Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
Bodyfocushealthgroup.com.au
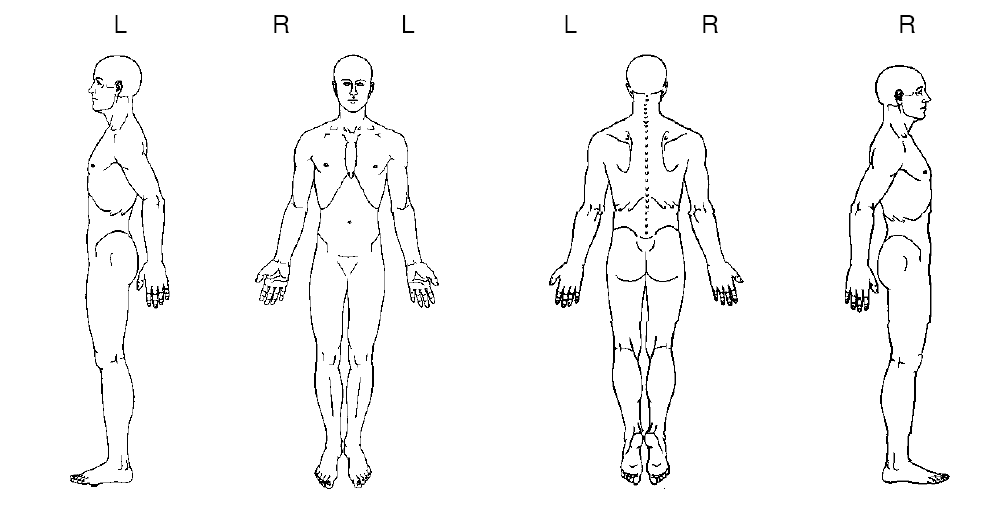
CONFIDENTIAL PATIENT CASE HISTORY As a multidisciplinary practice providing comprehensive care, we focus on your ability to be healthy. Our goals are: firstly, to address the issues that brought you to this practice; secondly, to treat the cause of your condition (not just treat the symptoms or place a temporary patch over your condition); and thirdly, to offer you the opportunity of improved health potential and wellness services in the future. Answering the following questions will give us a profile of your health, and ensure that we optimise your outcome and deliver treatment excellence. What is your major complaint? _________________________________________________________________ Draw on the sketch below the area(s) where you feel your problem to be.
When did your symptoms start? _________________________________________________________________ Was it a gradual or sudden onset? _________________________________________________________________ Have you had this or a similar problem in the past? _________________________________________________________________ If you are experiencing pain, please tick the words that best describe your pain:
Confidential Patient Case History Form Version 1.0,
Do you get?
needles Since the problem started it is:
About the same Getting better Getting worse
What makes your pain worse? Your pain interferes with: What type of work do you do? __________________________________________________________ Any Bladder or Bowel changes since this episode started? __________________________________________________________ Do you experience any nausea, dizziness, difficulty swallowing, changes in vision, or fainting spells, fever, skin rashes associated with your symptoms? __________________________________________________________ Other health professionals seen for this problem (please list): Medical Doctor____________________________________________________________ Specialist Doctor/Surgeon_____________________________________________________ Physiotherapist/Chiropractor __________________________________________________________________ Other __________________________________________________________________ List any medications you are taking __________________________________________________________________ __________________________________________________________________ __________________________________________________________________ __________________________________________________________________ Have you ever taken oral cortisone or prednisone (including asthma medications such as pulmicort, symbicort, flixotide & seretide)? Y/N Are you pregnant? Y/N
Confidential Patient Case History Form Version 1.0,
Do you have or have you ever had?: (please tick)
High blood pressure
Patient’s Signature: _______________ Print Name: ______________________ Practitioner's Signature: _________________ Date: _____________________
Confidential Patient Case History Form Version 1.0,
Max GXL Ingredients Serving Size – 3 capsules (56 servings per box) – take 1 pkg in the am, one in the pm – comments next to the ingredients are those of a friend who likes to analyze this Amount per serving Vitamin C (as Calcium Ascorbate) – 250mg N-Acetyl Cysteine – 375mg L-glutamine – 750mg N-Acetyl D-Glucosamine – 125mg Quercetin – 37.5mg
Joseane AmesI,II Falsifi cação de medicamentos Daniele Zago SouzaIII no Brasil Counterfeiting of drugs in Brazil OBJETIVO: Identifi car os principais medicamentos falsifi cados apreendidos pela Polícia Federal brasileira e os estados em que houve a apreensão. MÉTODOS: Estudo retrospectivo descritivo dos laudos periciais elaborados por Peritos Criminais da Polícia Feder

 CONFIDENTIAL PATIENT CASE HISTORY
CONFIDENTIAL PATIENT CASE HISTORY 
 Do you have or have you ever had?: (please tick)
Do you have or have you ever had?: (please tick)