Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
Vandenelzen.info
Alimentary Pharmacology & Therapeutics
Review article: a critical view on impaired accommodation astherapeutic target for functional dyspepsia
B . D . J . V A N D E N E L Z E N & G . E . E . B O E C K X S T A E N S
Several important pathophysiological mechanisms have been identifiedin functional dyspepsia, however a complete understanding of these
mechanisms and beneficial therapeutic strategies are still lacking. Based
on the currently available literature we aimed at providing a critical
view on one of these pathophysiological mechanisms, impaired accom-
Although impaired gastric accommodation is identified as a major
pathophysiological mechanism, the clinical evidence supporting its role
as an important therapeutic target is currently still lacking. Treatment
with fundic relaxant drugs has shown conflicting results and has been
These negative findings could be explained by the fact that impaired
fundic accommodation is part of a more complex disorder involvingother regions of the proximal gut or by the increasing insight that cen-tral mechanisms may play an important role. Future studies of impairedaccommodation should take these considerations into account.
Journal compilation ª 2006 Blackwell Publishing Ltddoi:10.1111/j.1365-2036.2006.02930.x
1500 B . D . J . V A N D E N E L Z E N A N D G . E . E . B O E C K X S T A E N S
With the introduction of the barostat, it became
possible to study subtle changes in tone, either in
Functional dyspepsia (FD) is a common disorder char-
response to meal intake or to a pharmacological agent.
acterized by persistent or recurrent pain or discomfort
The first studies in dogs revealed that soon after meal
centred in the upper abdomen without evidence of
intake, the proximal stomach relaxes creating a reser-
organic disease likely to explain the symptoms.1 A
voir for the ingested food. As gastric emptying pro-
broad variety of symptoms such as fullness, bloating,
gresses, fundic tone recovers, returning to its basal
early satiety, epigastric pain, nausea, weight loss,
value.18, 19 Vagal cooling abolishes gastric relaxation
belching and vomiting have been reported by patients
illustrating that this motor pattern is vagally medi-
with FD. Although symptoms can occur at any time,
ated.20 In addition, in man, meal ingestion results in a
patients often relate the onset or aggravation of their
prolonged relaxation of the proximal stomach.15, 21–24
This relaxation is mimicked not only by distension of
Several pathophysiological mechanisms underlying
the duodenum and antrum, but also by infusion of
FD such as delayed gastric emptying,5, 6 abnormal
nutrients in the duodenum. These findings indicate
antroduodenal motility,7, 8 altered sensitivity to duode-
that both distension of the antrum and the duodenum
nal lipid or acid exposure,9–11 visceral hypersensitiv-
by the meal and activation of vagal afferents by nutri-
ity12, 13 and impaired fundic accommodation14, 15 have
ents in the duodenum contribute to create a reservoir
been identified. However, the current knowledge of
for the meal by relaxing the proximal stomach.18, 25
these pathophysiological mechanisms has not led to a
As such, food will preferentially remain in the prox-
complete understanding of FD. Furthermore, attempts to
imal stomach preventing filling of the antrum and the
develop therapeutic strategies based on this knowledge
have thus far not banned dyspepsia from our midst.
Basal gastric tone is maintained by a balance
Together with visceral hypersensitivity and delayed
between cholinergic excitatory activity and non-adr-
gastric emptying, impaired accommodation is the most
energic non-cholinergic inhibitory input. The inhibi-
frequently observed pathophysiological mechanism in
tion of basal gastric tone is predominantly regulated
patients with FD. All three mechanisms have inde-
by vagal inhibitory input which stimulates the release
pendently been reported in approximately 40% of the
of nitric oxide (NO) as principle neurotransmitter at
functional dyspeptic patients.2–4 In this paper we aim
the neuromuscular junction. Animal studies have con-
at providing a critical view of the current knowledge
sistently shown that basal tone is decreased by vagal
regarding one of these pathophysiological mechanisms
stimulation and that this effect is blocked by the spe-
involved in FD, namely impaired fundic accommoda-
cific NO inhibitor, NG-nitro-L-arginine (L-NNA).26, 27
tion and its potential as a therapeutic target in the
The use of another NO inhibitor, N-G-monomethyl-L-
arginine (L-NMMA), confirmed the involvement of NOin gastric relaxation in humans.28, 29 The gastricaccommodation to a meal can be mimicked by phar-
macological interventions. This can be achieved by sti-
Gastric relaxation in response to meal intake was first
described by Cannon and Lieb16 almost a century ago.
neurones (sumatriptan)30, 31 or by administration of
This gastric accommodation response reduces meal-
NO donors such as nitroglycerine.32, 33 Second, reduc-
induced increase in gastric pressure and might thus
tion in the cholinergic input, as shown for clonidine33
impair the development of dyspeptic symptoms. Gas-
will also lead to a reduction in tone, a mechanism that
tric accommodation consists of two types of relaxa-
has been advocated to be useful in improving meal-
relaxation. The receptive relaxation is triggered byactivation of pharyngeal and oesophageal mechanore-
ceptors. When the bolus reaches the stomach, the gas-
relaxation, which modulates gastric tone in response
The first indication of impaired gastric accommodation
to specific nutrients.17 Both reflexes contribute indis-
in FD patients was derived from scintigraphic and
tinguishably to the gastric accommodation response.
ultrasound studies.22, 34 These studies observed an
ª 2006 The Authors, Aliment Pharmacol Ther 23, 1499–1510Journal compilation ª 2006 Blackwell Publishing Ltd
R E V I E W : I M P A I R E D G A S T R I C A C C O M M O D A T I O N
abnormal intragastric distribution of food in FD
tes mellitus. Several studies have indicated that the
patients with accumulation of the meal in the distal
gastric accommodation reflex is hampered in patients
stomach. Later, barostat studies revealed that the
with diabetic neuropathy.42, 43 Animal studies revealed
relaxation of the proximal stomach to meal intake is
that one possible mechanism is impaired NOS expres-
impaired in approximately 40% of the patients with
FD.15, 35 Furthermore, the relaxation of the proximal
Another possible underlying mechanism leading to
stomach to distension of the antrum and infusion of
impaired accommodation is abnormal vagal input to
nutrients in the duodenum is impaired in a subgroup
the nitrergic neurones. Disturbed vagal efferent func-
of FD patients.36 This impaired accommodation of the
tion, as evidenced by altered respiratory sinus dys-
proximal stomach will lead to an abnormal meal dis-
rhythmia or diminished pancreatic-polypeptide release
tribution, as observed in the earlier scintigraphic and
in response to the insulin-induced hypoglycaemia test
ultrasound studies,22, 34 with increased filling of the
has been reported in FD patients.45–48 In diabetic
distal stomach. Especially as the antrum of patients
patients, vagal tone was significantly correlated with
with FD is hypersensitive to distension,36 impaired
the maximal postprandial volume response,42, 49 fur-
accommodation may significantly contribute to the
ther corroborating to a possible role of altered vagal
development of meal-induced symptoms. Tack et al.
input in impaired accommodation. Abnormal activa-
indeed showed that the prevalence of early satiety and
tion of duodenal vagal afferents by either nutrients or
weight loss is significantly greater in patients with
local release of hormones may also lead to impaired
impaired accommodation and that the impaired caloric
activation of the motor response. FD patients indeed
intake in these patients can be increased by pretreat-
have a less pronounced fundic relaxation in response
to duodenal nutrients.36, 50 On the other hand, abnor-mal exposure of the duodenum to acid51 leads to ablunted meal-induced relaxation in healthy volunteer
(HV). This finding together with the observation that
duodenal acid clearance in FD is impaired, points
Although impaired gastric accommodation is consid-
towards a role for duodenal acid in an abnormal
ered an important pathophysiological mechanism in
motor response of the proximal stomach to meal
the development of FD, surprisingly little is known
intake.52 Finally, an abnormal response to the arrival
about the aetiology of impaired gastric accommoda-
of lipids in the duodenum has also been suggested to
tion. Theoretically, gastric accommodation can be
play an important role in the generation of dyspeptic
hampered at any level of the reflex arc, both at the
symptoms.9, 25 Duodenal lipids relax the proximal
afferent and efferent arm of the pathway, including
stomach, but to a lesser extent in patients with FD.50
Future studies are certainly warranted to further clar-ify their role in the gastric accommodation response. A more detailed review on the role of food in the
pathogenesis of FD is reported elsewhere.2
One plausible mechanism leading to impaired gastricaccommodation is neuronal damage of the enteric
neurones, either postinfectious or as part of the pro-gression of a systemic disease such as diabetes. Similar
The efferent output of the vagal nerve is determined
to other functional gastrointestinal disorders such as
by the motor neurones in the dorsal vagal complex.53
the irritable bowel syndrome and gastroparesis,37–40
These neurones can be stimulated by microinjection of
FD has been associated with acute intestinal infections
L-glutamate, one of the main afferent neurotransmit-
in 17% of patients.41 Tack et al. clearly illustrated that
ters released in the brain stem, resulting in pro-
impaired accommodation is significantly more preval-
nounced gastric relaxation in mice.54 The dorsal motor
ent in patients with presumed postinfectious dyspepsia
nucleus of the vagal nerve not only receives afferent
compared with unspecified-onset dyspepsia (67% vs.
information from the nucleus tractus solitarius (NTS).
30%; P < 0.05),41 most likely resulting from dysfunc-
It also receives input from the locus coeruleus, the
tion of the nitrergic neurones.41 Neuronal damage can
also be afflicted by a systemic disorder such as diabe-
and the anterior cingulate cortex,55 brain regions
ª 2006 The Authors, Aliment Pharmacol Ther 23, 1499–1510Journal compilation ª 2006 Blackwell Publishing Ltd
1502 B . D . J . V A N D E N E L Z E N A N D G . E . E . B O E C K X S T A E N S
important for regulation of arousal, emotions and auto-
manner, and (ii) what is the clinical evidence that
nomic or behavioural responses.56–58 At this level,
impaired accommodation indeed represents an import-
stress and emotions can significantly alter the auto-
nomic output. It therefore seems plausible that stress oranxiety affects the vagal output to the stomach leading
HO W T O S E L E C T PA T IE N T S W I T H I M P AI RE D
to impaired gastric accommodation. Recent studies
indeed show that experimentally induced anxietyresults in impaired meal-induced accommodation in
At present, the gold standard to detect impaired gastric
HV.59, 60 However, this finding needs to be confirmed
accommodation is the gastric barostat, a computerized
in studies with FD patients. A more detailed review of
pump that measures volume changes under constant
this issue is provided by Van Oudenhove et al.61
pressure in an intragastric balloon.62 This procedure ishowever invasive and stressful and above all, the pres-ence of the balloon interferes with normal gastric
physiology.63, 64 Therefore, the use of other diagnostic
tools to study proximal and distal stomach function
The clinical relevance of impaired gastric accommoda-
tion as a pathophysiological mechanism in FD wasfirst
impaired accommodation is present in a substantialproportion of FD patients, is associated with early sati-
As impaired accommodation has been associated with
ety and weight loss, and gastric relaxation improved
early satiety,15 one option would be to select patients
drinking capacity in a small group of FD with
based on symptoms. Tack et al. indeed provided evi-
impaired accommodation.15 These considerations make
dence that increasing severity of early satiety was
impaired gastric accommodation an important thera-
accompanied by lower tolerated nutrient drink vol-
peutically target and have been the trigger to develop
umes, which in turn predicted the presence of impaired
new pharmacological agents aiming at relaxing the
accommodation.65 Other investigators however fail to
illustrate such a relationship. Bredenoord et al. conclu-
Although the concept of improving gastric accom-
ded that symptoms alone cannot predict physiological
modation is very appealing, there are still some very
disturbances such as gastric accommodation or empty-
important unsolved practical issues for the clinician.
ing in patients with unexplained upper gastrointestinal
First, if treatment aims at restoring fundic accommo-
symptoms. Similarly, we were unable to find a rela-
dation, ideally one should be able to select those
tionship between symptoms and proximal stomach
patients who will benefit most, i.e. patients with
function. Conversely, the symptom profile evoked by a
impaired accommodation. In most studies reported so
drink test is comparable in FD patients with impaired
far, abnormal proximal stomach function has been
accommodation or visceral hypersensitivity.35 These
identified by barostat studies. However, as this tech-
findings, together with the fact that FD presents with a
nique is time consuming, and above all invasive, it is
variety of symptoms4, 35 imply that the clinician can-
simply impossible to subject all patients to a barostat.
not simply rely on presenting symptoms to predict
Therefore, noninvasive techniques evaluating proximal
whether or not a patient may benefit from fundic
stomach function are certainly required to replace the
barostat. Second, although there are several argumentsto accept that impaired fundic relaxation is associated
with FD, we still have no real proof of the conceptthat correction of impaired fundic relaxation leads to
Recently, a drink test was suggested as a noninvasive
improvement of symptoms in patients with FD. Indi-
alternative to the barostat to detect impaired accom-
rectly this may question the importance of impaired
modation. Tack et al. showed a good correlation
accommodation as an important therapeutic target. In
between a nutrient drink test at a rate of 30 mL/min
the following part of this review, we addressed these
and impaired accommodation as measured by the bar-
two important issues: (i) How can we select patients
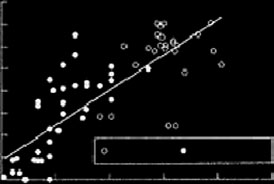
ostat in FD patients (r ¼ 0.71, P < 0.001) (Figure 1a).
with impaired fundic accommodation in a noninvasive
At a cut-off of 400 kcal, the sensitivity and specificity
ª 2006 The Authors, Aliment Pharmacol Ther 23, 1499–1510Journal compilation ª 2006 Blackwell Publishing Ltd
R E V I E W : I M P A I R E D G A S T R I C A C C O M M O D A T I O N
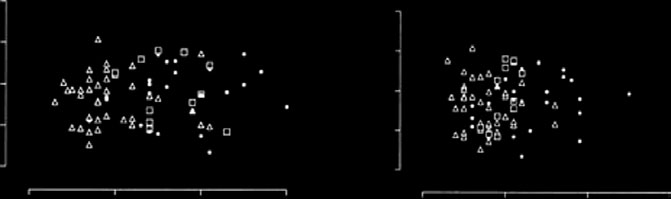
Figure 1. (a) Relationship between the maximal ingested volume with a 30-mL/min drink test and meal-induced accommo-dation. A significant correlation was found (r ¼ 0.76, P < 0.01)65 (with kind permission from BMJ Publishing Group). (b) Individual data showing the relationship between the postprandial fundic accommodation and the maximal ingestedvolume of water and Nutridrink with a 100-mL/min drink test in HV (d), MS (h) and FD (n). No significant correlationwas found66 (with kind permission from American Gastroenterological Association). It is suggested that the discrepancybetween these results derives from the difference in drinking speed (30 mL/min vs. 100 mL/min). With the rapid drink testpatients reach their maximum drinking capacity before reaching the maximal accommodation volume,67 whereas the slowdrink test is more likely to be affected by gastric emptying.66
of a slow nutrient drink test in predicting impaired
the rapid drink test was inappropriately timed as
accommodation were 92% and 86% respectively.
patients reached their maximum drinking capacity
However, it should be emphasized that the study pop-
before reaching the maximal accommodation vol-
ulation consisted of patients with severe dyspepsia of
ume,67 whereas a slow drink test is more likely to be
which some even had received total parental nutrition.
affected by gastric emptying.66 Nevertheless, before
It remains therefore questionable to what extent this
accepting the slow drink test as a noninvasive tool
applies to the majority of FD. We previously showed
replacing the barostat, it certainly should be validated
that both the water and nutrient drink test at a rate of
in the majority of patients with dyspepsia seen by the
100 mL/min are good tools to evoke dyspeptic symp-
general practitioner. To date, the only study available
toms and are useful to discriminate healthy volunteers
addressing this issue could not demonstrate a relation-
from patients with FD.35 However, with this drink test
ship between the findings during the drink test when
we were unable to predict impaired gastric accommo-
compared with single photon emission computed
dation as assessed by the gastric barostat (Figure 1b).66
tomography (SPECT) scanning.68 On the other hand,
The difference between these two studies may be
several studies have illustrated that it is a valuable
explained by the drinking rate. It was suggested that
tool to elicit symptoms in FD, and thus may be
ª 2006 The Authors, Aliment Pharmacol Ther 23, 1499–1510Journal compilation ª 2006 Blackwell Publishing Ltd
1504 B . D . J . V A N D E N E L Z E N A N D G . E . E . B O E C K X S T A E N S
useful to evaluate the effect of drugs on symptoms,
unclarities or inconsistencies however remain in the
Relationship between dyspeptic symptoms and
Single photon emission computed tomography, 3-D
To be considered an important therapeutically target,
ultrasound and magnetic resonance imaging (MRI) are
there should be a clear causal relationship between
relatively new methods allowing noninvasive assess-
ment of gastric volume. Due to their noninvasive nat-
under study. One well-designed study in 40 FD
ure, these techniques are patient friendly and provide
patients showed that impaired gastric accommodation
more physiological data compared with the gastric
measured by gastric barostat was indeed associated
barostat. Their capacity to detect volume changes
with symptoms of early satiety and weight loss.15
makes them suitable to investigate the accommodation
The association between early satiety and impaired
response. Gilja et al. demonstrated impaired gastric
accommodation was later also demonstrated in a
relaxation in FD patient by ultrasound,22 whereas Kim
study using planar scintigraphy, whilst a study based
et al. showed that SPECT could detect an impaired
on SPECT found an association with impaired accom-
volume response to food ingestion in FD patients.69
modation and weight loss.69, 74 However, other stud-
For an excellent review on the value of these tech-
ies using a gastric barostat or SPECT could not
niques to measure gastric accommodation we refer to
confirm the relationship between impaired accommo-
De Schepper et al.70 In contrast to the barostat, these
dation and early satiety, nor could these studies
techniques rather detect the volume of the intragastric
establish a correlation between gastric accommoda-
content after meal intake, and not gastric tone or
tion and any one of the dyspeptic symptoms in 44,
relaxation. We previously showed that the positive
32 and 151 FD patients respectively.35, 69, 75 Hence it
pressure applied by the barostat amplifies subtle chan-
remains debatable if impaired gastric accommodation
ges in tone allowing better and more adequate quanti-
plays a direct role in symptom generation or that
fication of gastric relaxation compared with SPECT
it is part of a more complex mechanism leading to
imaging. This was illustrated by a lack of correlation
in glucagon-induced gastric accommodation betweenSPECT scanning and the gastric barostat.71 Therefore,
Inhibition of fundic relaxation should lead to
in our view, these techniques are unsuitable to evalu-
ate changes in gastric tone. Nevertheless, SPECT scan-ning, MRI or 3-D ultrasound are very interesting tools
When impaired gastric accommodation plays a key
to study other aspects of gastric function, thus provi-
role in the development of dyspeptic symptoms, it
ding a more physiological view on intragastric vol-
should be possible to modulate dyspeptic symptoms by
ume, volume distribution and on gastric emptying
pharmacological substrates affecting the fundic relaxa-
tion response. Indeed, Tack et al. demonstrated thaterythromycin, sumatriptan and cisapride all affecteddrinking capacity as expected based on their known
I S I M P A I R E D A C C O M M O D A T I O N AN
effects on fundic accommodation.15, 65 However, an
I M P O R T A N T T H E R A P E U T I C T A R G E T ?
increased drinking capacity does not necessarily indi-
From a pathophysiological point of view, there is
cate a decrease in dyspeptic symptoms as demonstra-
abundant evidence to accept that impaired accommo-
ted by another study where sumatriptan influenced
dation may contribute to the generation of dyspeptic
drinking capacity but failed to affect dyspeptic symp-
toms after a drink test.35 Other studies even reported a
increased fundic pressure, shown to be related to
decrease in meal or fat-induced dyspeptic symptoms
symptoms especially in the presence of visceral hyper-
after blocking the gastric accommodation response by
sensitivity.73 In addition, the meal will be pushed
either L-NMMA, a NO synthase inhibitor28 or dexlox-
towards the less compliant antrum leading to overfill-
iglumide, a cholecystokinin (CCK) antagonist that
ing and consequently dyspeptic symptoms.36 Several
ª 2006 The Authors, Aliment Pharmacol Ther 23, 1499–1510Journal compilation ª 2006 Blackwell Publishing Ltd
R E V I E W : I M P A I R E D G A S T R I C A C C O M M O D A T I O N
Abnormal function Abnormal function
Figure 2. (a) A casual relationship between an abnormal function and a symptom. Correction of the abnormal functionwould lead to symptom improvement. (b) The abnormal function as an epiphenomenon sharing a common underlyingcause with the symptoms. Correction of the abnormal function would not lead to symptom improvement.
agents on proximal stomach function has been evalu-
Impaired accommodation: a pathophysiological
ated. However, the evidence that these agents indeed
reduce symptoms is very scarce and will be discussed
In general, there are at least two ways by which symp-
toms can be related to an abnormal motor patternsuch as impaired accommodation. The symptom can
either be a direct result of the mechanism under studyor be indirectly related to it by sharing a common
Nitric oxide has been identified as the principle neuro-
underlying cause (Figure 2). In the latter, the abnormal
transmitter involved in gastric relaxation.78, 79 Admin-
motor pattern is not causally related to the symptom
istration of NO donors relaxes the proximal stomach
but should rather be considered an epiphenomenon.
in humans,32, 33 and improves accommodation of the
Targeting this mechanism with pharmacological agents
proximal stomach to a meal. Sublingual nitroglycerine
will then consequently not lead to improvement of
reduced postprandial pain and nausea scores in FD.32
symptoms. Instead, the disorder giving rise to the
However, the use of NO donors is generally associated
abnormal motor pattern should be corrected. For
with significant side effects such as reduction in blood
pressure, tachycardia and headache. Especially the lat-
increasingly recognized in the aetiology of functional
ter may have distracted the attention leading to lower
gastrointestinal disorders.76, 77 Stress or central dys-
postprandial scores. In addition, these side effects ren-
function may lead to abnormal processing of visceral
der this class of drugs less suitable as a treatment
incoming information with increased perception, lead-
option for FD. An alternative for NO donors would be
ing to abnormal autonomic output and impaired effer-
sildenafil, a phosphodiesterase blocker that prolongs
ent vagal output. The recent finding that anxiety can
the relaxant properties of NO-mediated smooth muscle
impair meal-induced relaxation supports this hypothe-
relaxation. Pretreatment with sildenafil relaxes the
sis.59 These considerations would rather plead for cen-
proximal stomach in healthy volunteers.80 However,
tral acting agents instead of peripherally acting fundic
whether it also restores impaired gastric accommoda-
tion or improves dyspeptic symptoms remains to bedetermined.
Fundic relaxation as a treatment: the clinicalevidence
Since the introduction of impaired accommodation as
The role of serotonin (5-HT) as a neurotransmitter of
a therapeutic target, the effect of several relaxant
intrinsic neurones in the vagally mediated gastric
ª 2006 The Authors, Aliment Pharmacol Ther 23, 1499–1510Journal compilation ª 2006 Blackwell Publishing Ltd
1506 B . D . J . V A N D E N E L Z E N A N D G . E . E . B O E C K X S T A E N S
relaxation was first described in mouse and guinea-pig
could not establish an effect of SSRIs on gastric
by Bulbring and Gershon.81 5-HT1 receptor activation
volumes94, 95 or fasting compliance.94, 95 In HV, i.v.
by f.e. sumatriptan relaxes the proximal stomach
citalopram even inhibits gastric accommodation,96
in both animals and man by releasing NO.30, 82, 83
suggesting that effects on symptom improvement of
In humans, sumatriptan induces an immediate and
this type of drugs is more likely mediated by their
profound relaxation of the gastric fundus15, 31, 84 and
effects on the central nervous system.
patients with early satiety.15 It should be emphasized
though that caloric intake during the drink test wasstill only half of the amount ingested by healthy con-
Another approach to influence gastric accommoda-
trols, and the effect on dyspeptic symptoms was not
tion is through the sympathetic innervation. Cloni-
evaluated. Other investigators failed to confirm the
dine, an a2 receptor agonist, has been shown to
effect of sumatriptan on meal intake in HV and FD
relax the proximal stomach, enhance accommodation
patients with impaired accommodation and sumatrip-
and to reduce gastric sensations.33 However, the
tan did not affect postprandial symptoms.35, 85 Buspi-
effects on gastric accommodation were only present
rone, a 5-HT1 agonist, improved meal-induced gastric
at lower doses (<0.1 mg), whereas the effect on gas-
accommodation in 18 FD patients and reduced meal-
tric discomfort became prominent at the higher dose
related symptoms by 50%.86 Buspirone however is a
(0.1 mg). Other distension-evoked symptoms were
potent anxiolytic drug which may have greatly contri-
not affected by clonidine. Therefore, as the authors
state, their data suggest a specific effect on afferent
Recently, the effect of a new specific 5-HT1a receptor
nociceptive pathways, rather than an effect mediated
agonist R137696, shown to relax the proximal stom-
by relaxation of the stomach. Similar to these find-
ach of HV,87 was evaluated in a randomized placebo-
ings, clonidine (0.5 mg) only improved postprandial
belching in a study with eight FD patients and did
however failed to improve fundic accommodation and
dyspeptic symptoms.88 Tachyphylaxis or inadequate
indicate that the gastric relaxant capacity of cloni-
dosing may however have contributed to the negative
dine is not related to an improvement in dyspeptic
Other 5-HT agonists such as tegaserod, a partial
5-HT4 agonist, failed to enhance meal-induced gastric
although there was a significant effect on meal-
In general, the clinical evidence of a role for fundic
induced gastric volume increase in a subgroup of FD
relaxation as therapeutic strategy in FD is rather lim-
patients with normal gastric emptying.89 A recent
ited. Several factors could have contributed: one
study showed a significant effect on gastric accommo-
plausible explanation could be that fundic relaxant
dation with tegaserod in a small group (n ¼ 12) of
drugs also relax the distal stomach leading to delayed
HV.91 In FD patients however, tegaserod had no
gastric emptying80, 97 and an increase in antral diam-
effect on gastric accommodation and showed no bene-
eter.84 As mentioned earlier, antral distension is
ficial effect on the satisfactory relief of dyspeptic
already present in FD patients34, 98, 99 and the less
compliant antrum was shown to be sensitive to disten-sion.36, 100 Sumatriptan has been shown to increaseantral area in HV84 which may perhaps explain why
Selective serotonin reuptake inhibitor (SSRI)
sumatriptan and R137696 had no effect on dyspeptic
Based on the concept that 5-HT is involved in vagally
symptoms. This would suggest that the ideal drug
mediated relaxation,92 several studies focused on the
should relax the proximal stomach but increase tone
use of SSRI to prolong endogenous 5-HT availability
in order to improve gastric accommodation. Although
Other explanations include receptor tachyphylaxis
paroxetine increased gastric accommodation after food
or the use of inappropriate doses. Receptor tachyphy-
intake, the difference between the paroxetine and pla-
laxis is a well-known problem of 5-HT receptor agon-
cebo group was small.93 Furthermore, other studies
ists101, 102 and may well explain the negative results
ª 2006 The Authors, Aliment Pharmacol Ther 23, 1499–1510Journal compilation ª 2006 Blackwell Publishing Ltd
R E V I E W : I M P A I R E D G A S T R I C A C C O M M O D A T I O N
after long-term use. In addition, patients with FD may
relaxation, the aetiology of this pathophysiological
require higher doses of the drug under study compared
mechanism remains largely unknown, and both central
with HV. In the R137696, application of 2 mg did not
and peripheral factors may be involved. The relation-
result in an increase in meal-induced accommoda-
ship between dyspeptic symptoms and a pathophysio-
tion,88 whereas this dose resulted in a significant
logical mechanism such as impaired accommodation is
obviously very complex. Although impaired gastric
Finally, the weak causal relationship between dys-
accommodation is identified as a major pathophysio-
peptic symptoms and impaired accommodation would
logical mechanism, the clinical evidence for impaired
provide another explanation for the disappointing
accommodation as an important therapeutic target is
results on fundic relaxant therapy. If impaired accom-
currently still lacking. Treatment with fundic relaxant
modation only moderately contributes to symptom
drugs thus far has shown conflicting results and has
generation, treatment should perhaps aim preferen-
been rather disappointing in general. These negative
tially at other more important mechanisms (Figure 2).
findings could be explained by the fact that impaired
Whether this hypothesis is valid and whether central
fundic accommodation is part of a more complex dis-
mechanisms or peripheral mechanisms are involved as
order involving other regions of the proximal gut or
the underlying mechanism clearly remains to be eluci-
by the increasing insight that central mechanisms may
Although we understand more and more about the
B.v.d.E. is supported by a grant from Janssen Research
neural pathways involved in meal-induced fundic
imal duodenum in dyspeptic patients.
Gastroenterology 1999; 116: 515–20.
7 Bassotti G, Pelli MA, Morelli A. Duode-
13 Mertz H, Fullerton S, Naliboff B, Mayer
Clin Gastroenterol 1990; 12: 17–21.
of symptoms in functional dyspepsia.
15 Tack J, Piessevaux H, Coulie B, Caene-
4 Tack J, Bisschops R, Sarnelli G. Patho-
5 Jian R, Ducrot F, Ruskone A et al.
16 Cannon W, Lieb C. The receptive relax-
ª 2006 The Authors, Aliment Pharmacol Ther 23, 1499–1510Journal compilation ª 2006 Blackwell Publishing Ltd
1508 B . D . J . V A N D E N E L Z E N A N D G . E . E . B O E C K X S T A E N S
31 Tack J, Coulie B, Wilmer A, Andrioli A,
21 Azpiroz F. Control of gastric emptying
23 Moragas G, Azpiroz F, Pavia J, Malage-
test Liver Physiol 1993; 264: G1112–7.
tility in patients with functional dyspep-
sia. Psychosom Med 1993; 55: 12–22.
Ropert R, Galmiche JP, Berstad A. Gastric
37 Bityutskiy LP, Soykan I, McCallum RW.
pathic gastroparesis – clinical charac-
in diabetes – relation to vagal tone.
diarrhoea. Lancet 1996; 347: 150–3.
39 Gwee KA, Leong YL, Graham C et al.
50 Feinle C, Meier O, Otto B, D’Amato M,
41 Tack J, Demedts I, Dehondt G et al.
52 Lee KJ, Vos R, Janssens J, Tack J.
30 Coulie B, Tack J, Sifrim D, Andrioli A,
Janssens J. Role of nitric oxide in fast-
ª 2006 The Authors, Aliment Pharmacol Ther 23, 1499–1510Journal compilation ª 2006 Blackwell Publishing Ltd
R E V I E W : I M P A I R E D G A S T R I C A C C O M M O D A T I O N
gic nerves in the rat gastric fundus.
67 Tack J. Drink tests in functional dyspep-
ment of nitric oxide in the reflex relaxa-
food or fluid. Nature 1991; 351: 477–9.
80 Sarnelli G, Sifrim D, Janssens J, Tack J.
et al. Does the nutrient drink test accu-
Influence of sildenafil on gastric senso-
inhibitory innervation of the stomach.
82 Kojima S, Ishizaki R, Shimo Y. Investi-
58 Mertz H. Role of the brain and sensory
inga RE, Tytgat GNJ, Boeckxstaens GEE.
gastric barostat. Gut 2003; 52: 1548–54.
72 Lee KJ, Kindt S, Tack J. Pathophysiology
Clin Gastroenterol 2004; 18: 707–16.
73 Tack J, Caenepeel P, Corsetti M, Jans-
initial transpyloric flow in healthy sub-
86 Tack J, Piessevaux H, Coulie B, Fischler
gastroenterol Motil 2003; 15: 447–55.
87 Boeckxstaens G, Tytgat G, Wajs E et al.
64 Rao SS, Vemuri S, Harris B, Schulze K.
antral and duodenal motility in man.
stomach function in healthy volunteers.
testinal motility and sensitivity. Dig Dis
88 Tack J, Van Elzen B, Tytgat G et al.
77 Stam R, Akkermans LM, Wiegant VM.
tinal function. Gut 1997; 40: 704–9.
JJ et al. Release of nitric-oxide upon sti-
ª 2006 The Authors, Aliment Pharmacol Ther 23, 1499–1510Journal compilation ª 2006 Blackwell Publishing Ltd
1510 B . D . J . V A N D E N E L Z E N A N D G . E . E . B O E C K X S T A E N S
94 Chial HJ, Camilleri M, Ferber I et al.
99 Marzio L, Falcucci M, Grossi L et al.
troenterology 2005; 128 (Suppl. 2): A94.
90 Tack J, Vos R, Janssens J, Salter J, Jauf-
on the perception of gastric distension.
gastroenterol Motil 2002; 14: 395–402.
101 Salomone S, Morel N, Godfraind T.
enterology 2005; 128 (Suppl. 2): A469.
92 Notivol R, Coffin B, Azpiroz F, Mearin
102 Whalen EJ, Johnson AK, Lewis SJ.
93 Tack J, Broekaert D, Coulie B, Fischler
B, Janssens J. Influence of the selective
ª 2006 The Authors, Aliment Pharmacol Ther 23, 1499–1510Journal compilation ª 2006 Blackwell Publishing Ltd
VII. Access to Drugs and Formularies This section covers: • Pharmacy networks • Formularies • Cost-containment strategies • Transition policies Each Part D plan has a network of pharmacies from which an enrollee can routinely access his or her Part D drugs. Additionally, each Part D plan covers the prescription drugs that it places on a formulary, or list of covered d
Title Incremental Cost-Effectiveness (ICE) Statistical Inference from Two Unbiased SamplesAuthor Bob Obenchain <wizbob@att.net>Maintainer Bob Obenchain <wizbob@att.net>Description Given two unbiased samples of patient level data on cost and effectivenessfor a pair of treatments, make head-to-head treatment comparisons by (i) generating thebivariate bootstrap resampling distribution
 R E V I E W : I M P A I R E D G A S T R I C A C C O M M O D A T I O N
Figure 1. (a) Relationship between the maximal ingested volume with a 30-mL/min drink test and meal-induced accommo-dation. A significant correlation was found (r ¼ 0.76, P < 0.01)65 (with kind permission from BMJ Publishing Group).
R E V I E W : I M P A I R E D G A S T R I C A C C O M M O D A T I O N
Figure 1. (a) Relationship between the maximal ingested volume with a 30-mL/min drink test and meal-induced accommo-dation. A significant correlation was found (r ¼ 0.76, P < 0.01)65 (with kind permission from BMJ Publishing Group).