Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
Pain management center
PAIN MANAGEMENT CENTER PATIENT HISTORY
NAME: _______________________________________________________________
Please fill in completely (0) all circles (yes and no) as pertaining to your current symptoms. Constitutional Musculoskeletal Ophthalmology Neurology Dermatology Endocrinology Cardiology Hematology/Lymph Respiratory Allergy/Immune system Gastroenterology Psychology Male reproductive Female reproductive
How long have you had your pain? O 0-6 months O 6-12 months
O 1-5 years O 5-10 years O longer than 10 years
In the last 2-3 weeks when does your pain occur?
On a scale of 0 to 10, with 10 being the worst pain, mark where the severity of your pain is. O 0
Associated numbness O Yes O No Associated Tingling O Yes O No What was the setting when the problem first occured?
O prolonged keyboard activity O repetitive grasping
O sports (without obvious trauma) O squatting
Please describe your pain (quality): O aching
O penetrating O pins and needles O pressure
Please indicate those activities that INCREASE your pain: (check all that apply) O work
O foods or beverages O locale (i.e. home/work/etc.)
O medications O menstrual cycle O physical activites
O recreational drug use O sleep-related factors
Please indicate those activities that DECREASE your pain: (check all that apply) O walking
O emergency room treatment O elevating the affected area
O non weight bearing O supporting the extremity O avoiding stress
O language difficulty O mental status change
How many ER visits have you had in the last 3 months for pain?
Do you take any of the following anticoagulants? (check all that apply)
Have you tried any of these therapies: O acupressure
O nerve stimulation O occupational therapy
Have you tried any of these pain clinic treatments: O injection therapy O medications O physical therapy
Have you tried the following NSAIDS to help relieve your pain: O ibuprofen O aleve
Are you on Workers Comp?
Mark the appropriate information related to Worker's Compensation:
O unable to work at all since the injury
O able to work with restrictions since the injury
O temporary limitations after the injury
Litigation pending: O Yes
If you are involved in any lawsuits, who is the lawsuit against? (Check all that apply) O Worker's Compensation O Auto accident
Have you been to any of the following types of doctors? O Back Surgeon
Past Medical History Heart disease
Thyroid/endocrine problem O Yes O No Family History Is your father still alive?
Do you have children or other dependents at home? O Yes O No Social History What is your marital status? Are you currently employed? Are you on Disability? What type of disability do you have? Do you use alcohol to control your pain? O Yes O No Mark if you use any of the following drugs recreationally: O Amphetamines Dependency or addiction to drugs now or in the past? (Check all that apply) O Amphetamines
O Marijuana O Morphine O Oxycodone O Soma
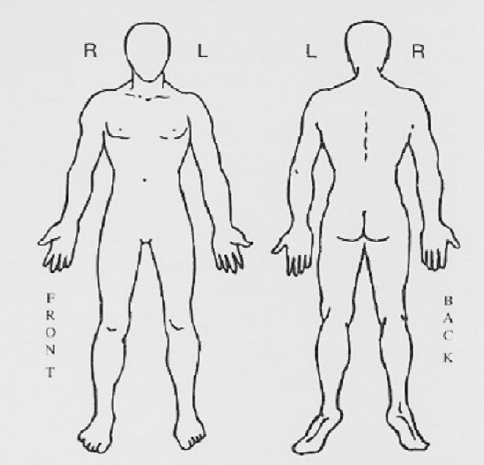
Please mark your pain area(s) on this diagram.
A NEW Sexual Assault Referral Centre is set to open in North Wales. Feb 18 2009 Daily Post North Wales Police Authority has authorised the majority of the £700,000 funding for the centre which will open in Colwyn Bay. It will specialise in investigating sex crimes and providing support for victims. Detective Superintendent Alan Green, Head of the Force’s Public Protection Unit, said:
Forme juridique Objectif de gestion Le FCP a pour objectif d’obtenir une performance supérieure à celle de l’indicateur de référence pour optimiser le rendement de contratsd'assurance-vie libellés en unités de compte relevant de l'option dite "DSK". Date de création Catégorie Engine - EuroPerformance Performances * Cumulées Classification AMF
 Please mark your pain area(s) on this diagram.
Please mark your pain area(s) on this diagram.