Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
Microsoft word - an intervention of diet.doc
An Intervention of Diet, Exercise, and Medication to Reduce the Prevalence of Cardiovascular Disease and Obesity among Hispanic Male Population in South Texas Border Cities
Rohitha Goonatilake† (harag@tamiu.edu), Vivian Garcia‡ (vivian@tamiu.edu), Irma A.
Lara‡ (ilara@tamiu.edu), and Rose A. Saldivar‡ (rsaldivar@tamiu.edu)
†Department of Mathematical and Physical Sciences, College of Arts and Sciences
‡Dr. F.M. Canseco School of Nursing, College of Nursing and Health Sciences
Texas A&M International University, Laredo, Texas 78041-1900
Abstract
Cardiovascular disease (CVD) is highly prevalent among Hispanics. Recently, there has been an increase in reported cases of CVD. Finding measures to deal with the prevention and treatment of these diseases are high on the agenda among healthcare providers, community leaders, and local and state legislatures. These issues are being considered by healthcare professionals and community leaders to bring the situation under control and for prevention of these diseases. The issues are investigated on the basis of the cause of the disease and the relationship among various factors unique to the population and the circumstances that are highly prevalent in the population. The prevalence of the metabolic syndrome is highest among Hispanic adults. Actos and other similar drugs are considered thiazolidinedione anti-diabetic agents that depend on the presence of insulin for their mechanism of action [11]. Actos also decreases insulin resistance in the periphery and in the liver resulting in increased insulin-dependent glucose disposal and decreased hepatic glucose output. Treatment methods of the disease using these medications will be discussed using a number of drugs available in the markets and impacts of them on various age groups consist of male patients. Keywords: Cardiovascular disease, Hispanics, diet, exercise, cholesterol, HDL, LDL Preliminaries
Among Hispanics or Latinos in the US, heart disease and stroke rank as the top causes of death. They claim the lives of 28.6% of the more than 122,000 Hispanics or Latinos who die each year as of 2003 final figures. Cancer follows, killing 19.7%. All other causes of death account for 51.7% [1]. Cardiovascular disease is not as noticeable or unsightly as obesity, costs a lot, and inflicts both whites and Hispanics, particularly men, but the rate for women and children is increasing. The Latino population is projected to reach approximately 103 million (24.4% of the US population) by 2050 [2] costing $163 billion annually to treat CVD related diseases and $118 billion to treat diabetes patients. For generations, concerns over CVD among Latino or Hispanic ethnic groups in the US were
± Funding for this project undertaking partially supported by Texas Center for Border Economic and Enterprise Development at Texas A&M International University, Laredo, Texas 78041-1900
unnoticed by a widespread perception that they were less vulnerable to CVD-related diseases than the rest of the population. Deaths from CVD and related diseases place a huge burden on our country’s economy as related healthcare costs are staggering along with costs to maintain families left behind. According to [17], the cause of death by ethnic group, diseases of the heart is ranked at the top for Hispanics, blacks, and American children. In 2003, it was estimated that 7.7% of Hispanics have heart disease, 4.5% have cardiovascular heart disease; 19% must deal with hypertension, which is associated with the development of heart disease and 2.2% have suffered stroke [1].
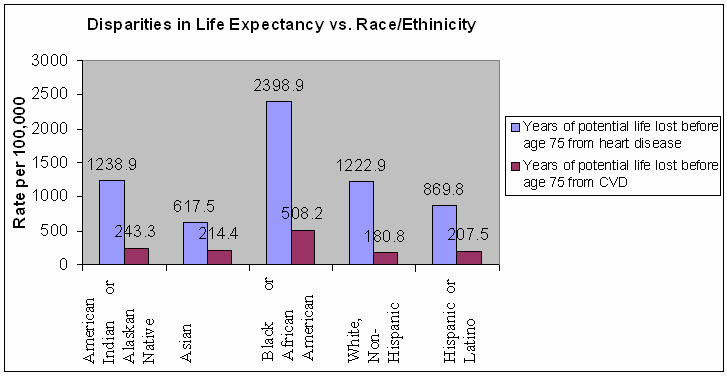
Figure 1: Disparities in Selected Health Indicators by Race/Ethnicity, US Date Source: http://www.cdc.gov/DHDSP/library/action_plan/pdfs/action_plan_3of7.pdf. Some ethnic groups reported a lower life expectancy due to heart disease and CVD as provided in Figure 1. The Hispanic/Latino ethnic group is one of the greatest affected ethnic groups. Rates calculated per 100,000 age-adjusted using the 2000 US standard population that includes all heart disease deaths coded according to the International Statistics Classification of Diseases and Related Health problems. The data from other already existing sources such as the US Census Bureau, the Centers for Disease Control (CDC), the National Institutes of Health (NIH), and the Interuniversity Consortium for Political and Social Research (ICPSR) has been a part of much of the descriptive statistics provided for preliminary work [5] and [10]. Data based on household interviews of a sample of the civilian non-institutionalized population summarizes in Table 1. Based on the responses, Hispanics or Latinos claimed to have the largest affected ethnic group in terms of a lower percentage of excellent health, a lower life expectancy or very good health having a larger variation due to heart disease and CVD. Table 1: Percentage of Excellent or Very Good Health vs. Ethnicities Race/Ethnicity Percent Confidence Interval
Date Source: National Health Interview Survey, January-June 2007 Figure 2 depicts this disparity among these ethnic groups in terms percentage of excellent or very good health.
Figure 2: An Illustration for Interval Estimation for Excellent or Very Good Health Based on National Health Interview Survey, January-June 2007 The purpose of this study can be many-fold. The first objective is to establish the prevalence of the metabolic syndrome and related disease factors in the South Texas region and of individual components contributing to overweight of Hispanic groups ages ranging from teenagers to older adults at risk for Type II diabetics [4]. Final summaries are presented using ATP III criterion and the World Heath Organization (WHO) criteria for diagnosis of metabolic syndrome [7], [8], and [9]. The results from this representative sample of US adults from South Texas border region at risk for Type II diabetics, for all age groups can shed some light on the situation that is highly prevalent and impact the fastest growing ethnic group. The large numbers of US residents with the metabolic syndrome may have important implications for the healthcare sector and the staggering costs in treatment and prevention. The healthcare professionals and border community leaders need to join hands to combat these diseases and bring the situation under control. There is an urgent need to take drastic measures for the Hispanic population and to identify the associated factors for socioeconomic research in order to assist governmental and other organizations to implement particularly, health-related social programs that combat the diseases. Research Methodology and Analysis
Visits have been made to two selected local treatment facilities in Laredo, Webb County, Texas, US on a regular basis to gather data (names are withheld for the purpose of confidentiality). These facilities provide treatment for patients diagnosed with diabetes and metabolic syndrome and related comorbidities. The patients are monitored during and after initiating treatments. One is a Primary Care Clinic and other is a Private Physician’s Medical Office.
The primary Care Clinic is administered by two physicians and two nurse practitioners. One physician and a nurse practitioner manage the Private Physician’s Medical Office. The patients who are at the Primary Care Clinic are mostly women. Both men and women are treated at the Private Physician’s Medical Office. A group of patients from one facility was included in the data set. The patients’ information is de-identified. It is noted that care is provided utilizing different treatment guidelines which may lead to the use of different medications and treatment options. Follow-up visits and care differs between the two facilities as have been noticed. The blood tests will normally consist of a Lipid Panel (T Chol, Trig, LDL, HDL). If the patient is diabetic or hypoglycemic, other tests will be determined by the healthcare provider. For the discussion of this paper, records of a group of 18 male patients were examined. They were categorized into age groups, 35 – 45, 45 – 55, 55 – 65, 65 – 75, 75 – 85, and 85 – 95 to determine the impact of these test indicators as results of administering drugs and treatments including diet and exercise. In addition, data from other already existing sources such as the US Census Bureau, the Centers for Disease the Control (CDC), the National Institutes of Health (NIH), and the Interuniversity Consortium for Political and Social Research (ICPSR) have been included in preliminary work of this study. Participants are selected by utilization of a convenience sample drawn from Laredo, Webb County, Texas, US. The male patients of Hispanic background ranging from mid thirties to older adults have been the targeted subjects at the physician’s office. A criterion for inclusion at the facility includes being on Actos or another antibiotic drug for treatment of metabolic syndrome or diabetes mellitus [6]. Data collection includes total cholesterol, high density lipoprotein (HDL), low density lipoprotein (LDL), triglycerides, fasting blood glucose prior to each visit and every three to six month scheduled visits to these facilities. Blood pressure [3], height, weight, and abdominal girth measurements (BMI) are taken on these appointments were extracted and tabulated for analysis. Benefit of Heritage and Typical of the Population
The better-than-expected health and mortality of Hispanics, given their lower socioeconomic status (SES), has been called the Hispanic paradox. Studies find that Hispanics have relatively lower mortality rates compared with Whites [13]. However, other studies provide evidence that Hispanics (Mexican-Americans) are not advantages in their measured biological risk profiles [12]. Mexican immigrants have been inspired by the literature on the "epidemiological paradox" - they appear healthier because they arrive from a culture with healthier food, more exercise and less smoking and drinking--this advantage disappears as they acculturate to American society. Hunt et al. criticize the use of English language usage and demographic proxy indicators for what is a complex cultural concept [14]. Lengths of time in the US of foreign-born and subsequent generations or English language usage ratings are poor measures for Americanization. This would involve a complex constellation of attitudes, values, and practices along with change overtime. Abraido-Lanza et al. found that Latinos are less likely to drink alcohol and smoke cigarettes, which would contribute to an explanation of the epidemiological paradox [15]. Smoking is related to cardiovascular disease and lung cancer, which is less evident in the
Latino population. Nevertheless, Latinos had a less favorable BMI (body mass index) and were less likely to exercise for the purpose of physical fitness- primarily due to female behavior, not male. These mixed findings were found while controlling for age and socio- economic status. BMI is related to the Latino diabetes rate but not to cardiovascular disease rate- a paradoxical finding. It is suggested that Latinos do engage in strenuous behavior at work and home rather than leisure exercise. Acculturation was associated with an increase in three unhealthy behaviors: (1) drinking alcohol, (2) smoking and (3) increased BMI (which implies a change in diet) and one healthy behavior--increased physical exercise at leisure. Abraido-Lanza et al. suggests that both men and women acculturate to American gender norms regarding drinking and smoking [15]. It is speculated that an unhealthy diet may be the basis of increased BMI among women. The traditional consumption of beans, rice, and vegetables in home countries is healthier than the typical US diet. This study found that acculturated women were more likely to exercise. This sample can be critiqued as practicing "ethnic lumping" of all Latino subgroupings when there may be inter-ethnic variation. Results and Findings
A determination is made to find the extent of effectiveness by different combination of drugs available in the market to reduce weight and BMI. For this group, combination of drugs has been used for treatment. The assumption that they equally assisted in treating the disease is needed in this determination. Contributions made by each patient are then aggregated for the entire sample in order to obtain Figures 3. Next, the impact on test indicators for various age groups from these drugs will be determined.
Drug Impact on Weight and BMI ion 10 duct e R s/ 5 Names of Drugs Figure 3: Drug Impact on the Loss of Weight and Reduction of BMI
There are many drugs currently on the market to treat these diseases. In particular, drugs such as 1-Actos, 2-Actos plus M, M-Metformin, J-Januvia, Jm-Janumet, Am-Glimepiride, Bi-Glyuburide, L-Lipitor, Lo-Lovasa, T-Tricor, Gl-Glipizide, V-Simvastin, Ad-Lovastin, C-Crestor, AdM-Avandamet, La-Lantus, Z-Zetia, Hu-Humalog are well known and in addition, introduction (+) and removal (-) of other drugs at various stages of the treatment plans are done by the healthcare provider to treat the prevalent symptoms and dependent on patient willingness to use and ability to obtain, if determined. As for the impact of drugs and combination of drugs for the study group, the survey was able to conclude that Actos, Actos plus Metformin, Lipitor, Glipizide, Glimepiride, Januvia, Metformin, and Lovastin have performed well in that order as in Figure 3. The drug types, Janumet and Glyuburide, equally helped to be the last candidates in the survey. Tricor assisted to reduce the BMI, while Avandamet assisted to reduce the weights only. The rest of the drugs showed a negative reaction when it comes to weight and BMI. It is safe to conclude that some drugs performed better than others but it is cautioned that it is necessary to conduct a survey of a larger group of males for longer period to make a final determination to decide the effectiveness of these drugs in this population and age groups. A form of hemoglobin termed as Glycosylated (or glycated) hemoglobin (hemoglobin A1c, Hb1c, or HbA1c) used primarily to identify the average plasma glucose concentration over prolonged periods of time. It is sometimes abbreviated to A1C. It is formed in a non-enzymatic pathway by hemoglobin's normal exposure to high plasma levels of glucose. High A1C has been implicated in nephropathy and retinopathy in diabetes mellitus. Monitoring the HbA1c diabetic patients may improve treatment options [16]. Reductions of this indicator and others for each patient are aggregated for the entire sample in order to obtain Figures 4-9.
AIC vs. Age Groups Age Groups Figure 4: Reaction of Glycosylated Hemoglobin (A1C) vs. Age Groups One of the primary objectives of this paper is to see the extent of effectiveness from various drugs in A1C test indicators. The test indicator A1C showed negative effects on
age groups, 35-45, 55-65, and 65-75 while other groups showed some effects as in Figure 4 during the period of observation.
FBP vs. Age Groups Age Groups Figure 5: Reaction of Fasting Blood Pressure (FBP) vs. Age Groups Fasting blood pressures (FBP) have shown no remarkable improvement for these groups as depicted in Figure 5 during the period of observation. HDL vs. Age Groups Age Groups Figure 6: Reaction of HDL vs. Age Groups The impact of HDL is higher for age group 55-65. At the same time, the age group 75-85 has received no positive impact during the period of observation according to Figure 6. LDL vs. Age Groups n 20 tio c 0 Age Groups Figure 7: Reaction of LDL vs. Age Groups From Figure 7, it can be stated that the test indicator for LDL reacted negatively for age groups 65-75 and 75-85 during the period of observation. T Chol vs. Age Groups n 40 tio c 20 Age Groups Figure 8: Reaction of T Cholesterol (T Chol) vs. Age Groups The test results showed T Chol is unfavorable for age groups, 65-75 and 75-85 from Figure 8 during the period of observation. Trig vs. Age Groups n io ct 100 Age Groups Figure 9: Reaction of Triglycerides (Trig) vs. Age Groups These drugs did not help much to improve triglycerides (Trig) for age groups, 45-55 and 85-95 during the period of observation as determined from Figure 9. Conclusions and Future Work
One of the primary objectives of this paper is to see the extent of effectiveness for various drugs in terms of each test indicators. The test indicator A1C was affected negatively in age groups, 35-45, 55-65, and 65-75 while for other groups showed some positive effects. Fasting blood pressures (FBP) have shown no remarkable improvement for these groups. The impact of HDL is higher for age group 55-65, the age group 75-85 has received no positive impact, and LDL reacted negatively for age groups 65-75 and 75-85. The test results showed T Chol is unfavorable for age groups, 65-75 and 75-85. These drugs did not help very much to improve triglycerides (Trig) for age groups, 45-55 and 85-95 during the period of observation. As for the impact of drugs and combination of drugs for the study group, the survey was able to conclude that Actos, Actos plus Metformin, Lipitor, Glipizide, Glimepiride, Januvia, Metformin, and Lovastin performed well in that order. The drug types, Janumet and Glyuburide equally helped to be the last candidates in the survey. A cholesterol drug, Tricor also assisted to reduce the BMI, while Avandamet to reduce the weights only. The rest of the drugs showed a negative reaction when it comes to weight and BMI. However, it is always necessary to conduct a survey for a larger group of males for consistent longer observation period needed to make a final determination to decide the effectiveness of these drugs in the patients and age groups considered in the study. Acknowledgements
Dr. Andrés Rivas Chavez, Director and Ms. Amy Palacios, Research Assistant of Texas Center Texas Center for Border Economic and Enterprise Development at Texas A&M International University, Laredo, Texas 78041 deserve our appreciation for awarding this
Texas Center Research Fellows Grant Program award for this project with funding. Ms. Rose A. Saldivar, assistant professor of nursing, Dr. F.M. Canseco School of Nursing, College of Nursing and Health Sciences, who gathered partial data needed for this research topic during Summer 2008, has assisted with the completion of this project, deserves our many thanks. The cooperation received from the physicians and staff at the two selected local treatment facilities in Laredo for gathering data has been tremendous. References
[1]. American Heart Association Committee on Statistics and Strokes Subcommittee, 2006. http://www.americanheart.org [2]. Fogel S and Martin J (March 2006). Four Immigration Scenarios, a Report by the Federation for American Immigration Reform Projecting the U.S. Population to 2050 [3]. Third Report of the National Cholesterol Education Program Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Executive Summary, Bethesda, MD, National Institutes of Health, National Heart, Lung and Blood Institute (NIH publication no. 01-3670), 2001 [4]. Alberti KG, Zimmet PZ (1998). Definition, Diagnosis and Classification of Diabetes Mellitus and its Complications. Part 1. Diagnosis and Classification of Diabetes Mellitus, Provisional Report of a WHO Consultation. Diabet Med 15, pp. 539–553, 1998 [5]. Polit DF (1996). Data Analysis and Statistics for Nursing Research, Appleton & Lange, Stamford, CT [6]. Metabolic Syndrome: The Costliest Condition You've Never Heard Of Afflicts Nearly One in Four Americans, Main Category: Diabetes News, Article Date: 09 May 2005, (UK), Medco Health Solutions, Inc. http://www.medco.com [7]. Dennison JA (May 2005). Metabolic Syndrome May Be the Next American Epidemic, Vol. 7, HEALTH NEWS [8]. Selig PM (2006). Metabolic Syndrome in the Acute Care Setting, AACN Clinical Issues, 17, 1, pp. 79-85 [9]. Foldout Feature: Getting Tough with Metabolic Syndrome, 2004, The McGraw-Hill Companies, New York, NY. http://www.postgradmed.com/issues/2004/01_04/metabolic_foldout.pdf [10]. Shannon DM and Davenport MA (2001). Using SPSS to Solve Statistical Problems: A Self-Instruction Guide, Prentice-Hall, Inc, Upper Saddle River, NJ [11]. Cruz ML, Weigensberg MJ, Huang TT-K, Ball G, Shaibi GQ, and Goran MI (2004). The Metabolic Syndrome in Overweight Hispanic Youth and the Role of Insulin Sensitivity, J Clin Endorcrinol Metab, January 89 (1), pp. 108-113 [12]. Crimmins EM, Kim JK, Alley DE, Karlamangla A, and Seeman T (2007). Hispanic Paradox in Biological Profiles, American Journal of Public Health, Research and Practices, Vol. 97, No. 7, pp. 1305-1310 [13]. Markides KS, Eschbach K, (2005). Aging migration, and mortality: current status of research on the Hispanic paradox, Journal of Gerontol B. Psychol. Sci Soc. Sci., Vol. 60, pp. 68-75 [14]. Hunt LM, Schneider S, and Comer B (2004). Should “acculturation” be a variable in health research? A critical review of research on US Hispanics, Social Science & Medicine 59, pp. 973-986
[15]. Abraído-Lanza AF, Chao MT, and Flórez KR (2005). Do healthy behaviors decline with greater acculturation? Implications for the Latino mortality paradox, Social Science & Medicine, Vol. 61, pp. 1243-1255 [16]. Fraser DJ and Phillips AO (2007). Diabetic nephropathy, Medicine, Vol. 35, Issue 9, pp. 503 – 506 [17]. Monthly vital statistics report; Vol. 43, No. 6 (s): NCHS, Advance report of final mortality statistics, 1992. Hyattsville, Maryland: US Department of Health and Human Services, Public Health Service, CDC, 1994 Profile of the Authors
Dr. Rohitha Goonatilake is an associate professor of mathematics in the Department Mathematical and Physical Sciences and the coauthor of similar projects with several of his colleagues. Ms. Vivian Garcia, Ms. Irma A. Lara, and Ms. Rose A. Saldivar serve as assistant professors of nursing in Dr. F.M. Canseco School of Nursing and are working on healthcare issues, primarily, prevention of diseases such as diabetes and Cardiovascular disease in the Laredo/Webb County, Texas.
Antimicrobial susceptibility of 51 Campylobacter strains isolated from diarrheic and diarrhea-free dogs. ANTIMICROBIAL SUSCEPTIBILITY OF 51 CAMPYLOBACTER STRAINSISOLATED FROM DIARRHEIC AND DIARRHEA-FREE DOGS* J.R. Modolo1, R. Giuffrida2, C.A. de M. Lopes3 1Faculdade de Medicina Veterinária e Zootecnia, UNESP/Botucatu, CP 524, CEP 18618-000, Botucatu, SP,The minimum inhibitory concentrat
Diagnosis of Fibromyalgia Syndrome—A Comparison ofAssociation of the Medical Scientific Societies in Germany,Survey, and American College of Rheumatology CriteriaWinfried Ha¨user, MD,*w Sebastian Hayo,* Werner Biewer, MD,z Mechthild Gesmann, MD,yHedi Ku¨hn-Becker, MD,J Frank Petzke, MD,z Hubertus von Wilmoswky, MD,#Objectives: The survey and the Association of the Medical ScientificAlth
 unnoticed by a widespread perception that they were less vulnerable to CVD-related diseases than the rest of the population. Deaths from CVD and related diseases place a huge burden on our country’s economy as related healthcare costs are staggering along with costs to maintain families left behind. According to [17], the cause of death by ethnic group, diseases of the heart is ranked at the top for Hispanics, blacks, and American children. In 2003, it was estimated that 7.7% of Hispanics have heart disease, 4.5% have cardiovascular heart disease; 19% must deal with hypertension, which is associated with the development of heart disease and 2.2% have suffered stroke [1].
Figure 1: Disparities in Selected Health Indicators by Race/Ethnicity, US
unnoticed by a widespread perception that they were less vulnerable to CVD-related diseases than the rest of the population. Deaths from CVD and related diseases place a huge burden on our country’s economy as related healthcare costs are staggering along with costs to maintain families left behind. According to [17], the cause of death by ethnic group, diseases of the heart is ranked at the top for Hispanics, blacks, and American children. In 2003, it was estimated that 7.7% of Hispanics have heart disease, 4.5% have cardiovascular heart disease; 19% must deal with hypertension, which is associated with the development of heart disease and 2.2% have suffered stroke [1].
Figure 1: Disparities in Selected Health Indicators by Race/Ethnicity, US  Table 1: Percentage of Excellent or Very Good Health vs. Ethnicities
Table 1: Percentage of Excellent or Very Good Health vs. Ethnicities