Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
Incorporating fertility preservation into the care of young oncology patients
Incorporating Fertility Preservation Into the Careof Young Oncology Patients
Amanda J. Redig, PhD1; Robert Brannigan, MD2; Steven J. Stryker, MD3,4; Teresa K. Woodruff, PhD4,5; and
As the number of cancer survivors continues to increase, oncologists are faced with the challenge of providing cancer
therapy to patients who may 1 day want to have children. Yet, gonadotoxic cancer treatments can compromise future
fertility, either temporarily or permanently. There are established means of preserving fertility before cancer treat-
ment; specifically, sperm cryopreservation for men and in vitro fertilization and embryo cryopreservation for women.
Several innovative techniques are being actively investigated, including oocyte and ovarian follicle cryopreservation,
ovarian tissue transplantation, and in vitro follicle maturation, which may expand the number of fertility preservation
choices for young cancer patients. Fertility preservation may also require some modification of cancer therapy; thus,
patients’ wishes regarding future fertility and available fertility preservation alternatives should be discussed before
initiation of therapy. This commentary provides an overview of the range of fertility preservation options currently
available and under development, using case-based discussions to illustrate ways in which fertility preservation can
be incorporated into oncology care. Cases involving breast cancer, testicular cancer, and rectal cancer are described
to illustrate fertility issues experienced by male and female patients, as well as to provide examples of strategies for
modifying surgical, medical, and radiation therapy to spare fertility. Current guidelines in oncology and reproductive
medicine are also reviewed to underscore the importance of communicating fertility preservation options to young
patients with cancer. Cancer 2011;117:4–10. V
KEYWORDS: fertility, chemotherapy, radiation therapy, cryopreservation, breast cancer, testicular cancer, colorectalcancer.
Cancer continues to be a leading cause of mortality, yet new and effective therapies have led to an increase in the num-ber of cancer survivors. There are over 10 million cancer survivors in the United States alone.1 Whereas the incidence ofmany cancers increases with age, 1 in 168 Americans will be diagnosed with a malignancy between the ages of 15 and 30.2Greater success in treating cancer brings a new challenge for the oncologist treating younger patients: providing cancertreatment for patients who have a very real possibility of 1 day having children. This requires an expanded perspective onthe potential long-term consequences of the cancer itself as well as the impact of intense and often highly toxic therapy onpatients’ future fertility. To this end, a recent study found patient concerns about future fertility ranked second only toquestions about mortality.3
Ongoing research efforts have led to expanded fertility preservation options for both men and women diagnosed
with cancer, and it is increasingly important for the care offered to younger oncology patients to include discussions aboutfamily planning and fertility preservation. As some approaches to fertility preservation may require modification in thetiming of a patient’s treatment and cannot be implemented once systemic therapy has begun, integration of fertility issuesinto initial discussions about cancer treatment is essential. Multidisciplinary cancer care requires close communicationbetween surgical oncologists, radiation oncologists, and medical oncologists during the development of a treatmentplan.4-6 This structured interaction should enable incorporation of fertility preservation into cancer management. Bybriefly reviewing the advances in fertility preservation for cancer patients and using case studies, this commentary willillustrate how fertility planning can be integrated into oncology practice to enhance the lives of cancer survivors.
Corresponding author: Jacqueline S. Jeruss, MD, PhD, Department of Surgery, Northwestern University Feinberg School of Medicine, 250 East Superior Street,Prentice, 4-420, Chicago, IL 60611; Fax: (312) 503-2555; j-jeruss@northwestern.edu
1Northwestern University Feinberg School of Medicine, Chicago, Illinois; 2Department of Urology, Northwestern University Feinberg School of Medicine, Chicago;3Department of Surgery, Northwestern University Feinberg School of Medicine, Chicago, Illinois; 4Robert H. Lurie Comprehensive Cancer Center, NorthwesternUniversity, Chicago, Illinois; 5Department of Obstetrics and Gynecology, Northwestern University Feinberg School of Medicine, Chicago, Illinois
DOI: 10.1002/cncr.25398, Received: January 22, 2010; Accepted: March 19, 2010, Published online August 31, 2010 in Wiley Online Library(wileyonlinelibrary.com)
Fertility Preservation Cancer Patients/Redig et al
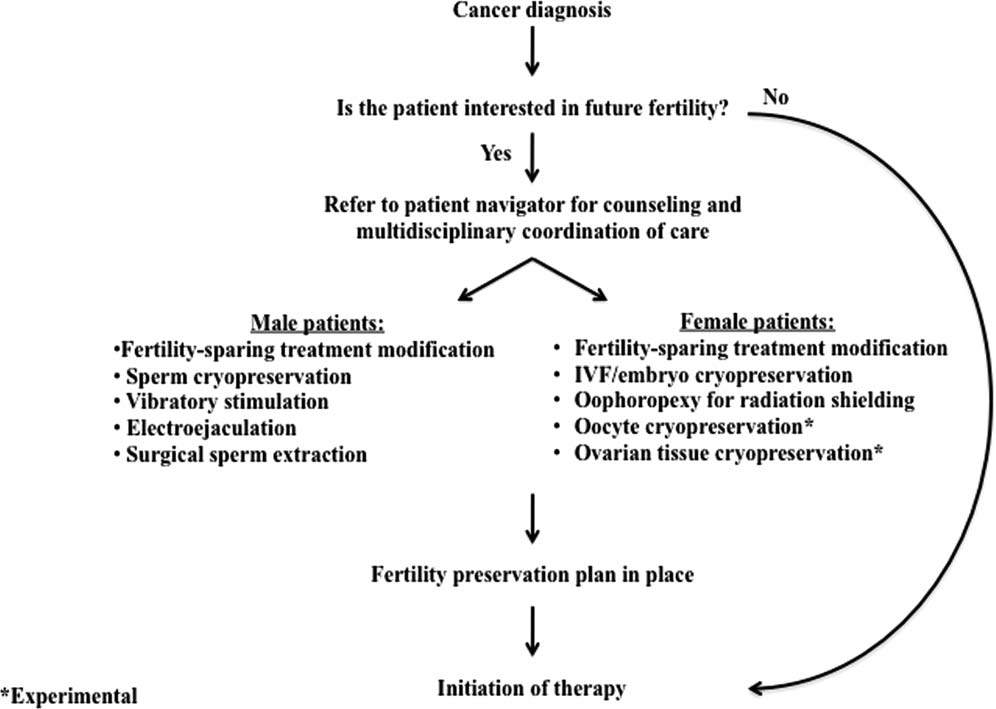
Figure 1. Navigation of the oncofertility treatment path is illustrated. Questions about a young patient’s desire for future fertilitybegin with a cancer diagnosis. If a patient is not interested in fertility preservation, cancer therapy can proceed. However, if apatient is interested in attempting to preserve future fertility, the next steps involve both patient counseling and coordination ofcare. A fertility preservation plan can be tailored to an individual’s circumstances and reflect both established and experimental
options. After a treatment plan incorporates both the need to treat a patient’s disease and their wishes regarding future fertility,the final step is initiation of cancer therapy.
complex decision. While IVF with embryo cryopreserva-
Fertility preservation options can be divided into several
tion remains the option most likely to succeed, ongoing
categories (Fig. 1). First, germ line cells can be preserved
research efforts in artificial reproductive therapy are exam-
directly. In postpubertal male patients, this involves sperm
ining approaches that would expand fertility preservation
banking. For younger pubertal male patients, where col-
options. Technologies are being used to remove ovarian
lection of a semen sample may be more difficult, vibratory
tissue, which contains immature oocytes, and cryopre-
stimulation, electroejaculation, or surgical sperm extrac-
serve strips of cortical tissue or individual follicles before
tion can be attempted.7,8 Currently, no viable options are
therapy.11,14-16 Cortical tissue strips can then be reim-
in place for prepubertal boys, though this is an area of
planted after cancer therapy has concluded, in an attempt
active investigation. For female patients, the most
to restore ovarian function. This approach has resulted in
accepted therapy involves hormonal stimulation, oocyte
6 reported live births for patients who have completed
retrieval, and either oocyte cryopreservation or in vitro
their cancer treatment, with 5 additional births presented
fertilization (IVF), followed by embryo cryopreservation
at a recent meeting of the International Society of Fertility
before initiating therapy.9-12 It is critical that the female
Preservation.14,16-19 However, this technique remains
patient have her baseline fertility assessed before any inter-
experimental and may carry the risk of reintroduction of
vention for fertility preservation, particularly for women
cancer cells upon autotransplantation.15,16,20,21 Labora-
over the age of 35, due to the natural reduction in ovarian
tory efforts for in vitro maturation of cryopreserved
reserve. At this point, over 500 live births have been
immature follicles have shown promise in animal and
achieved using cryopreserved oocytes from young women,
human studies.22-25 Although not yet an option for
yet this technique is still considered experimental.13 IVF,
patients, the ability to cryopreserve immature follicles
while often successful, necessitates that patients without
within ovarian cortical material to mature them at a later
partners choose a sperm donor, which can be a highly
date would facilitate fertility preservation for the youngest
female cancer patients not eligible to undergo assisted
for patients diagnosed during their reproductive
years.38,39 However, any change to standard therapy
In addition to direct germ-line preservation, other
requires discussion between patient and physician on a
strategies can be discussed with younger cancer patients
case-by-case basis. For example, in the setting of colorectal
who desire children. Male patients who are unable to bank
cancer, standard 5-FU therapy does not seem to have dele-
sperm before cancer treatment may consider IVF using a
terious effects on fertility while the use of newer adjuvant
sperm donor. Similarly, for women who do not preserve
agents such as oxaliplatin may introduce more fertility-
embryos or oocytes before cancer treatment, but who main-
threatening side effects.40 Furthermore, the incorporation
tain a functional reproductive tract after therapy, IVF with
of improved diagnostics may provide a more accurate
donor eggs can be used to achieve pregnancy. For those
assessment of patients who are likely to benefit from
patients who cannot carry a pregnancy, use of a gestational
chemotherapy. The recently developed Oncotype DX test
carrier or adoption are also options that can be considered.
may help breast cancer patients and clinicians make deci-sions regarding postsurgery chemotherapy on the basis of
tumor molecular markers and the likelihood of disease
Modification of surgical protocols can also be part of inte-
recurrence.41 Implementation of new diagnostic tools
grating fertility preservation into cancer therapy. For
may allow some younger patients to avoid gonadotoxic
young women with gynecologic malignancies, standard
therapy often involves aggressive surgical resection that
Data suggest that in certain malignancies, including
makes future pregnancies impossible. However, emerging
testicular cancer and Hodgkin disease, compounds pro-
data suggest that less aggressive resection can be used to
duced by the tumor itself can be spermatotoxic before the
successfully treat malignancy while still preserving fertil-
initiation of therapy, resulting in chromosomal aneu-
ity. Conservative management of endometrial carcinoma
ploidy.42 In addition, chromosomal abnormalities in
or ovarian carcinoma with subsequent fertility in young
spermatocytes can be detected up to 24 months after
patients has been reported, while ongoing studies are eval-
chemotherapy.42 Fertility discussions with these patients
uating the clinical efficacy of fertility-sparing conical exci-
should include the possibility that cryopreserved sperm
sions in women with cervical cancer.26-29
may not lead to a viable pregnancy. The role of preim-
Radiation therapy is gonadotoxic in a dose-depend-
plantation genetic diagnosis may also be discussed with
ent manner and has been shown to damage developing
sperm as well as decrease ovarian reserve.30-33 In the caseof gastrointestinal tumors, relative proximity to the repro-
ductive tract is a concern, as radiation used to treat the
Conversations about fertility preservation in cancer
primary tumor may have deleterious secondary effects on
patients are most effective when they occur before initia-
future fertility.34 However, as with other treatment
tion of treatment. Germ line tissue banking for both male
modalities, recognition of this challenge before initiation
and female patients optimally should take place before
of gonadotoxic radiation can help preserve fertility in
any cancer-related surgical resection of reproductive tissue
some patients. Sperm cryopreservation can be offered to
and before initiation of chemotherapy. This is particularly
men, whereas surgical ovarian transposition out of the
relevant for female patients, as the effects of chemotherapy
radiation field and/or oocyte or embryo preservation are
become more pronounced as a woman nears meno-
options for women undergoing pelvic radiation.34
pause.43,44 The more subtle challenge facing oncologists is
As more data emerge regarding the threat to fertility
determining in which patients and for how long standard
posed by specific pharmacological agents, chemotherapy
therapy can be delayed to accommodate fertility preserva-
protocols may be modified to avoid potentially gonado-
tion. It has been proposed that women with breast cancer
toxic side effects in young patients. Chemotherapeutic
can delay treatment for up to 1 month to initiate hormo-
agents targeting rapidly dividing cells are damaging to
nal stimulation and oocyte retrieval for either oocyte or
germ cells, with alkylating agents having particularly toxic
embryo cryopreservation.8,11,45,46 There is also some evi-
effects on ovarian tissue.33,35-37 Studies in patients with
dence suggesting that breast cancer patients who will ulti-
urological tumors or breast cancer suggest the feasibility
mately undergo a course of tamoxifen treatment can delay
of treatment modification to help minimize reproductive
this antihormonal therapy until after a pregnancy.47
tract toxicity; these modified regimens may be preferable
Although estrogen receptor-positive tumors are hormo-
Fertility Preservation Cancer Patients/Redig et al
nally driven, there is no evidence directly linking preg-
scrotal ultrasound revealed a 3-cm heterogeneous left tes-
nancy after breast cancer with an increased incidence of
ticular lesion, prompting a referral to a urologist. Repeat
physical examination confirmed the presence of anindurated, nontender, left testicular mass. Serum tumor
marker levels revealed normal alpha-fetoprotein, beta-
As demonstrated by the series of case discussions that fol-
hCG, and LDH levels. At that time, the patient was coun-
low, incorporating fertility preservation into cancer care
seled regarding treatment options, and a recommendation
requires flexibility on a case-by-case basis to consider a
was made for left radical orchiectomy. In addition, he was
patient’s wishes as well as the optimal course of therapy
encouraged to undergo sperm cryopreservation before sur-
gery. He agreed to pursue each of these procedures. Thepatient noted upon questioning that he was engaged and
that he and his fiancee had been trying to achieve a preg-
A 34-year-old woman presented with an isolated
nancy for 1 year without success. He also reported that his
4-cm, firm, left breast mass. After visualization by ultra-
fiancee had recently seen a reproductive endocrinologist
sound and mammogram, core biopsy was performed,
for evaluation of her reproductive health. The oncofertil-
which demonstrated estrogen and progesterone receptor-
ity patient navigator was contacted, and she helped
negative and HER2 negative infiltrating ductal carci-
arrange semen analysis testing with concurrent sperm cry-
noma. Treatment planning was discussed with the patient
opreservation. The patient provided 2 separate semen
and included timing of chemotherapy, lumpectomy ver-
samples for cryopreservation, each with an appropriate
sus mastectomy, and the use of radiation therapy. The
duration of 2-3 days of preceding abstinence. Both semen
patient opted for primary surgery with lumpectomy, fol-
analyses revealed normal ejaculate volume, severely low
lowed by chemotherapy and radiation. Fertility preserva-
sperm concentration (<100,000 sperm per mL), a moder-
tion was also discussed, and the patient, who was single
ately low percentage of sperm with motility, and a moder-
and had no children, stated that she would want to pursue
ately low percentage of sperm with normal morphology.
as many options as possible to try to have a child after her
A total of 6 vials of sperm were cryopreserved, and a test
treatment. After meeting with the surgical oncologist, thepatient met with an oncofertility patient navigator, and
thaw revealed that 25% of the sperm had progressive mo-
her case was discussed with the multidisciplinary oncofer-
tility post-thaw. The patient’s case was subsequently pre-
tility team that included the patient’s oncologists, a repro-
sented at the multidisciplinary oncofertility grand rounds,
ductive endocrinology infertility specialist, and the
attended by his urologist, his fiancee’s reproductive endo-
patient navigator. The patient then met with the repro-
crinologist, and the oncofertility patient navigator. A rec-
ductive endocrinology infertility specialist who discussed
ommendation was made for the couple to undergo IVF
fertility preservation options, including embryo cryopre-
with intracytoplasmic sperm injection (ICSI), given the
servation, oocyte cryopreservation, and ovarian tissue cry-
severe male factor infertility present.
opreservation. The patient opted for embryo and oocyte
The patient underwent left radical orchiectomy,
cryopreservation, and oral contraceptives were started im-
revealing a nonseminomatous mixed germ cell tumor.
mediately in preparation for oocyte retrieval after surgery.
Postoperative imaging revealed a normal chest x-ray and
On final pathology, all lymph nodes and margins were
no evidence of retroperitoneal lymphadenopathy, consist-
noted to be free of tumor cells. During her 4-week recov-
ent with clinical stage I disease. After meeting with a med-
ery from surgery, the patient underwent successful ovarian
ical oncologist and discussing treatment options, the
stimulation and oocyte harvest, which resulted in the cry-
patient opted for primary platinum-based chemotherapy
opreservation of several oocytes and 4 embryos using an
consisting of 2 cycles of bleomycin, etoposide, and cispla-
anonymous sperm donor. The patient subsequently began
tin. Upon completion of chemotherapy, he underwent se-
adjuvant chemotherapy to be followed by radiation, and
rial semen testing every 6 months for 2 years. Each semen
she intends to pursue a pregnancy in the future with her
analysis showed normal ejaculate volume with azoosper-
mia. Two years after completion of chemotherapy, thecouple underwent IVF/ICSI using his cryopreserved
Fertility preservation and testicular cancer
sperm, and a singleton pregnancy resulted.
A 28-year-old single male presented to his internist
This case accentuates several important points. First,
for evaluation of a painless, firm, left testicular lump. A
men affected by cancer may not initially volunteer their
efforts to achieve a pregnancy or express their desire for
yet become pregnant, although her periods have returned.
future paternity. It is imperative that the urologist or
The patient and her husband are now discussing the possi-
oncologist discuss the potential effects of cancer and can-
bility of working with a reproductive endocrinologist to
cer therapy with the patient, preferably before initiation
attempt a pregnancy using their cryopreserved embryos. If
of treatment. Second, many males diagnosed with cancer
the patient’s uterus is determined to be too fibrotic postra-
present concurrently with impaired semen parameters.
diation to sustain a pregnancy, they have decided not to
These changes may derive from a variety of factors,
pursue the use of a surrogate and may instead investigate
including fever, cytological immune response, hypogo-
nadism, and congenital or acquired testicular abnormal-ities. Finally, surgical therapy and chemotherapy may
result in persistent azoospermia, further highlighting the
Each of the above cases illustrates the means by which fer-
importance of offering sperm cryopreservation before
tility preservation can be integrated into the care of cancer
patients. In all cases, the success of such measures dependsupon early and open communication with patients, flexi-
bility in scheduling appointments and procedures for
A 38-year-old woman with a history of hemorrhoids
both cancer care and fertility preservation, and the pres-
noticed bright red blood in her stool for 6 months. When
ence of a multidisciplinary oncofertility team that can see
the bleeding did not stop and became associated with ab-
patients and discuss their cases on short notice. Current
dominal pain and intermittent constipation, she under-
guidelines issued by the professional bodies representing
went a colonoscopy which revealed a suspicious mass in
both oncologists and fertility specialists underscore the
the rectum. Biopsy results demonstrated high-grade ade-
importance of clear discussion regarding available inter-
nocarcinoma, and a CT scan of the chest, abdomen, and
ventions.51,52 The 2005 report of the ethics committee of
pelvis indicated disease had spread to some local lymph
the American Society of Reproductive Medicine (ASRM)
nodes. No evidence of disease was seen in other organs. At
states that physicians should inform cancer patients about
the time of diagnosis, the patient had a 3-year-old daugh-
options for fertility preservation—recognizing that, to
ter, and she and her husband had been trying to conceive
date, the only established techniques for doing so include
sperm or embryo cryopreservation. The ASRM guidelines
Treatment for stage III rectal cancer involves surgery
further emphasize that experimental techniques, includ-
as well as preoperative chemotherapy and radiation to the
ing oocyte or ovarian tissue cryopreservation, should be
pelvis. In this case, pelvic radiation was the most signifi-
conducted with the oversight of an Institutional Review
cant threat to future fertility, and options, including pre-
Board.51 In 2006, the American Society of Clinical On-
treatment oophoropexy to move the ovaries away from
cology (ASCO) Recommendations on Fertility Preserva-
the site of maximum radiation, were discussed with the
tion in Cancer Patients were published.52 Key to these
patient and her husband. In addition, the decision was
guidelines was an awareness that cancer patients are inter-
made to use a 5-FU-based chemotherapy regimen instead
ested in information regarding fertility, and that early
of the more gonadotoxic oxaliplatin. After meeting with
intervention and discussion are critical to ensure future
her surgeon, the patient was referred to the oncofertility
reproductive success. Similar to the ASRM report, these
team, where additional options for oocyte or embryo cry-
recommendations also identify sperm and embryo cryo-
opreservation were also discussed. The patient opted for
preservation as the options known to be most successful.
oocyte retrieval and embryo cryopreservation before her
As greater numbers of young cancer patients are suc-
scheduled oophoropexy and subsequent neoadjuvant
cessfully treated, it is increasingly important for the medical
chemotherapy and radiation. Dosimetry was specified to
community to address the long-term needs of the cancer
minimize exposure of the uterus and ovaries to radiation.
survivor. The oncologist has the greatest ability to initiate
At the time of surgery, 8 weeks after chemoradiation, a
conversations about disease management, treatment
22-cm section of distal colon and rectum were removed,
options, and issues related to life after cancer; thus, it is
and margins were declared free of tumor. Thirteen meso-
essential that oncologists become familiar with the growing
rectal lymph nodes showed no evidence of residual cancer,
field of fertility preservation. Not only can several distinct
and the patient recovered without complications. To date,
options be discussed with patients and incorporated into
18 months after the completion of therapy, she has not
the multidisciplinary steps of cancer treatment, but doing
Fertility Preservation Cancer Patients/Redig et al
so can also immeasurably enrich patients’ lives as cancer
11. Agarwal SK, Chang RJ. Fertility management for women
survivors. To facilitate this goal, the Oncofertility Consor-
with cancer. Cancer Treat Res. 2007;138:15-27.
12. Anderson RA, Wallace WH, Baird DT. Ovarian cryopreser-
tium has been established as a multidisciplinary and multi-
vation for fertility preservation: indications and outcomes.
institution research collaboration specifically focused on
the research efforts, clinical practice, and social and ethical
13. Porcu E, Bazzocchi A, Notarangelo L, Paradisi R, Landolfo
C, Venturoli S. Human oocyte cryopreservation in infertility
implications raised by fertility preservation in cancer
and oncology. Curr Opin Endocrinol Diabetes Obes.
patients.43 A recent analysis of several qualitative studies
with adult and pediatric oncologists suggests that, despite
14. Donnez J, Dolmans MM, Demylle D, et al. Livebirth after
the ASCO/ASRM guidelines, many oncologists do not dis-
orthotopic transplantation of cryopreserved ovarian tissue. Lancet. 2004;364:1405-1410.
cuss fertility preservation with cancer patients.53 Several
15. Demeestere I, Simon P, Emiliani S, Delbaere A, Englert Y.
factors have been identified to account for this discrepancy,
Orthotopic and heterotopic ovarian tissue transplantation.
including lack of knowledge, uncertainty about the success
16. Meirow D, Levron J, Eldar-Geva T, et al. Pregnancy after
of fertility preservation methods, and language/cultural
transplantation of cryopreserved ovarian tissue in a patient
barriers. As cancer care moves into the 21st century, it is
with ovarian failure after chemotherapy. N Engl J Med.
our hope that available options for fertility preservation
17. Demeestere I, Simon P, Buxant F, et al. Ovarian function
will continue to expand and become part of the conversa-
and spontaneous pregnancy after combined heterotopic and
tion between every oncologist and their young patients.
orthotopic cryopreserved ovarian tissue transplantation in apatient previously treated with bone marrow transplantation:case report. Hum Reprod. 2006;21:2010-204.
18. Andersen CY, Rosendahl M, Byskov AG, et al. Two suc-
Supported by a National Institutes of Health predoctoral fellow-
cessful pregnancies following autotransplantation of frozen/
ship F30ES015668 (to A.J.R.) and by National Institutes of
thawed ovarian tissue. Hum Reprod. 2008;23:2266-2272.
19. Donnez J, Jadoul P, Squifflet J, et al. Ovarian tissue cryo-
preservation and transplantation in cancer patients. BestPract Res Clin Obstet Gynaecol. 2009;24:87-100.
20. Meirow D, Levron J, Eldar-Geva T, et al. Monitoring the
ovaries after autotransplantation of cryopreserved ovarian tis-
1. Ries LA, Harkins D, Krapcho M, et al. SEER Cancer Statis-
sue: endocrine studies, in vitro fertilization cycles, and live
tics Review, 1975–2003. Bethesda, MD: National Cancer
birth. Fertil Steril. 2007;87:418 e7-418 e15.
21. Meirow D, Hardan I, Dor J, et al. Searching for evidence
2. Bleyer A. Young adult oncology: the patients and their sur-
of disease and malignant cell contamination in ovarian tissue
vival challenges. CA Cancer J Clin. 2007;57:242-255.
stored from hematologic cancer patients. Hum Reprod.
3. Loscalzo MJ, Clark KL. The psychosocial context of cancer-
related infertility. Cancer Treat Res. 2007;138:180-190.
22. Xu M, Kreeger PK, Shea LD, Woodruff TK. Tissue-engi-
4. Guarneri V, Conte P. Metastatic breast cancer: therapeutic
neered follicles produce live, fertile offspring. Tissue Eng.
options according to molecular subtypes and prior adjuvant
therapy. Oncologist. 2009;14:645-656.
23. Telfer EE, McLaughlin M, Ding C, Thong KJ. A 2-step se-
5. Bengala C, Bettelli S, Bertolini F, et al. Epidermal growth
rum-free culture system supports development of human
factor receptor gene copy number, K-ras mutation and path-
oocytes from primordial follicles in the presence of activin.
ological response to preoperative cetuximab, 5-FU and radi-
ation therapy in locally advanced rectal cancer. Ann Oncol.
24. Xu M, Barrett SL, West-Farrell E, et al. In vitro grown
human ovarian follicles from cancer patients support oocyte
6. You DD, Lee HG, Heo JS, Choi SH, Choi DW. Prognos-
growth. Hum Reprod. 2009;24:2531-2540.
tic factors and adjuvant chemoradiation therapy after pan-
25. Jin SY, Lei L, Shikanov A, Shea LD, Woodruff TK. A novel
creaticoduodenectomy for pancreatic adenocarcinoma. J
2-step strategy for in vitro culture of early-stage ovarian fol-
Gastrointest Surg. 2009;13:1699-1706.
licles in the mouse. Fertil Steril. 2009;93:2633-2639.
7. Schmiegelow ML, Sommer P, Carlsen E, Sonksen JO,
26. Mazzon I, Corrado G, Masciullo V, Morricone D, Ferran-
Schmiegelow K, Muller JR. Penile vibratory stimulation and
dina G, Scambia G. Conservative surgical management of
electroejaculation before anticancer therapy in 2 pubertal
stage IA endometrial carcinoma for fertility preservation.
boys. J Pediatr Hematol Oncol. 1998;20:429-430.
8. Jeruss JS, Woodruff TK. Preservation of fertility in patients
27. Wright JD, Shah M, Mathew L, et al. Fertility preservation
with cancer. N Engl J Med. 2009;360:902-911.
in young women with epithelial ovarian cancer. Cancer.
9. West ER, Zelinski MB, Kondapalli LA, et al. Preserving
female fertility following cancer treatment: current options and
28. Park JY, Kim DY, Kim JH, Kim YM, Kim YT, Nam JH. Sur-
future possibilities. Pediatr Blood Cancer. 2009;53:289-295.
gical management of borderline ovarian tumors: The role of
10. Lee D. Ovarian tissue cryopreservation, transplantation:
fertility-sparing surgery. Gynecol Oncol. 2009;113:75-82.
banking reproductive potential for the future. Cancer Treat
29. Fambrini M, Penna C, Pieralli A, et al. CO2 laser cylindri-
cal excision or standard re-conization for persistent-recurrent
high-grade cervical intraepithelial neoplasia (HG-CIN) in
41. Paik S, Shak S, Tang G, et al. A multigene assay to predict
women of fertile age. Anticancer Res. 2008;28:3871-3875.
recurrence of tamoxifen-treated, node-negative breast cancer.
30. Nalesnik JG, Sabanegh ES, Jr, Eng TY, Buchholz TA. Fer-
tility in men after treatment for stage 1 and 2A seminoma.
42. Tempest HG, Ko E, Chan P, Robaire B, Rademaker A,
Martin RH. Sperm aneuploidy frequencies analysed before
31. Sieniawski M, Reineke T, Nogova L, et al. Fertility in male
and after chemotherapy in testicular cancer and Hodgkin’s
patients with advanced Hodgkin lymphoma treated with
lymphoma patients. Hum Reprod. 2008;23:251-258.
BEACOPP: a report of the German Hodgkin Study Group
43. Backhus LE, Kondapalli LA, Chang RJ, Coutifaris C, Kazer
R, Woodruff TK. Oncofertility consortium consensus state-
32. Lie Fong S, Laven JS, Hakvoort-Cammel FG, et al. Assessment
ment: guidelines for ovarian tissue cryopreservation. Cancer
of ovarian reserve in adult childhood cancer survivors using
anti-Mullerian hormone. Hum Reprod. 2009;24:982-990.
44. Burstein HJ, Winer EP. Primary care for survivors of breast
33. Larsen EC, Muller J, Schmiegelow K, Rechnitzer C, Ander-
cancer. N Engl J Med. 2000;343:1086-1094.
sen AN. Reduced ovarian function in long-term survivors
45. West ER, Zelinski MB, Kondapalli LA, et al. Preserving
of radiation- and chemotherapy-treated childhood cancer.
female fertility following cancer treatment: current options
J Clin Endocrinol Metab. 2003;88:5307-5314.
and future possibilities. Pediatr Blood Cancer. 2009;53:289-
34. Elizur SE, Tulandi T, Meterissian S, Huang JY, Levin D,
Tan SL. Fertility preservation for young women with rectal
46. Falcone T, Attaran M, Bedaiwy MA, Goldberg JM. Ovarian
cancer—a combined approach from 1 referral center. J Gas-
function preservation in the cancer patient. Fertil Steril.
35. Arnon J, Meirow D, Lewis-Roness H, Ornoy A. Genetic
47. Gradishar WJ, Hellmund R. A rationale for the reinitiation
and teratogenic effects of cancer treatments on gametes and
of adjuvant tamoxifen therapy in women receiving fewer
embryos. Hum Reprod Update. 2001;7:394-403.
than 5 years of therapy. Clin Breast Cancer. 2002;2:282-
36. Nurmio M, Keros V, Lahteenmaki P, Salmi T, Kallajoki M,
Jahnukainen K. Effect of childhood acute lymphoblastic leu-
48. Blakely LJ, Buzdar AU, Lozada JA, et al. Effects of preg-
kemia therapy on spermatogonia populations and future fer-
nancy after treatment for breast carcinoma on survival and
tility. J Clin Endocrinol Metab. 2009;94:2119-2122.
risk of recurrence. Cancer. 2004;100:465-469.
37. Oktem O, Oktay K. Quantitative assessment of the impact
49. Ives A, Saunders C, Bulsara M, Semmens J. Pregnancy after
of chemotherapy on ovarian follicle reserve and stromal
breast cancer: population based study. BMJ. 2007;334:194.
function. Cancer. 2007;110:2222-2229.
50. Gupta PB, Kuperwasser C. Contributions of estrogen to
38. Pectasides D, Pectasides E, Papaxoinis G, et al. Testicular
ER-negative breast tumor growth. J Steroid Biochem Mol
function in poor-risk nonseminomatous germ cell tumors
treated with methotrexate, paclitaxel, ifosfamide, and cispla-
51. Ethics Committee of the American Society for Reproductive
tin combination chemotherapy. J Androl. 2009;30:280-286.
Medicine. Fertility preservation and reproduction in cancer
39. Zekri JM, El-Helw LM, Purohit OP, Hatton MQ, Cole-
patients. Fertil Steril. 2005;83:1622-1628.
man RE. Epirubicin/vinorelbine adjuvant chemotherapy in
52. Lee SJ, Schover LR, Partridge AH, et al. American Society
young women with breast cancer is associated with preserva-
of Clinical Oncology recommendations on fertility preserva-
tion of menstrual function. Clin Oncol (R Coll Radiol).
tion in cancer patients. J Clin Oncol. 2006;24:2917-2931.
53. Quinn GP, Vadaparampil ST, King L, Miree CA, et al.
40. Spanos CP, Mamopoulos A, Tsapas A, Syrakos T, Kiskinis
Impact of physicians’ personal discomfort and patient prog-
D. Female fertility and colorectal cancer. Int J Colorectal
nosis on discussion of fertility preservation with young can-
cer patients. Patient Educ Couns. 2009;77:338-343.
“REGULATED RENTS” IN PRIVATE BUILDINGS Type of proceedings: Composition of Tribunal: Dissenting opinion: Initiator: Supreme Court – Administrative, Labour Legal provisions under review Basis of review Transitional application of provisions concerning regulated rents determined by commune councils at a level not exceeding 3% of the reconstruction value of living
QUESTIONS AND ANSWERS ON THE REVIEW OF PROZAC FOR USE IN CHILDREN AND ADOLESCENTS The Committee for Medicinal Products for Human Use (CHMP) has completed its arbitration review of Prozac (fluoxetine) and associated namesextend its use in the treatment of children suffering from depression, provided that the marketing authorisation holder (MAH), Eli Lilly, carries out additional studie
 Fertility Preservation Cancer Patients/Redig et al
Figure 1. Navigation of the oncofertility treatment path is illustrated. Questions about a young patient’s desire for future fertilitybegin with a cancer diagnosis. If a patient is not interested in fertility preservation, cancer therapy can proceed. However, if apatient is interested in attempting to preserve future fertility, the next steps involve both patient counseling and coordination ofcare. A fertility preservation plan can be tailored to an individual’s circumstances and reflect both established and experimental
options. After a treatment plan incorporates both the need to treat a patient’s disease and their wishes regarding future fertility,the final step is initiation of cancer therapy.
Fertility Preservation Cancer Patients/Redig et al
Figure 1. Navigation of the oncofertility treatment path is illustrated. Questions about a young patient’s desire for future fertilitybegin with a cancer diagnosis. If a patient is not interested in fertility preservation, cancer therapy can proceed. However, if apatient is interested in attempting to preserve future fertility, the next steps involve both patient counseling and coordination ofcare. A fertility preservation plan can be tailored to an individual’s circumstances and reflect both established and experimental
options. After a treatment plan incorporates both the need to treat a patient’s disease and their wishes regarding future fertility,the final step is initiation of cancer therapy.