Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
Pii: s0886-3350(03)00575-3
Effect of amniotic membrane after laser-assisted subepithelial keratectomy on epithelial healing Clinical and refractive outcomes
Hyung Keun Lee, MD, Jin Kook Kim, MD, Sung Soo Kim, MD, Eung Kweon Kim, MD,Kwang One Kim, MD, In Sik Lee, MD, Gong Je Seong, MD
Purpose: To evaluate the effect of an amniotic membrane (AM) on reepithelialization time, corneal haze, and postoperative visual and refractive outcomes after laser- assisted subepithelial keratectomy (LASEK) for myopia and myopic astigmatism. Setting: Department of Ophthalmology, Yonsei University College of Medicine, and Balgeunsesang Ophthalmology Clinic, Seoul, Korea. Methods: One hundred fifty-two eyes of 84 patients with myopia or myopic astig- matism were prospectively evaluated for 6 months after LASEK. An AM was placed as a strip on the inferior limbus in 94 eyes of 54 patients after LASEK; 58 eyes of 30 patients served as the control group. Postoperative epithelial heal- ing time, uncorrected visual acuity (UCVA), best corrected visual acuity, remaining refractive error, and corneal haze were examined. Results: The reepithelialization time was shorter in the AM group (2.40 days Ϯ 0.94 [SD]) than in the control group (3.90 Ϯ 0.97 days) (PϽ.001). At 6 months, 86 eyes (91.5%) in the AM group had a UCVA of 20/25 or better and 90 eyes (95.7%) had a UCVA of 20/40 or better; 48 eyes (82.8%) and 53 eyes (91.4%) in the control group had a UCVA of 20/25 or better and 20/40 or better, respec- tively. The mean spherical equivalent in the AM group was Ϫ0.48 Ϯ 0.54 diopter (D) and in the control group, Ϫ0.94 Ϯ 0.60 D (PϽ.001). The corneal haze was sig- nificantly less in the AM group than in the control group (PϽ.001). Conclusion: Amniotic membrane use after LASEK induced rapid epithelial heal- ing with more favorable visual and refractive outcomes and lower corneal haze scores than conventional LASEK. J Cataract Refract Surg 2004; 30:334–340 2004 ASCRS and ESCRS
Laser-assisted subepithelial keratectomy (LASEK) ocular pain after surgery or stromal opacity similar to
was introduced and popularized with the advan-
tages of decreased pain, tearing, irritating symptoms,
Amniotic membrane (AM), the innermost mem-
and corneal opacity compared to photorefractive kera-
brane lining the placenta facing the fetus, is known to
tectomy (PRK). It also enables the correction of refrac-
induce rapid corneal epithelial healing and is used to
tive errors, especially in eyes with thin corneas.1,2 There
reconstruct the ocular surface in cases of partial limbal-
is, however, some controversy about the possibility of
cell deficiency and persistent epithelial defects.4–7 Recent
delayed epithelial healing resulting in complaints of
studies show that AM transplantation results in lessstromal infiltration of inflammatory cells and a reduced
Accepted for publication June 17, 2003.
loss of keratocytes in rabbit corneas.8,9 These results
Reprint requests to Eung Kweon Kim, MD, Institute of Vision Research,
suggest that AM application to the cornea after LASEK
Department of Ophthalmology, College of Medicine, Yonsei University,
would affect the epithelial healing pattern and stro-
134 Shinchon-dong, Sudaemoon-gu, Seoul, Korea. E-mail: eungkkim@yumc.yonsei.ac.kr.
This study prospectively evaluated the effect of AM
placement after LASEK on epithelial healing time, post-operative visual outcomes including refractive status andvisual acuity, and corneal opacities. Patients and Methods
One hundred fifty-two consecutive eyes of 84 patients
were enrolled between September 2000 and December 2001. The preoperative ophthalmic examination of all patients in-cluded slitlamp biomicroscopy, intraocular pressure, fundusexamination, pupil diameter measurements, Schirmer test,manifest refraction, corneal keratometry, corneal topography,corneal pachymetry, and visual field examination. No patienthad a history of refractive procedures or cataract surgery,
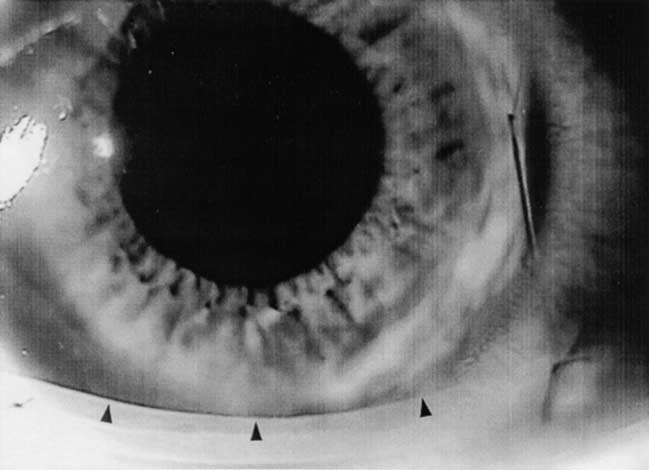
Figure 1.
(Lee) One day after LASEK with AM strip transplantation.
keratoconus, diabetes, glaucoma, connective tissue disorders,
Arrowheads mark the upper margin of the AM.
After the preoperative examinations, the patients were
proparacaine hydrochloride 0.5% (Alcaine) instilled. An
told about the AM and its intended use after LASEK. They
alcohol solution cone (J2905, Janach) with an 8.5 mm diame-
were also told that this might be the first human trial after
ter was placed on the eye. Twenty percent of the alcohol
photoablation, and written informed consent was obtained
solution was instilled inside the cone, left for about 20 sec-
once the patients agreed to participate. The patients who did
onds, and then carefully washed off with a balanced salt
not agree to the use of the AM on the LASEK-treated eye
solution so the epithelium around the flap was not disturbed.
were considered the control group after they provided in-
The epithelial flap was gently lifted with an epithelial
microhoe (J2915A, Janach). If the edges were difficult to lift,the alcohol application was repeated for another 10 seconds. Preparation of Preserved Human Amniotic Membrane
The epithelial flap was then peeled back as a sheet toward the
The AM was prepared following the methods of Lee
12 o’clock position using a spatula (J2910A, Janach). To avoid
and Tseng.10 Human placenta was obtained during an elective
tears in the epithelial flap, the basal lamina was carefully
Cesarean section in a seronegative (human immunodeficiency
separated from Bowman’s layer instead of separating the
virus, human hepatitis type B and C, and syphilis) woman.
epithelium from the basal lamina. If the epithelial flap was
Informed consent was obtained from the AM donor after the
not applied to the denuded stromal as an intact sheet, the
purpose of the AM was explained. Under a laminar flow hood,
the placenta was cleaned of blood clots with sterile phosphate-
Excimer laser treatment was performed in the usual man-
buffered saline solution containing penicillin 50 g/L,
ner using the nomogram for PRK with the EC-5000 laser
streptomycin 50 g/L, neomycin 100 g/L, and ampho-
system (Nidek). The flap was washed with a balanced salt
tericin B 2.5 g/L. The amnion was separated from the
solution and then repositioned carefully with a spatula. In
chorion by blunt dissection and flattened on a nitrocellulose
the control group, the treatment was finished with the appli-
paper, with the epithelium-basement-membrane surface fac-
cation of a therapeutic soft contact lens on the operated eye.
ing away from the paper. The paper with adherent AM was
In the AM group, the AM was washed thoroughly and
then cut into 1.5 cm blocks and stored at Ϫ80ЊC until
immersed in a balanced salt solution containing gentamicin
transplantation in a sterile vial containing Dulbecco’s modi-
8 g/L and cefaxolin 4 g/L for 30 minutes before sur-
fied Eagle medium (GIBCO Life Technologies, Inc.) and
gery. The membrane was then cut into 1.5 cm ϫ 0.3 cm
glycerol (GIBCO Life Technologies, Inc.) at the ratio of 1:1
rectangular pieces. With the mesenchymal side facing the
(vol/vol). Six months after delivery, the AM donors were
cornea, the membrane was attached to the stromal bed after
retested by the previous serologic examinations for the win-
excimer laser ablation. The slender AM strip was placed on
dow period of transmittable diseases. Only the AM that
the inferior limbus so it would not touch the ablated corneal
passed prenatal and postnatal serologic tests as seronegative
bed and secured with 2 interrupted 10-0 nylon sutures placed
on the limbal conjunctiva. A therapeutic soft contact lenswas also placed on the eyes with the AM strip (Figure 1). Laser-Assisted Subepithelial Keratectomy Procedure
One drop of ofloxacin 0.3% (Tarivid) and diclofenac
The LASEK procedure was the same in the control and
0.1% (Optanac) was given to the patients in both groups
AM groups. A speculum was applied to the patient’s eye and
immediately after LASEK. All patients were checked daily
J CATARACT REFRACT SURG—VOL 30, FEBRUARY 2004
illumination; 1, for an opacity of minimal density seen withdifficulty under direct and diffuse illumination; 2, for an
easily visible opacity; 3, for a dense opacity that significantly
Characteristics P Value
decreased visualization of intraocular structures such as the
iris and retina; and 4, for an opaque cornea.
Statistical analysis was performed using Statistical Analy-
sis System (version 6.12, SAS Institute Inc.). A P value lessthan 0.05 was considered statistically significant.
AM ϭ amniotic membrane; NS ϭ not significant
The AM group and the control group consisted of
94 eyes of 54 patients and 58 eyes of 30 patients,respectively. Preoperative data are shown in Table 1. There were no statistically significant differences be-tween the 2 groups in the preoperative independentvariables.
Eyes with an AM had a significantly faster rate of
epithelial healing than the control eyes (PϽ.001). Round or oval epithelial defects under the epithelialflap and therapeutic soft lens were observed on the dayof treatment; the defects decreased concentrically ateach follow-up. The mean epithelial healing time was2.40 days Ϯ 0.94 (SD) in the AM group and 3.90 Ϯ0.97 days in the control group. Three days after surgery,82 eyes (87.2%) in the AM group and 18 eyes (31.8%)in the control group were completely reepithelialized. Ten eyes (10.6%) in the AM group showed complete
Figure 2.
(Lee) Completion of epithelial healing in the control and
reepithelialization within 36 hours of surgery, and 2
eyes (3.45%) in the control group showed completereepithelialization after 5 days (Figure 2).
until the epithelial defect completely healed. They were in-
At 1 week, 61 eyes (64.9%) in the AM group and
structed to apply 1 drop of diclofenac and ofloxacin every
31 eyes (53.5%) in the control group had a UCVA
2 hours and artificial tears (Hyalein 0.1%) every hour until
of 20/25 or better. At 6 months, 48 eyes (82.8%)
Complete epithelialization was determined by daily slit-
in the control group had a UCVA of 20/25 and 53
lamp observation. Once the epithelium was healed, the thera-
eyes (91.4%), of 20/40 or better; in the AM group,
peutic contact lenses and AM, if used, were removed from
86 eyes (91.5%) had a UCVA of 20/25 or better and
the cornea. Then, ofloxacin 0.3% and fluorometholone 0.1%
90 eyes (95.7%), of 20/40 or better (Table 2).
(Fluorometholone) were administered 4 times daily for
There were no statistically significant differences in
1 week and 2 times daily for 1 month.
BCVA between the 2 groups during the follow-up.
Uncorrected visual acuity (UCVA), best corrected visual
acuity (BCVA), manifest refraction, tonometry, and slitlamp
Most patients in both groups showed no changes in
biomicroscopy were performed at each follow-up examina-
BCVA. However, 7 eyes (7.5%) in the AM group and
tion. Subepithelial corneal haze levels were checked with a
5 eyes (8.6%) in the control group lost 1 or 2 Snellen
slitlamp 1, 3, and 6 months after surgery. Two of the authors,
lines of BCVA at the final examination.
who did not know whether the eye examined was part of
Statistically significant differences in the mean refrac-
the AM group or the control group, observed and graded
tive error were found between 1 month and 6 months
the corneal opacities from 0 to 4, according to the methodof Hanna et al.11 A grade of 0 was given for “totally clear”;
(Table 3). At the final examination, 70 eyes (74.5%)
0.5, for a faint corneal opacity seen only by oblique indirect
in the AM group and 40 eyes (69.0%) in the control
J CATARACT REFRACT SURG—VOL 30, FEBRUARY 2004
Visual acuity results in the control and AM groups over time after LASEK. Month(s) After LASEK
AM ϭ amniotic membrane; LASEK ϭ laser-assisted subepithelial keratectomy*pϽ.01, chi-square test
group had a mean spherical equivalent (SE) within
in the control group had a corneal haze score greater
Ϯ0.50 diopter of the attempted myopic correction,
than 2 (PϽ.01). At 6 months, the AM group had a more
with a significant between-group difference (PϽ.01).
favorable corneal haze score. Forty-five eyes (47.8%) in
The cylinder magnitude between the groups was also
the AM group and 21 eyes (35.2%) in the control group
significantly different from 1 month to 6 months
had a haze score below grade 1. Three eyes (5.2%) in
the control group and 4 eyes (4.3%) in the AM group
Corneal haze was examined and graded under the
had grade 3 corneal opacity 6 months after surgery
slitlamp according to the previously described grading
system. At 1 month, the corneal haze score was less
The correlations between duration of the epithelial
than grade 1 in all eyes. But the AM group had less
defect, corneal opacity, SE, and cylinder magnitude in
haze than the control group (PϽ.01). At 3 months,
all eyes are shown in Table 4. The strongest correlation
8 eyes (8.5%) in the AM group and 20 eyes (34.7%)
was between corneal opacity and SE at 6 months (corre-lation coefficient ϭ Ϫ0.711, P ϭ .000). The correlation
Refractive error in the control and AM groups after
coefficient showed a positive correlation between the
duration of the epithelial defect and the stromal opacity
Mean D Ϯ SD
(r ϭ 0.653, P ϭ .000) and negative correlations between
Control Group P Value*
the stromal opacity and the SE (r ϭ Ϫ0.607, P ϭ
Discussion
From our results, we conclude that the epithelializa-
tion and the wound-healing process after LASEK was
influenced by the AM strip. Both visual and refractive
outcomes were acceptable in all patients. However, the
AM group had a shorter epithelial healing time and
more favorable visual and refractive outcomes. At the
beginning of the study, we used the AM to cover the
entire LASEK-treated surface directly. However, inmany eyes, the regenerated corneal epithelium was de-
tached during removal of the AM so a longer period
was needed for reepithelialization. We therefore modi-
AM ϭ amniotic membrane; Cyl ϭ cylinder; LASEK ϭ laser-assisted
fied the so-called overlay technique to use the AM as
subepithelial keratectomy; SE ϭ spherical equivalent*pϽ.05, Student t test
J CATARACT REFRACT SURG—VOL 30, FEBRUARY 2004
Corneal haze score in the control and AM groups after LASEK. Month(s) After LASEK
AM ϭ amniotic membrane; LASEK ϭ laser-assisted subepithelial keratectomy*pϽ.01, chi-square test
The exact mechanism of how AM use after LASEK
first is that the AM strip may act as a mechanical barrier
is effective in corneal epithelial healing was not demon-
against white-blood-cell migration that emerges from
strated in this study. The AM was not directly in contact
the limbal blood vessels or tear fluid in the conjunctival
with the wound bed, so the direct physical and mechani-
sac. After excimer laser refractive surgery, the concentra-
cal roles of the AM would hardly affect the wound
tion of inflammatory cells and cytokines such as trans-
healing after LASEK. A bandage soft contact lens
forming growth factor- is increased immediately.12,13
(BSCL) was used in both groups until the epithelial
The greatest amount of tear flow occurs in the meniscus
healing was complete. Both groups were studied at the
adjacent to the lower lid.14 The AM, which was placed
same time by the same surgeon and observers. We
on the inferior limbus, might act as a mechanical barrier
therefore think the BSCL had the same effect on both
so it would decrease inflammatory cell infiltration in
groups and did not act as a bias in 1 group.
the wound bed and reduce epithelial cell destruction
We suggest 2 possible mechanisms to explain how
by the white blood cells and the inflammatory factors
the AM strip facilitates corneal epithelial healing. The
The second possibility is that the various cytokines
Correlation coefficients between duration of epithelial de-
and epithelial-growth-associated factors within the AM
fect and corneal opacity, refractive error, and cylinder magnitude at
would help epithelial regeneration and wound healing
after LASEK. The AM has been shown to express epi-
dermal growth factor, hepatocyte growth factor, and
keratinocyte growth factor15 and suppress the proinflam-
matory cytokines during wound healing, just as interleu-
kin does.16 Although the exact role of these factors in
AM associated with facilitating cornea wound healing
is not known, the factors may play some role in corneal
epithelial healing. However, further studies of how the
AM promotes epithelial healing are needed.
The UCVA was better in the AM eyes than in the
control group from 1 week to 6 months after surgery.
We believe the faster epithelial healing that resulted in
a smoother refractive surface in the AM group provided
better UCVA a week after LASEK. At 6 months, cornealopacities, which might cause irregular astigmatism and
CM ϭ cylinder magnitude; DED ϭ duration of epithelial defect; SD ϭstromal opacity; SE ϭ spherical equivalent; Sig ϭ significance
increase postoperative refractive errors, were fewer in
J CATARACT REFRACT SURG—VOL 30, FEBRUARY 2004
2. Dastjerdi MH, Soong HK. LASEK (laser subepithelial
the AM group. We think these could be related to the
keratomileusis). Curr Opin Ophthalmol 2002; 13:261–
We did not find statistically significant differences
3. Litwak S, Zadok D, Garcia-de Quevedo V, et al. Laser-
in the BCVA between the 2 groups until 6 months
assisted subepithelial keratectomy versus photorefractive
postoperatively. After PRK or LASEK, the corneal haze
keratectomy for the correction of myopia; a prospective
is associated with BCVA loss.17 Up to 6 months postop-
comparative study. J Cataract Refract Surg 2002; 28:1330–1333
eratively, most patients showed no changes in BCVA
4. Azuara-Blanco A, Pillai CT, Dua HS. Amniotic mem-
and corneal haze below grade 2. We do not think this
brane transplantation for ocular surface reconstruction.
mild to moderate grade of corneal haze would affect
5. Tseng SCG, Prabhasawat P, Barton K, et al. Amniotic
Although the refractive outcomes in the 2 groups
membrane transplantation with or without limbal allo-
were relatively comparable, there was a statistically sig-
grafts for corneal surface reconstruction in patients withlimbal stem cell deficiency. Arch Ophthalmol 1998;
nificant difference in the remaining refractive errors.
Besides the spherical component of the postoperative
6. Tsubota K, Satake Y, Ohyama M, et al. Surgical recon-
refractive error, the magnitude of astigmatism was statis-
struction of the ocular surface in advanced ocular cicatri-
tically significantly different between the groups. More-
cial pemphigoid and Stevens-Johnson syndrome. Am J
over, we found correlations among corneal opacity,
7. Chen H-J, Pires RTF, Tseng SCG. Amniotic membrane
epithelial healing time, and remaining refractive errors.
transplantation for severe neurotrophic corneal ulcers.
From these results, we think it is possible that the AM
affects postoperative wound healing after LASEK.
8. Wang MX, Gray TB, Park WC, et al. Reduction in
The excessive synthesis of collagen and glycosami-
corneal haze and apoptosis by amniotic membrane ma-
noglycans by keratocytes in the ablation zone can lead to
trix in excimer laser photoablation in rabbits. J Cataract
a thickening that yields myopic regression, astigmatism,
9. Park WC, Tseng SCG. Modulation of acute inflamma-
irregular topography, and optical aberration.18 Tabin
tion and keratocyte death by suturing, blood, and amni-
et al.19 report that surgically induced refractive errors
otic membrane in PRK. Invest Ophthalmol Vis Sci
including astigmatism may be the result of irregular
epithelial thickening or epithelial hyperplasia. There-
10. Lee S-H, Tseng SCG. Amniotic membrane transplanta-
fore, the postoperative wound healing after excimer laser
tion for persistent epithelial defects with ulceration. AmJ Ophthalmol 1997; 123:303–312
surgery could significantly affect the postoperative visual
11. Hanna KD, Pouliquen YM, Waring GO III, et al. Cor-
and refractive outcomes. It is possible that corneal haze
neal wound healing in monkeys after repeated excimer
and surgically induced refractive errors could be regu-
laser photorefractive keratectomy. Arch Ophthalmol
lated and moreover reduced with antiinflammatory
12. Tuominen ISJ, Tervo TMT, Teppo A-M, et al. Human
In conclusion, a strip of AM fixed on the limbus
tear fluid PDGF-BB, TNF-␣ and TGF-1 vs cornealhaze and regeneration of corneal epithelium and subbasal
after LASEK may reduce the duration of epithelial de-
nerve plexus after PRK. Exp Eye Res 2001; 72:631–641
fects and decrease corneal haze, which improves visual
13. Ramirez-Florez S, Maurice DM. Inflammatory cells, re-
outcomes in LASEK eyes. Further studies are needed
fractive regression, and haze after excimer laser PRK.
to investigate the subcellular mechanisms of the AM
in facilitating epithelial healing. We also believe that a
¯ gu¯t MS, Bavbek T, Kazokoglu H. Assessment of tear
longer follow-up of the patients is needed.
drainage by fluorescein dye disappearance test after ex-perimental canalicular obstruction. Acta Ophthalmol1993; 71:69–72
References
15. Koizumi N, Inatomi T, Sotozono C, et al. Growth factor
1. Lee JB, Seong GJ, Lee JH, et al. Comparison of laser
mRNA and protein in preserved human amniotic mem-
epithelial keratomileusis and photorefractive keratec-
brane. Curr Eye Research 2000; 20:173–177
tomy for low to moderate myopia. J Cataract Refract
16. Solomon A, Rosenblatt M, Monroy D, et al. Suppression
of interleukin 1␣ and interleukin 1 in human limbal
J CATARACT REFRACT SURG—VOL 30, FEBRUARY 2004
epithelial cells cultured on the amniotic membrane stro-
pic astigmatism; the Melbourne Excimer Laser Group.
mal matrix. Br J Ophthalmol 2001; 85:444–449
J Cataract Refract Surg 1996; 22:924–930
17. Van Gelder RN, Steger-May K, Yang SH, et al. Compar-
ison of photorefractive keratectomy, astigmatic PRK,
From the Institute of Vision Research, Department of Ophthalmology,
laser in situ keratomileusis, and astigmatic LASIK in the
College of Medicine (H.K. Lee, S.S. Kim, E.K. Kim, Seong) and
treatment of myopia. J Cataract Refract Surg 2002; 28:
BK21 Project for Medical Science (E.K. Kim); Yonsei University; andBalgeunsesang Ophthalmology Clinic (J.K. Kim, I.S. Lee), Seoul, Korea.
18. Shah S, Chatterjee A, Smith RJ. Predictability and out-
Supported by a grant (02-PJ1-PG1-CH02-0003) from the Korea
comes of photoastigmatic keratectomy using the Nidek
Health 21 R&D Project, Ministry of Health and Welfare, Republic
EC-5000 excimer laser. J Cataract Refract Surg 2002;
19. Tabin GC, Alpins N, Aldred GF, et al. Astigmatic change
None of authors has a financial or proprietary interest in any prod-
1 year after excimer laser treatment of myopia and myo-
J CATARACT REFRACT SURG—VOL 30, FEBRUARY 2004
607 14th Street, NW, Suite 800 Washington, D.C. 20005 Tel: (202) 783-6040 Fax: (202) 783-6031 Email: slieberman@rfem.com Steven Lieberman Mr. Lieberman was born in New York City and admitted to the Bar of the State of New York in 1985 and the Bar of the District of Columbia in 1993. He is also admitted to practice before the United States Supreme Court; the United States Cour
DO NOT OPEN THIS EXAM UNTIL YOU ARE TOLD TO DO SO. Instructions Write your SUID in the upper right corner of this exam. Do NOT write your name. SHOW ALL YOUR WORK. Answers without supporting work will receive little or no credit. Do all your work on this exam. If you need extra space, write on the backs of the pages. However, if you do write an answer on the back of a page, be sure you've
 This study prospectively evaluated the effect of AM
placement after LASEK on epithelial healing time, post-operative visual outcomes including refractive status andvisual acuity, and corneal opacities.
This study prospectively evaluated the effect of AM
placement after LASEK on epithelial healing time, post-operative visual outcomes including refractive status andvisual acuity, and corneal opacities.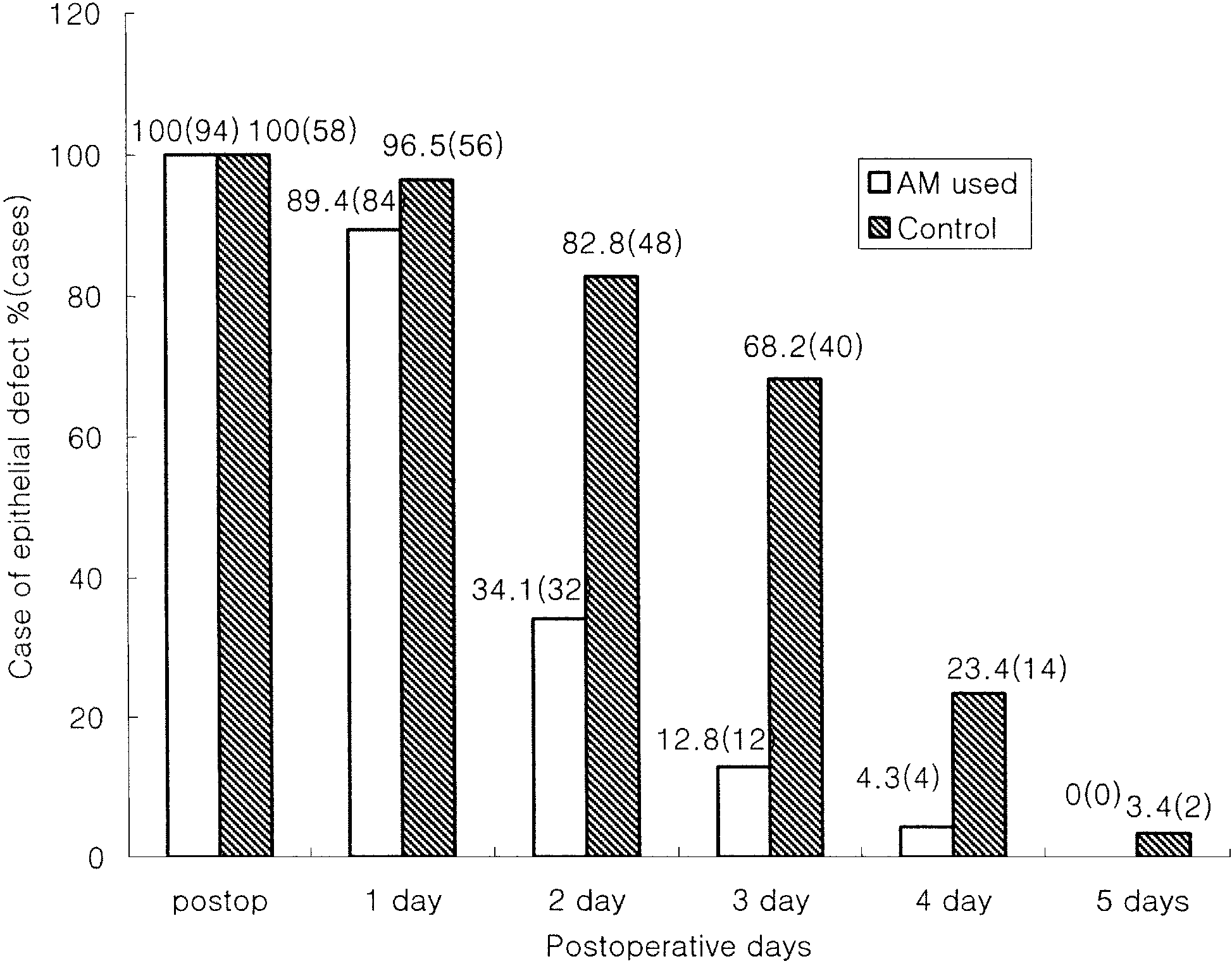 illumination; 1, for an opacity of minimal density seen withdifficulty under direct and diffuse illumination; 2, for an
easily visible opacity; 3, for a dense opacity that significantly
Characteristics
illumination; 1, for an opacity of minimal density seen withdifficulty under direct and diffuse illumination; 2, for an
easily visible opacity; 3, for a dense opacity that significantly
Characteristics