues and at several different
of March through August 2004 by our research
educational levels. This factor makes it difficult to
team. Using a qualitative research approach,semi-
quantify the public health workforce and standardize
structured interviews were conducted with 19 public
the position requirements, a process that is even more
health officials at 9 interview sites at regional and local
difficult for rural areas. Officials with graduate degrees
levels (see The interviews were 1½ to 3 hours
in public health were found only at the regional level;
no officials with public health academic degrees werefound at the local agency sample sites. Many nurses
and officials interviewed in this study had found their
The audiotapes were transcribed and entered into
way to public health service without formal education
research software (The Ethnograph, 5.08, distributed
by Qualis Research Associates) that is designed tofacilitate the analysis of qualitative data. Researchers
Many nurses and officials interviewed in this
coded all segments of the text and compiled themesby code. A code book and a code family tree were
study had found their way to public health
used to ensure consistency and objectivity in working
service without formal education or training in
with text segments across the interviews. The inter-views iterated a primary theme regarding the diverse
roles that public health nurses have in general and indisease surveillance in particular. This theme also was
The public health nurses came from a variety of
present across a variety of initially defined codes.
previous types of practice. Only a few had taken
In the process of data analysis, the thoughts of
courses in public health, and local public health
separate interviewees on different public health nurses’
nurses trained each other. Many nurses expressed
roles were reconstructed into a meaningful category by
frustration at the difficulty of finding additional
the processes of data reduction, combining same or
training or taking time to study when they did not
similar themes, and induction, identifying new mean-
have adequate coverage for their absence.
ingful ideas emerging from the gathered data.
Many of the local health departments in Texas
This study of the public health system in Texas
DSHS Region 8 consisted of one nurse and perhaps an
DSHS Region 8 demonstrated a number of themes that
administrative assistant. Two public health nurses
100 Disaster Management & Response/Akins et al
described being on call around the clock, year-round,even taking calls when on vacation, sometimes out ona boat in the middle of a lake. When one person ina department leaves, others may try to ‘‘keep the placefrom falling apart,’’ but often the traveler is the onlyone who is fully capable of some functions.
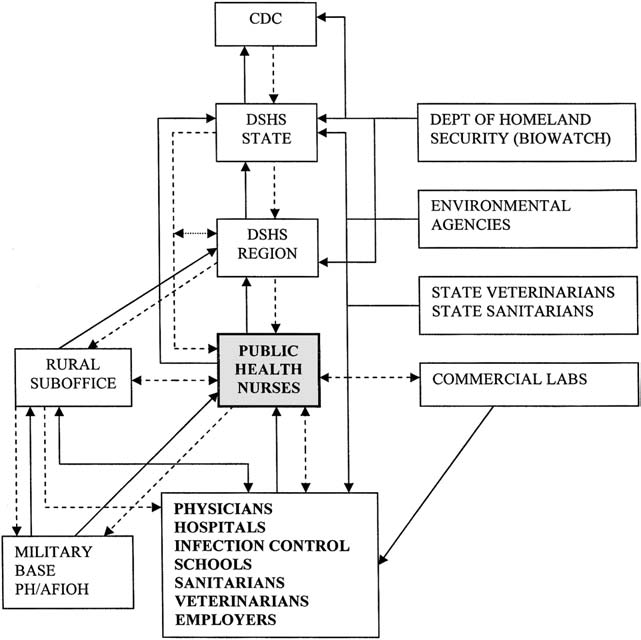
We found a well-established network of formal
reporting pathways, coupled with very importantinformal networks of information sharing and feed-back. shows the complicated informationflow from various reporters to the public healthagencies.
Our study showed that regular reporting of in-
fectious diseases at a county level was dependent onthe working relationships between the public healthnurse and all other reporters (eg, the doctors, infectioncontrol people at the hospital, clinics, laboratories,
Figure 1: Disease surveillance reporters to public health
school nurses, day care, and nursing homes). The
agencies. Straight lines indicate formal networks; dashed
public health nurses took the initiative, whether it was
lines indicate informal networks and partnerships.
weekly or only several times a year, to talk with thevarious reporters about the importance of what theyare doing and the need for timeliness. Feedback about
aggregated counts of cases from the public health
department to all of the reporters also assisted in
Funding for public health nurses has traditionally
maintaining the awareness of the necessity of timely
come through disease or service-specific programs (eg,
tuberculosis screening, family planning, or treating
All of the interviewees spontaneously expressed
sexually transmitted diseases). Unlike hospital-based
their belief that person-to-person working relation-
nurses who theoretically could change positions and
ships were the backbone of surveillance. In one
roles based on the general needs of the institution,
county, active surveillance began in 1998 when the
public health nurses’ primary responsibilities are
public health nurse became more aware of the
closely tied to particular funding programs, which
necessity for collecting information about communi-
often are mandated through legislation. It becomes
cable diseases in a timely manner. That nurse took the
extremely difficult for a public health nurse who is
initiative to call each of the possible reporters and
funded through a specific program to be proactive in
explain why they needed to make complete reports in
bioterrorism preparedness and disease surveillance in
a timely manner on infectious diseases. The nurse
addition to the primary program activities.
explained that it took some time to educate all of the
As one of our interviewees noted, ‘‘A lot of people
reporters, but they all soon began to appreciate the
have spent their entire public health careers watching
regular weekly phone calls. Furthermore, the report-
disease du jour funding. In fact, if you look across
ers began to fax or telephone a suspicious report
health departments in Texas, you can see evidence of
immediately on their own initiative, without waiting
this, because depending on when they established their
health department, those are the program dollars that
Another county public health nurse undertook
they get. So you’ve got programs created in the 60’s that
a very active campaign when she came into that
have. a vast majority of their State funding is
position to educate doctors, school and hospital
tuberculosis. It has nothing to do with the disease
nurses, and all other reporters. The nurse explained
patterns now of TB, but it has to do with when they
that with personal relationships and communications,
raised their hand and said, ‘‘We want to have a local
she was able to initiate more reporting and timelier
health department’’ and the money available in the 60’s
reports: ‘‘I made packets with the reporting guidelines
was TB money. So, they still have it. Health departments
from the State, and I went out and visited with every
that sprang up in the 70’s have immunization money,
physician and their office staff. I explained the
and in the 80’s, the health departments started getting
importance of and the legal need for, which they were
disproportionately funded with HIV and STD money.
not aware of really, that these were laws that required
And if you formed a health department right now, then
you’ve got people on a bioterrorism budget.’’
Disaster Management & Response/Akins et al 101
The Texas DSHS Region 8 Director noted that
although bioterrorism preparedness funds have been
Local public health nurses are expected to in-
available after September 11, 2001, few positions in
vestigate disease outbreaks, assess community health,
this region have been established with the grant
provide a variety of health community services,
money. This is because the bioterrorism grant funding
execute prevention programs, interpret and apply
was expected to go on for only several more years,
analytic tools and methodologies, and build commu-
and there was an obvious lack of a source to sustain
the funding over time. The unreliable sources of
Their duties include guiding the development of
funding made it difficult to open positions for public
bioterrorism response plans for their institutions and
health nurses that also were needed for other essential
communities, encompassing preventive measures,
public health services. ‘‘Theoretically you would think
infection control practices, postexposure manage-
that we could look at the time of a public health nurse,
ment, laboratory support, and public information
and we could say, 2 days a week she spends doing
bioterrorism, one day maternal and child health, one
In general, the public health workforce includes all
day TB, one day vaccine preventable diseases, and
people educated and employed in public health or
right there I’ve filled up a week in 20% increments.
related fields, and their professional skills can be
And you would think that we would be able to
broad and variable.In our study, the public health
attribute her salary in 20% increments to those 4
nurses came from a variety of backgrounds, including
different programs: bioterrorism, TB, family health
well-child nursing, psychiatric nursing, communicable
services, immunizations. But our accounting system
diseases, hospital nursing, and school nursing. If
can’t do that. It wants everybody, every full time
public health professionals were to be defined solely
on their education or certification, it would be almostimpossible to recruit enough nurses to fill the
positions, because of a lack of public health focus innursing curricula and a competition for nurses who
might be interested in other, more financially re-
2001, few positions in this region have been
warding fields.Nurses who assume public healthroles have multiple educational needs, including how
to connect with their community needs and publichealth priorities.
Although nurses are funded through a specific
In a case study conducted in rural local health
program, their scope of responsibilities can encom-
departments of Wyoming and Idaho, the lack of
pass both clinical and public health care in their local
formal public health training of the workforce was
communities. There is an explicit expectation by the
identified as a major problem in reaching the public
regional office that the nurses will know their
health service objectives.It was concluded that the
communities and local authorities and will need to
lack of scientific and medically relevant curriculum
establish relationships and networks. Public health
materials for public health and medical professionals
nurses were perceived to be the ‘‘bridge’’ connecting
is contributing to the knowledge gap in bioterrorism
clinical health care and public health at the local level.
This is an example of how a nurse’s practice can differ
The need for specialized bioterrorism training has
due to the constraints of programmatic funding.
led some agencies to create their own resources. TheUniversity of Connecticut utilizes a variety of ap-proaches to accommodate working public health
practitioners by offering evening programs, distancelearning, interdisciplinary approach, maximum utili-
In general, the US public health system structure
zation of local resources (such as the regional office of
has enormous variability across different states. Local
the Federal Bureau of Investigation), guest speakers,
public health offices comprise the safety network for
communities in case of natural disaster or terroristattack and nurses play a pivotal role in ensuring thefunction of the public health system.The scope and
extent of the services provided in each state depend
Traditionally, when a public health nurse is needed,
on infrastructure, workforce composition, educational
a recruitment announcement for a nurse is placed.
preparedness, and funding sources. The only com-
Persons with new clinical skills are put into the
monality found across state public health organiza-
community but are not necessarily public health–-
tions is the great demand for nurses to fill public
trained individuals. This practice leads to public health
nurses getting knowledge and skills from on-the-job
102 Disaster Management & Response/Akins et al
training. The general lack of available and accessible
The active outreach activities carried on by the nurses
education and training, the noncompetitiveness of
we interviewed display remarkable commitment and
public health position salaries, and the national nurse
problem–solving ability in the face of persistent
shortage are all problems for filling public health
personnel and resource shortages. We perceive that
positions with appropriately trained nurses. One study
these partnerships have improved the timeliness of
of the nursing workforce documented that an increase
communicable disease reporting during recent years.
in nursing wages affected nurses’ supply, causing the
Multiple communication systems required. Pub-
number of employed nurses to increase when wages
lic health nurses are expected to use complex commu-
increased.Thus, increased funding for public health
nication and information technology systems (including
nurses may increase the number of persons interested
work with E-mail, Internet, and the Public Health
Information Network) to support important functions
Interviewees indicated that they would be more
of surveillance, such as disease outbreak detection and
effective if they had additional public health nurse
monitoring, data analysis, knowledge management,
personnel. Employers may find it challenging to
develop uniform public health job requirements based
Although constrained by limited resources, the
on job title, functions, and organizational base.
public health nurses in this study found creative
Previous researcsuggests that many public health
ways to improve reporting and keep information
nurses, especially those in rural areas, are filling in for
flowing. The nurses created formal and informal
jobs and activities that would have been delegated to
networking (partnerships) to conduct disease surveil-
others if more staff were available in their public
lance. The complexity of information pathways
health departments. The inadequate number of
reflects the widely diverse sources and users of this
personnel available to perform day-to-day functions
information. The formal and informal pathways forinformation flow are equally important and publichealth nurses play a pivotal role in data gathering and
Because the personnel are stretched to the
The informal pathways supplement the formal ones
and ensure timely recognition of important problems.
the infrastructure for surge capacity for
These informal pathways are created by the partner-ships established by public health nurses, which are
catastrophic disasters is not developed.
characteristic of Region 8 surveillance. If only the for-mal pathways for information flow were used, part of
can easily lead to ‘‘burnout.’’ Because the personnel
the surveillance information would not be available.
are stretched to the breaking point with everyday
Informal networks were considered extremely
activities, the infrastructure for surge capacity for
important for successful functioning of local public
catastrophic disasters is not developed.
health departments. In one case of a school outbreakof Shigella infection, the public health nurses quickly
informed neighboring counties to be on the lookout
Active versus passive surveillance. The litera-
for a secondary spread. Although this happened
ture makes a distinction between active and passive
through an informal reporting chain, it served the
surveillance methodshowever, Region 8 county
practicality of the issue very well; the public health
public health nurses used both methods of collecting
nurses of surrounding counties were notified even
information. Active surveillance occurs when public
before the medical doctors went to the school.
health officials request surveillance reports from
Each organizational level of health departments in
health care providers on a regular basis. Passive
Region 8 has processes to relay information up and
surveillance refers to public health officials expecting
down the chain. The state health department operates
the providers/reporters to send the information to
a Health Alert Network of fax and E-mail notification
them unprompted. In our study, we found no useful
of important disease information to health depart-
distinction between active and passive surveillance
ments, public health nurses and practitioners. Most
because the nurses created good working relation-
local health departments also have means to relay
ships (partnerships) among the public health officials
local surveillance information to their reporters. All
and the various types of reporters, so that both types
public health officials believed that when an emerging
situation required a public response, they were able to
The partnerships developed with the providers/
get that response. They expressed confidence that
reporters in their communities by the public health
their elected officials trust them to provide appropriate
nurses in this study (see ) give evidence of
information and recommendations. A few interview-
fulfilling the ‘‘extensive individual initiative’’ required
ees mentioned the role of economic and political
in the county public health nurse position description.
influences on action, but most believed that a true
Disaster Management & Response/Akins et al 103
health emergency would receive appropriate atten-
responsibilities, will serve as a cornerstone for
tion, even if there were negative effects such as loss of
improvement and national alignment of bioterrorism
This case study is important because it clearly
identified the multifaceted roles of public health
nurses in bioterrorism preparedness and chartedsome of their needs and barriers to more proactive
This study is limited to information acquired from
surveillance. The role of the public health nursing
literature and document review, and the perceptions,
workforce merits clear definition and emphasis in the
experiences, and expertise of the study participants,
further development of the public health infrastructure
who are public health officials at local and regional
for bioterrorism preparedness. Focused attention from
levels in a large public health region in Texas
public health, political, and homeland security leaders
including both urban and rural settings.
for support in the development of the public healthworkforce is well deserved.
1. Fraser MR, Fisher VS. Elements of effective bioterrorism
Public health nurses are central to the public health
preparedness: a planning primer for local public health
system and to bioterrorism surveillance, which was
agencies. Washington: National Association of Countyand City Health Officials; 2001. Available from: URL:
evidenced by their ability to navigate through a system
that lacked clear boundaries, definitions, or expect-
ations for their performance. Coming from different
2. Moteff J, Parfomak P. Critical infrastructure and key
backgrounds, often without prior public health expe-
assets: definition and identification (2004 Oct 1). CRS
rience or training, the public health nurses managed
report for Congress. Available through The Library ofCongress, order code RL32631.
to carry a variety of responsibilities while continuing
3. Census 2000 [online, accessed 2005 Feb 3]. Available
their community service. The nurses emerged as a
fragily balanced, but critical and committed compo-
4. Emerson RM, Fretz RI, Shaw LL. Writing ethnographic
nent of the public health system, and disease
fieldnotes. Chicago: The University of Chicago Press;
surveillance, in particular. Our data suggest that the
5. Lincoln YS, Guba EG. Naturalistic inquiry. Newbury Park
nurses created informal partnerships to augment and
support the formal information flow pathways needed
6. Gebbie K, Merrill J, Tilson HH. The public health
workforce. Health Affairs 2002;21:57-67.
Our study showed that the fragmentation of the
7. Latter S, Speller V, Westwood S, Latchem S. Education for
public health system, the operational lines, expect-
public health capacity in the nursing workforce: findingsfrom a review of education and practice issues. Nurs
ations, and responsibilities for public health nurses are
quite confusing. The lack of clearly set theoretical and
8. Dembek Z, Iton A, Hancen H. A model curriculum for
public health bioterrorism education. Public Health Rep2005;120:11-8.
Public health nurses carry both public health
9. Richardson M, Casey S, Rosenblatt RA. Local health
districts and the public health workforce: a case study of
Wyoming and Idaho. J Public Health Manage Practice2001;7:37-48.
10. English JF, Cundiff MY, Malone JD, Pfeifer JA, Bell M,
Steele L, et al. Bioterrorism readiness plan: a template for
healthcare facilities [online; 1999 Apr 13; accessed 2005May 27]. Available from: URL:
service boundaries makes it difficult even for nurses
formally trained in public health to define public
11. Grant Makers in Health. Strengthening the public health
health responsibilities and expectations at national or
system for a healthier future (Issue Brief No.17, February2003) [online, accessed 2005 Feb 3]. Available from: URL:
local levels. Thus, the lack of a systems design and the
fragmented infrastructure become hindrances in the
12. Dumpe ML, Herman J, Young SW. Forecasting the
execution of public health priorities. Furthermore,
nursing workforce in a dynamic health care market. Nurs
public health nurses carry both public health and
community health functions, which, although over-
13. Hajat A, Stewart K, Hayes KL. The local public health
workforce in rural communities. J Public Health Manage
lapping, have different connotations. Defining the
structure of the public health system, as well as the
14. Dicker R. Principles of epidemiology. 2nd ed. (CDC
expectations for and the scope of public health nurses’
Self-Study Course 3030-G, 1992) [online, accessed 2005
104 Disaster Management & Response/Akins et al
based approach to connecting public health and clinical
medicine. In: Syndromic surveillance: reports from
15. Broome CV, Loonsk J. Public Health Information Net-
a national conference, 2003. Morbid Mortal Weekly Rep
work: improving early detection by using a standards-
Disaster Management & Response/Akins et al 105
FUSING & ATROPHY 1. HOW FUSING TAKES PLACE 2. FUSING VS. ATROPHY HOW FUSING TAKES PLACE Normally the mucous membranes are made to slide back and forth without sticking to one another, (such as in the mouth, even our internal organs) they have a 'slickness' to them, (a coating or covering,) without pulling on each other. Rub your tongue over the inside of your cheek and you'll
A healthy sexual relationship is one of life’s expectations and pleasures. When things go wrong, whether or not we have diabetes, many of us fi nd it hard to accept that there might be a problem that may need to be treated. It’s important to know this isn’t something you need to face alone as there is a great deal of available support. Does diabetes cause sexual problems?While most peo
 described being on call around the clock, year-round,even taking calls when on vacation, sometimes out ona boat in the middle of a lake. When one person ina department leaves, others may try to ‘‘keep the placefrom falling apart,’’ but often the traveler is the onlyone who is fully capable of some functions.
described being on call around the clock, year-round,even taking calls when on vacation, sometimes out ona boat in the middle of a lake. When one person ina department leaves, others may try to ‘‘keep the placefrom falling apart,’’ but often the traveler is the onlyone who is fully capable of some functions.