Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
10 1.9999
Journal of Thrombosis and Haemostasis, 1: 171–177
Protective effects of vitamin C on endothelium damageand platelet activation during myocardial infarctionin patients with sustained generation ofcirculating microparticles
O . M O R E L , Ãy L . J E S E L , à B . H U G E L , yz M - P D O U C H E T , à M . Z U P A N , à M . C H A U V I N , à J - M F R E Y S S I N E T yz andF . T O T I yz§ÃFe´de´ration de Cardiologie des Hoˆpitaux Universitaires de Strasbourg, France; yInstitut d’He´matologie et d’Immunologie, Universite´ Louis Pasteur,Strasbourg, France; zU. 143 INSERM, Le Kremlin-Biceˆtre; and §Faculte´ de Me´decine Paris-Sud, Le Kremlin-Biceˆtre, France
thrombin generation [5]. Their procoagulant potential relies on
Summary. During myocardial infarction (MI), high levels of
phosphatidylserine (PhtdSer), an aminophospholipid translo-
circulating procoagulant microparticles (MP) shed from endo-
cated to the external membrane leaflet, and on the possible
thelial cells and platelets diffuse prothrombotic and proinflam-
presence of membrane tissue factor (TF), the major cellular
matory potentials crucial for the coronary prognosis. In addition
activator, expressed by smooth muscle cells, fibroblasts, mono-
to conventional treatments, we evaluated whether vitamin C
cytes and activated endothelial cells. High amounts of circulat-
treatment could modify circulating levels of procoagulant MP.
ing procoagulant MP, shed mainly from platelets and
Upon admission, 61 patients with MI were prospectively ran-
endothelial cells, are detected during acute coronary syndrome
domized for immediate additional vitamin C treatment. Circu-
[6] and may influence the coronary prognosis [7].
lating MP were quantified by functional prothrombinase assay
Oxidative stress may account for a significant proportion in
before and after 5 days of vitamin C administration (1 g dayÀ1).
endothelium dysfunction and platelet activation observed in
The cellular origin of MP was also assessed. In vitamin C-
atherogenesis [8–12]. Evidence suggests that the antioxidant
treated patients, the reduction in platelet-derived MP was 10%
status is linked to the clinical expression of coronary artery
higher (P ¼ 0.01). In patients with diabetes mellitus, dyslipi-
disease [13]. Indeed, low vitamin C serum concentrations are
demia or more than two cardiovascular risk factors, vitamin C
associated with inflammation and severity of the illness [14,15].
decreased endothelial and platelet-derived MP levels by $70%
Therefore, additional antioxidant treatments were proposed to
and 13%, respectively. This early effect on circulating platelet
reduce both platelet activation and endothelial dysfunction
and endothelial-derived MP, testifies to the importance of
during atherogenesis [16]. In various experimental models,
oxidative stress during MI. Vitamin C could prove beneficial
antioxidants were found to be beneficial on vasospasm, neoin-
for the outcome of patients at higher thrombotic risk.
timal thickening or remodeling after balloon injury [17]. Ac-cordingly, antioxidant vitamin C treatment was shown to
Keywords: atherosclerosis; oxidative stress; thrombosis.
improve endothelial function in several subsets of patientsincluding hypercholesterolemia, coronary artery disease andheart transplantation vasculopathy [18–22].
In this study, we examined whether additional treatment by
vitamin C may reduce circulating procoagulant MP as a marker
Membrane microparticles (MP) are shed from stimulated and/or
of vascular damage and platelet activation in the peripheral
apoptotic vascular cells and released in blood flow. They bear
blood of patients with myocardial infarction (MI). The cell
membrane glycoproteins testifying to their cell origin and their
origin of MP was also assessed to detect a possible subset of
amount was found to be correlated to the degree of apoptosis
cells more responsive to vitamin C treatment. MP were isolated
[1]. Elevated levels of circulating MP have been reported in a
from plasma samples by capture onto immobilized annexin V, a
variety of pathologies [1–4]. In the blood flow, circulating MP
protein with high affinity for PhtdSer. MP measurements and
provide an additional procoagulant phospholipid surface neces-
characterization were performed using a modified prothrombi-
sary for the assembly of the clotting enzymes complexes and
nase assay [4]. Effects of vitamin C were examined with respectto various cardiovascular risk factors.
Correspondence: F. Toti, Institut d’He´matologie et d’Immunologie, Faculte´
de Me´decine, 4, rue Kirschleger 67085 Strasbourg cedex, France.
Tel.: þ 33 03 9024 3986; fax: þ 33 03 9024 4016;
e-mail: florence.toti@hemato-ulp.u-strasbg.fr
Sixty-one patients presenting an acute myocardial infarction
Received 18 April 2002, revised 11 July 2002, accepted 13 July 2002
were enrolled in the study. Typical chest pain, persistent
# 2003 International Society on Thrombosis and Haemostasis
ST–segment elevation on electrocardiogram, and a two-fold
streptavidin-coated microtitration plates and Chromozym TH
rise in creatine phosphokinase (CPK) diagnosed MI. All pati-
were from Roche Diagnostics (Mannheim, Germany).
ents received conventional treatment including beta-blockers,aspirin (160–325 mg dayÀ1) before blood sampling. An addi-
Isolation of circulating MP and determination of their
tional weight-adjusted unfractionated heparin regimen was
applied (initial bolus 50 units kgÀ1) to achieve an activatedpartial thromboplastin time between 60 and 90 s. Patients were
Blood samples, collected by venous puncture, were collected on
prospectively randomized to receive an additional 5 days’ vitamin
138 mmol LÀ1 citrated solution (9 volumes of blood : 1 volume of
C oral treatment (1 g dayÀ1) or placebo tablets (29 and 32 patients,
anticoagulant) before vitamin C therapy [day (D)1] and 5 days
respectively). 76% of the patients treated by vitamin C and 75% of
later (D5). Platelet-free plasma samples (PFP) containing circu-
the patients with placebo were submitted to primary angioplasty.
lating MP were obtained by double centrifugation as previously
Statins, anti-ischemic medications and anti-platelet inhibitors
described [1]. MP were captured onto insolubilized annexin Vand
were equally prescribed. The opportunity of angioplasty, stent
their PhtdSer content was determined by functional prothrombi-
placement and additional anti-GPIIbIIIa therapy (abciximab or
nase assay using a microplate reader equipped with kinetics
eptifibatide) was under the responsibility of independent angio-
software. In this assay, blood clotting factors (FXa, FVa, FII)
plasty physicians. Vitamin C was given just at the end of anti-
and calcium concentrations were determined to ensure that
GPIIbIIIa treatment. This treatment consisted of one bolus of
PhtdSer is the rate-limiting parameter in the generation of soluble
250 mg kgÀ1 followed by 0.125 mg kgÀ1 minÀ1 continuous infu-
thrombin from prothrombin. In this purified system, the presence
sion up to 18 h for abciximab and one bolus of 180 mg kgÀ1
of TF on captured MP does not alter values corresponding to
followed by initiation of 2 mg kgÀ1 minÀ1 continuous infusion
PhtdSercontent, and FVawasinexcess with respect to FXa in order
up to 18 h for eptifibatide. Patients with diabetes mellitus (DM)
to exclude any contribution of FVa, possibly associated with MP.
were recruited on the basis of documented medical reports, if
Results were expressed as nanomolar PhtdSer equivalent (nmol
treated by insulin or oral hypoglycaemic agents, or when
LÀ1 PhtdSer Eq) by reference to a standard curve constructed with
elevated levels of fasting blood glucose (> 140 mg dLÀ1) were
liposomes of known composition and concentration [1].
measured on at least two separate occasions. Dyslipidemicpatients (DL) were identified on the basis of medical history,
Search for the cellular origin of circulating MP
ongoing treatment by statins or fibrates, or high levels of totalor LDL cholesterol measured during their stay. Other cardio-
Biotinylated monoclonal antibodies to various cell types (anti-
vascular risk factors considered were arterial hypertension,
CD31 for endothelial cells, anti-GPIb for platelets) were inso-
current smoking, increase weight (body mass index >29 kg
lubilized onto streptavidin-coated microtitration plates as pre-
mÀ2). For comparative purpose, 23 patients with less than two
viously described [4]. CD31 being also expressed to a small
cardiovascular risk factors were defined as low-risk patients
extent on platelets, it was previously ensured that circulating
(referred to as LR in the text) regardless of the occurrence
MP bearing CD31 ([CD31]þ MP) mainly originate from apop-
of DM or DL. Thirty-eight patients with more than two cardi-
totic endothelial cells and are therefore a reliable marker of
ovascular risk factors, including DM and DL, were defined
endothelial damage [7,23]. After incubation of PFP and wash-
as high-risk patients (referred to as HR in the text). Fifty heal-
ing, captured MP were quantified by prothrombinase assay as
thy volunteers (HV) were simultaneously investigated du-
described above. Background values obtained with correspond-
ring the inclusion period as a reference group. Written
ing irrelevant IgGs were subtracted. It should be emphasized
informed consent was obtained from all the patients with the
that no direct comparison between capture by annexin V and
approval of local Ethical Committee (Comite´ Consultatif de
antibodies could be performed because affinities for the respec-
Protection des Personnes dans la Recherche Biome´dicale,
tive counterpart ligands are different.
Results are expressed as mean Æ SEM from at least two
Monoclonal antibody (mAb) to human platelet glycoprotein
independent measurements. Patients groups were compared
GPIb was a kind gift of Dr F. Lanza, biotinylated as described
using a Mann–Whitney test. A P-value <0.05 was considered
elsewhere [4]. Biotinylated mAb to CD31 was from CALTAG
Laboratories (Burlingame, CA, USA), and the irrelevant cor-responding biotinylated immunoglobulins were from Leinco
Technologies (Ballwin, MO, USA). Human prothrombin (FII)was from Hyphen BioMed (Andresy, France) and activated
factor X (FXa) from Biogenic S.A. (Mauguio, France). Acti-vated factor V(FVa) was a product from American Diagnostica
Clinical details, angiographic data and treatments are given in
(Greenwich, UK). Biotinylated recombinant human annexin V
Tables 1 and 2. Sex, risk factor distribution, median time to
was the same as that used elsewhere [1]. High binding capacity
therapy, localization of MI, multivessel disease, CPK peak, type
# 2003 International Society on Thrombosis and Haemostasis
Vitamin C, procoagulant microparticles and MI 173
Table 1 Baseline characteristics and medical history
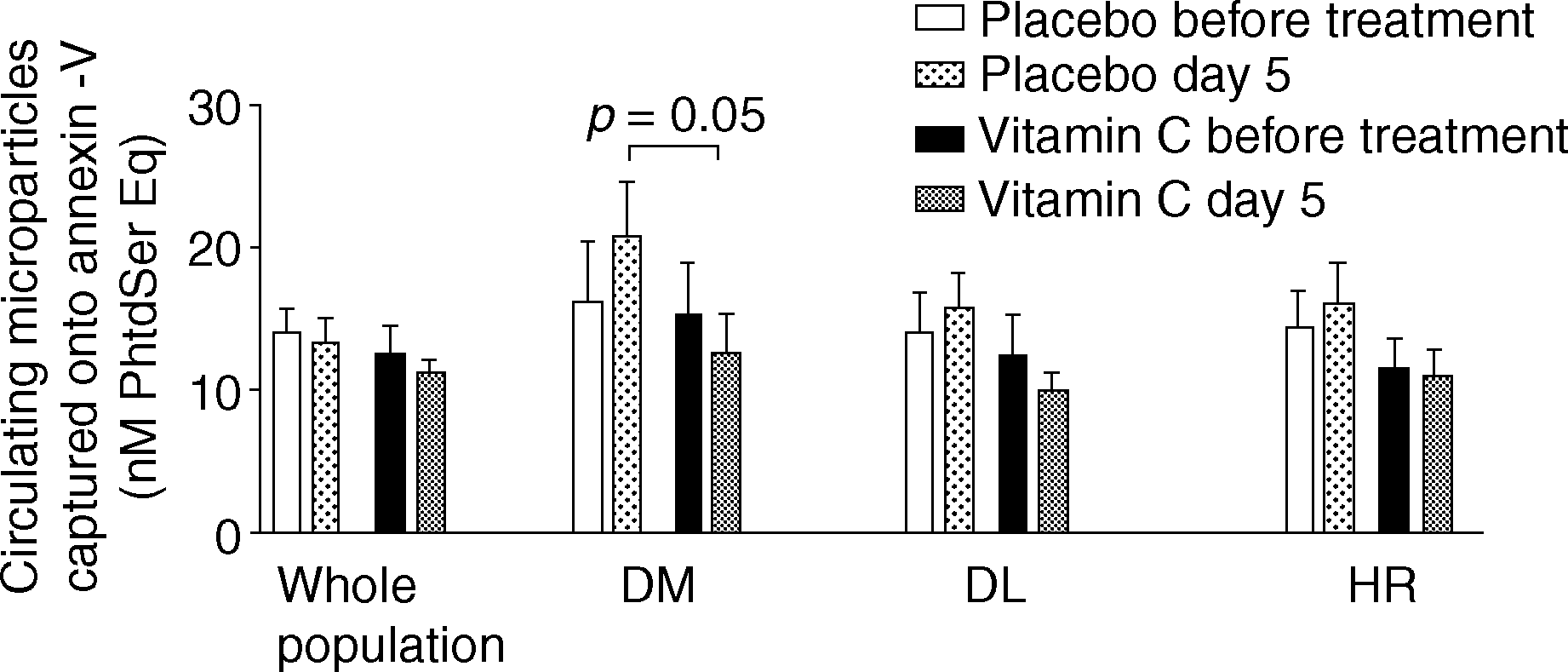
Fig. 1. Circulating procoagulant microparticles levels at day 5
Time from onset of pain to intervention (h)
following Myocardial Infarction in vitamin C and placebo groups. Whole
population (vitamin C: n ¼ 29; placebo: n ¼ 32), diabetes mellitus
Left ventricular ejection fraction assessed
(DM þ vitamin C: n ¼ 12; DM þ placebo n ¼ 11), dyslipidemic
(DL þ vitamin C: n ¼ 18; DL þ placebo: n ¼ 18), high-risk patients(HR þ vitamin C: n ¼ 20; HR þ placebo: n ¼ 18). Microparticles werecaptured onto annexin V. MP procoagulant phospholipid content was
measured as nanomolar phosphatidylserine equivalents (nmol LÀ1PhtdSer Eq) by functional prothrombinase assay.
Circulating procoagulant MP during myocardial infarction
With respect to values measured in HV, patients with MI pre-
sented high levels of procoagulant MP by capture onto annexin
V (MI 13.2 Æ 1.85 vs. HV 2.3 Æ 0.2 nmol LÀ1 PhtdSer Eq).
Circulating MP were mainly of platelet (MI 3.2 Æ 0.54 vs.
HV 0.58 Æ 0.10 nmol LÀ1 PhtdSer Eq) and endothelial (MI
0.48 Æ 0.20 vs. HV 0.02 Æ 0.006 nmol LÀ1 PhtdSer Eq) origin.
Values of circulating MP levels according to various risk factors
Coronary perfusion was assessed by TIMI flow scoring as defined by the
Effect of additional vitamin C treatment on procoagulant
Thrombolysis in myocardial infection study. TIMI 0 is defined by the
absence of antegrade flow, TIMI 1 by penetration of contrast withuncompleted opacification of the coronary vascular bed. ASA, acetylsa-
In the whole subset of patients with MI, the additional treatment
by vitamin C resulted in a slight ($14%) decrease in procoa-gulant MP captured onto annexin V, while an $4% reduction
of therapy were not statistically different between vitamin C-
was evidenced in the placebo group (Fig. 1). MP measurements
treated and untreated groups. At D1 after MI and before vitamin C
in treated or untreated patients, did not reach statistical differ-
administration, a non-significant difference between patients to
ence at D5 (vitamin C 10.8 Æ 1.3 vs. placebo 13.3 Æ 1.7
be treated by placebo and those to be treated by vitamin C was
nmol LÀ1 PhtdSer Eq). Interestingly, a significant difference
observed, the latter subset presenting a 11% lower mean value
was evidenced between untreated and vitamin C-treated DM
of circulating MP captured onto annexin V (vitamin C 12.45 Æ
patients who presented lower MP levels at D5 (DM þ vitamin C
1.9 vs. placebo 13.9 Æ 1.9 nmol LÀ1 PhtdSer Eq, P ¼ 0.57). This
12.7 Æ 2.6 vs. DM þ placebo 20.8 Æ 3.8 nmol LÀ1 PhtdSer Eq;
slight difference probably results from prospective randomiza-
P ¼ 0.05). Dyslipidemic and patients at high risk (HR) followed
tion. As the treatments applied were distributed equally between
a similar pattern although to a lesser extent (DL þ vitamin C
both subsets, they could hardly account for this observation.
9.9 Æ 1.3 vs. DL þ placebo 15.7 Æ 2.5 nmol LÀ1 PhtdSer Eq;
Table 3 Cell origin of circulating MP at day 1 after MI in diabetes mellitus (DM)(n ¼ 23), dyslipidemic (DL)(n ¼ 36) and high-risk (HR) patients(n ¼ 38). HV corresponds to healthy volunteers (n ¼ 50). No significant difference in the amount of circulating MP appeared at randomization betweenvitamin C and placebo group. Circulating MP were captured on antibodies to platelet (GPIb) or endothelial (CD31) membrane antigens. Procoagulantphospholipid content was measured by functional prothrombinase assay, and expressed as nanomolar phosphatidylserine equivalents (nmol LÀ1 PhtdSer Eq)
Circulating microparticles during myocardial infarction (day 1) (nM PhtdSer Eq)
# 2003 International Society on Thrombosis and Haemostasis
Fig. 2. Circulating procoagulant microparticles levels at day 5 followingMyocardial Infarction in diabetes mellitus and low-risk patients (LR).
Fig. 3. Platelet-derived microparticles levels at day 5 following
Diabetes mellitus (DM þ vitamin C: n ¼ 12; DM þ placebo n ¼ 11),
Myocardial Infarction in vitamin C and placebo groups. Whole population
low-risk patients (LR þ vitamin C: n ¼ 13; LR þ placebo: n ¼ 10).
(vitamin C: n ¼ 29; placebo: n ¼ 32), diabetes mellitus (DM vitamin C: n
Microparticles were captured onto annexin V. MP procoagulant
¼ 12; DM placebo: n ¼ 11), dyslipidemic (DL þ vitamin C: n ¼ 18; DL þ
phospholipid content was measured as nanomolar phosphatidylserine
placebo: n ¼ 18), high-risk patients (HR þ vitamin C: n ¼ 20; HR þ
equivalents (nM PhtdSer Eq) by functional prothrombinase assay.
placebo: n ¼ 18). Microparticles were captured onto anti-GPIb antibody. MP procoagulant phospholipid content was measured as nanomolarphosphatidylserine equivalents (nM PhtdSer Eq) by functional
P ¼ ns)(HR þ vitamin C 11.0 Æ 1.8 vs. HR þ placebo 16.2 Æ
2.5 nmol LÀ1 PhtdSer Eq; P ¼ ns)(Fig. 1). In these two subsetsof patients, placebo administration was associated with an$12% elevation in MP levels captured onto annexin V, to be
did not reach statistical significance at D5 (vitamin C 0.14 Æ
compared with the 28% elevation measured in DM patients.
0.02; placebo 0.39 Æ 0.18 nmol LÀ1 PhtdSer Eq). In HR or DL
Interestingly, in patients at lower risk (LR), circulating procoa-
patients significantly lower levels were, however, detected upon
gulant MP at D5 were reduced to the same extent in the presence
vitamin C treatment (DL þ vitamin C 0.12 Æ 0.03 vs. DL þ
or absence of additional vitamin C treatment, suggesting its
placebo 0.59 Æ 0.3 nmol LÀ1 PhtdSer Eq; P ¼ 0.05; HR þ vita-
inefficiency on MP release (placebo À34% and vitamin C
min C 0.11 Æ 0.03 vs. HR þ placebo 0.56 Æ 0.28 nmol LÀ1
PhtdSer Eq; P ¼ 0.04). In addition, a drastic elevation($60%) in circulating endothelial-derived MP was measuredin DM patients at D5 after placebo administration, whereas an
Effect of additional vitamin C treatment on platelet-derived
$70% reduction was observed after vitamin C treatment
(DM þ vitamin C 0.12 Æ 0.03 vs. DM þ placebo 0.97 Æ 0.7
Platelet-derived MP levels measured after capture onto GPIb
nmol LÀ1 PhtdSer Eq; P ¼ 0.06)(Fig. 4). As observed for plate-
antibody appeared decreased in vitamin C-treated patients
let-derived MP, a reduction in endothelial-derived MP was
regardless of the risk factor (vitamin C 2.2 Æ 0.4 vs. placebo
conversely found in LR patients, regardless of the treatment,
3.6 Æ 0.5 nmol LÀ1 PhtdSer Eq, P ¼ 0.01). However, the extent
67% and 50%, respectively, for vitamin C or placebo, the dif-
of the reduction varied with the clinical background. In
ference between the two subsets being-non-significant (LR þ
untreated DM and HR patients, platelet-derived MP levels
vitamin C 0.15 Æ 0.02 vs. LR þ placebo 0.35 Æ 0.19 nmol LÀ1
showed an $43% drastic increase after 5 days of placebo
administration reflecting an ongoing process of platelet stimu-lation (HR þ vitamin C 1.7 Æ 0.3 vs. HR þ placebo 3.9 Æ 0.7nmol LÀ1 PhtdSer Eq; DM þ vitamin C 3.0 Æ 0.6 vs. DM þplacebo 4.3 Æ 1.1 nmol LÀ1 PhtdSer Eq) (Fig. 3). In patients atlower risk (LR), neither placebo nor vitamin C administrationled to elevated platelet-derived MP; on the contrary, a reductionwas observed in both cases, the difference between both subsetsbeing non-significant (LR þ vitamin C 3.37 Æ 0.73 vs. LR þplacebo 3.22 Æ 0.38 nmol LÀ1 PhtdSer Eq, P ¼ ns).
Effect of additional vitamin C treatment on endothelial-derived MP during MI
Fig. 4. Endothelial-derived microparticles levels at day 5 followingMyocardial Infarction in vitamin C and placebo group. Whole population
Within the whole population of MI patients, a reduction of
(vitamin C: n ¼ 29; placebo: n ¼ 32), diabetes mellitus (DM þ vitamin C:
$65% in circulating endothelial-derived MP, captured onto
n ¼ 12; DM þ placebo: n ¼ 11), dyslipidemic (DL þ vitamin C: n ¼ 18;
anti-CD31 antibody, was evidenced after vitamin C treatment
DL þ placebo: n ¼ 18), high-risk patients (HR þ vitamin C: n ¼ 20; HR þplacebo: n ¼ 18). Microparticles were captured onto anti-CD31 antibody
whereas only an $29% decrease could be evidenced after
and their procoagulant phospholipid content measured by functional
5 days of placebo administration. Nevertheless, endothelial-
prothrombinase assay as nanomolar phosphatidylserine equivalents
derived MP levels measured in treated and untreated patients
# 2003 International Society on Thrombosis and Haemostasis
Vitamin C, procoagulant microparticles and MI 175
ed in acute coronary syndrome [33], pointing to underlying
endothelial apoptosis. In our study, endothelial-derived MP
In patients with MI taken as a whole population, the benefit of
were decreased by vitamin C treatment in DM, HR and DL
additional oral vitamin C treatment could appear modest with a
patients (70% reduction in DM), suggesting a major red-
14% decrease in circulating procoagulant MP levels compared
uction in endothelial damage (Fig. 4). In DM, results are
to the 4% reduction in patients with conventional treatment.
in accordance with the beneficial effects of vitamin C pre-
These measurements, performed after capture onto immobi-
viously demonstrated on endothelial function [18,34]. In-
lized annexin V, might underestimate MP populations present-
creased apoptosis and high oxidative stress are two features
ing a proportion of oxidized phospholipids restricting binding to
of DM [35]. Various serum factors, namely oxLDL, reactive
annexin V [24]. However, this limitation appears negligible in
oxygen species (ROS), angiotensin II, hyperglycemia-mediated
view of MP levels measured in clinical subsets in which high
superoxide induced endothelial cell apoptosis through en-
oxidative stress may account for enhanced cellular activation. A
hanced intracellular oxidative stress could be responsive to
significant elevation in circulating MP captured onto annexin V
the treatment [29]. In patients with congestive heart failure,
was detected in DM as well as the clear decrease upon vitamin C
vitamin C and carvedilol were both found to reduce endothelial
treatment. Furthermore, the inhibitory effect of vitamin C on
cell apoptosis, circulating levels of MP, and markers of oxida-
procoagulant MP release was not observed in patients at lower
risk (Fig. 2). In LR patients, amounts of circulating procoagu-
The drastic effect of additional vitamin C treatment on
lant MP were decreased to the same extent 5 days after vitamin
endothelial-derived MP measured in DM patients emphasizes
C or placebo administration. These opposite responses to
the specific role of endothelial apoptosis induced by ROS in
vitamin C treatment observed in DM and LR patients could
such a pathology. As an observation added in proof, no mod-
reflect a specific contribution of oxidative stress to vascular cell
ification in leukocyte-derived MP could be evidenced with
stimulation and MP release in HR patients. In LR patients,
respect to values measured in HV (data not shown). In DM,
oxidative stress might be overwhelmed by other stimuli such as
ROS could contribute to endothelium dysfunction by reducing
cytokines, shear stress, thrombin and tissue factor occurring,
bioavailability of NO [36,37], a potent mitochondrial mem-
generated or expressed during MI [25]. These observations
brane stabilizer [38,39], crucial for endothelial survival. ROS
confirm procoagulant MP as a relevant parameter to follow
could also promote the release of mitochondrial cytochrome c
an ongoing process of vascular damage during MI in patients at
Shed MP originating from apoptotic endothelial cells or
In accordance with previous reports from our group and
activated platelets are not only considered markers of vascular
others, platelet- and endothelial-derived MP appear to be the
damage but also behave as cellular effectors disseminating
two main sources of procoagulant MP released during MI [6,7].
proinflammatory, pro-adhesive, pro-apoptotic and prothrombo-
Unexpectedly, additional vitamin C treatment resulted in a 14%
tic potentials in the vasculature [41–45]. Recently, various
decrease in platelet-derived MP levels in spite of anti-platelet
phospholipids borne by MP shed from apoptotic endothelial
and antithrombin therapy. In DM and HR patients, although the
cells were found susceptible to oxidation and able to elicit
reduction after 5 days of vitamin C administration could appear
specific responses by vascular cells [24,46]. Furthermore, MP
modest per se (3% and 10%, respectively), it has to be compared
isolated from patients with MI selectively impair the endothe-
to the dramatic elevation in MP levels measured after placebo
lial NO transduction pathway [47]. Each MP population re-
administration (up to 44%). Thus, vitamin C prevents an on-
leased into the blood flow may have a specific contribution to
going process of platelet activation and membrane shedding in
the process of MI, which remains to be characterized. Likewise,
the susceptibility of membrane phospholipids and cells to
Diminished platelet aggregation and adhesion by vitamin C
oxidative stress probably differs with the lineage, explaining
has been evoked in previous studies [10,26,27]. In patients with
the variety of the vascular responses [48]. These observations
chronic heart failure, vitamin C enhanced platelet responsive-
lead to consider procoagulant circulating MP as an eventual
ness to the anti-aggregatory effects of NO donors, reduced
target for a pharmacological control in patients at high throm-
plasma lipid-derived free radicals and improved endothelial
function [28]. Various mechanisms may contribute to these
Our data suggest that an early additional antioxidant treat-
observations: (i) the formation of guanylate cyclase activation
ment may improve endothelial function particularly in subsets
and cGMP formation, a potent platelet inhibitor [29]; and (ii)
of patients in which high oxidative stress was previously
inhibition of inflammatory platelet activating factor mimetics
demonstrated, such as DL and DM groups. According to
preventing the formation of platelet-leukocytes aggregates and
the current understanding, vitamin C could promote an early
improvement of the cellular redox imbalance and prevent
Although representing a smaller proportion, endothelial-
NO inactivation in the vascular compartment. The associated
derived MP appeared highly susceptible to vitamin C treatment.
reduction in platelet activation, as evidenced by MP mea-
We previously showed that circulating endothelial-derived
surements, although less sensitive to antioxidant treatment,
MP testify to endothelial activation and/or apoptosis [7,32].
could also prove beneficial in patients at higher thrombotic
Indeed, low levels of circulating endothelial cells were report-
# 2003 International Society on Thrombosis and Haemostasis
21 Gokce N, Keaney JF Jr, Frei B et al. Long-term ascorbic acid admin-
istration reverses endothelial vasomotor dysfunction in patients with
We thank Fatiha Zobairi for kind and efficient help.
coronary artery disease. Circulation 1999; 99: 3234–40.
22 Fang JC, Kinlay S, Beltrame J et al. Effect of vitamins C and E on
progression of transplant-associated arteriosclerosis: a randomised trial.
23 Rossig L, Haendeler J, Mallat Z et al. Congestive heart failure induces
1 Aupeix K, Hugel B, Martin T et al. The significance of shed membrane
endothelial cell apoptosis: protective role of carvedilol. J Am Coll
particles during programmed cell death in vitro, and in vivo, in HIV-1
infection. J Clin Invest 1997; 99: 1546–54.
24 Huber J, Vales A, Mitulovic G et al. Oxidized membrane vesicles and
2 Laude I, Rongieres-Bertrand C, Boyer-Neumann C et al. Circulating
blebs from apoptotic cells contain biologically active oxidized phos-
procoagulant microparticles in women with unexplained pregnancy
pholipids that induce monocyte– endothelial interactions. Arterioscler
loss: a new insight. Thromb Haemost 2001; 85: 18–21.
3 Combes V, Simon AC, Grau GE et al. In vitro generation of endothelial
25 Ardissino D, Merlini PA, Bauer KA et al. Thrombogenic potential of
microparticles and possible prothrombotic activity in patients with
human coronary atherosclerotic plaques. Blood 2001; 98: 2726–9.
lupus anticoagulant. J Clin Invest 1999; 104: 93–102.
26 Wilkinson IB, Megson IL, MacCallum H, Sogo N, Cockcroft JR, Webb
4 Hugel B, Socie G, Vu T et al. Elevated levels of circulating procoagulant
DJ. Oral vitamin C reduces arterial stiffness and platelet aggregation in
microparticles in patients with paroxysmal nocturnal hemoglobinuria
humans. J Cardiovasc Pharmacol 1999; 34: 690–3.
and aplastic anemia. Blood 1999; 93: 3451–6.
27 Bordia A, Verma SK. Effect of vitamin C on platelet adhesiveness and
5 Freyssinet JM, Toti F, Hugel B et al. Apoptosis in vascular disease.
platelet aggregation in coronary artery disease patients. Clin Cardiol
6 Vidal C, Spaulding C, Picard F et al. Flow cytometry detection of
28 Ellis GR, Anderson RA, Chirkov YY et al. Acute effects of vitamin C on
platelet procoagulation activity and microparticles in patients with
platelet responsiveness to nitric oxide donors and endothelial function in
unstable angina treated by percutaneous coronary angioplasty and stent
patients with chronic heart failure. J Cardiovasc Pharmacol 2001; 37:
implantation. Thromb Haemost 2001; 86: 784–90.
7 Mallat Z, Benamer H, Hugel B et al. Elevated levels of shed membrane
29 Graier WF, Simecek S, Hoebel BG, Wascher TC, Dittrich P, Kostner
microparticles with procoagulant potential in the peripheral circulating
GM. Antioxidants prevent high-D-glucose-enhanced endothelial Ca2þ/
blood of patients with acute coronary syndromes. Circulation 2000;
cGMP response by scavenging superoxide anions. Eur J Pharmacol
8 Cai H, Harrison DG. Endothelial dysfunction in cardiovascular diseases:
30 Lehr HA, Frei B, Olofsson AM, Carew TE, Arfors KE. Protection from
the role of oxidant stress. Circ Res 2000; 87: 840–4.
oxidized LDL-induced leukocyte adhesion to microvascular and macro-
9 Ross R. Atherosclerosis – an inflammatory disease. N Engl J Med 1999;
vascular endothelium in vivo by vitamin C but not by vitamin E.
10 Caccese D, Pratico D, Ghiselli A et al. Superoxide anion and hydroxyl
31 Lehr HA, Weyrich AS, Saetzler RK et al. Vitamin C blocks inflam-
radical release by collagen-induced platelet aggregation – role
matory platelet-activating factor mimetics created by cigarette smoking.
of arachidonic acid metabolism. Thromb Haemost 2000; 83:
32 Rossig L, Hoffmann J, Hugel B et al. Vitamin C inhibits endothelial cell
11 Pratico D, Iuliano L, Mauriello A et al. Localization of distinct F2-
apoptosis in congestive heart failure. Circulation 2001; 104: 2182–7.
isoprostanes in human atherosclerotic lesions. J Clin Invest 1997; 100:
33 Mutin M, Canavy I, Blann A, Bory M, Sampol J, Dignat-George F.
Direct evidence of endothelial injury in acute myocardial infarction and
12 Reilly MP, Pratico D, Delanty N et al. Increased formation of distinct
unstable angina by demonstration of circulating endothelial cells. Blood
F2 isoprostanes in hypercholesterolemia. Circulation 1998; 98:
34 Virdis A, Ghiadoni L, Cardinal H et al. Mechanisms responsible for
13 Diaz MN, Frei B, Vita JA, Keaney JF Jr. Antioxidants and athero-
endothelial dysfunction induced by fasting hyperhomocystinemia in
sclerotic heart disease. N Engl J Med 1997; 337: 408–16.
normotensive subjects and patients with essential hypertension. J Am
14 Langlois M, Duprez D, Delanghe J, De Buyzere M, Clement DL. Serum
vitamin C concentration is low in peripheral arterial disease and is
35 Frustaci A, Kajstura J, Chimenti C et al. Myocardial cell death in human
associated with inflammation and severity of atherosclerosis. Circula-
diabetes. Circ Res 2000; 87: 1123–32.
36 Darley-Usmar V, White R. Disruption of vascular signalling by the
15 Vita JA, Keaney JF Jr, Raby KE et al. Low plasma ascorbic acid
reaction of nitric oxide with superoxide: implications for cardiovascular
independently predicts the presence of an unstable coronary syndrome.
disease. Exp Physiol 1997; 82: 305–16.
J Am Coll Cardiol 1998; 31: 980–6.
37 Laight DW, Carrier MJ, Anggard EE. Antioxidants, diabetes and
16 Pratico D, Tangirala RK, Rader DJ, Rokach J, FitzGerald GA. Vitamin E
endothelial dysfunction. Cardiovasc Res 2000; 47: 457–64.
suppresses isoprostane generation in vivo and reduces atherosclerosis in
38 Rossig L, Fichtlscherer B, Breitschopf K et al. Nitric oxide inhibits
ApoE-deficient mice. Nat Med 1998; 4: 1189–92.
caspase-3 by S-nitrosation in vivo. J Biol Chem 1999; 274: 6823–6.
17 Azevedo LC, Pedro MA, Souza LC et al. Oxidative stress as a signaling
39 Dimmeler S, Zeiher AM. Nitric oxide À an endothelial cell survival
mechanism of the vascular response to injury: the redox hypothesis of
factor. Cell Death Differ 1999; 6: 964–8.
restenosis. Cardiovasc Res 2000; 47: 436–45.
40 Green DR, Reed JC. Mitochondria and apoptosis. Science 1998; 281:
18 Ting HH, Timimi FK, Haley EA, Roddy MA, Ganz P, Creager MA.
Vitamin C improves endothelium-dependent vasodilation in forearm
41 Barry OP, Pratico D, Lawson JA, FitzGerald GA. Transcellular activa-
resistance vessels of humans with hypercholesterolemia. Circulation
tion of platelets and endothelial cells by bioactive lipids in platelet
microparticles. J Clin Invest 1997; 99: 2118–27.
19 Levine GN, Frei B, Koulouris SN, Gerhard MD, Keaney JF Jr, Vita JA.
42 Holme PA, Solum NO, Brosstad F, Pedersen T, Kveine M. Microvesicles
Ascorbic acid reverses endothelial vasomotor dysfunction in patients
bind soluble fibrinogen, adhere to immobilized fibrinogen and coag-
with coronary artery disease. Circulation 1996; 93: 1107–13.
gregate with platelets. Thromb Haemost 1998; 79: 389–94.
20 Heitzer T, Just H, Munzel T. Antioxidant vitamin C improves endothe-
43 Mesri M, Altieri DC. Endothelial cell activation by leukocyte micro-
lial dysfunction in chronic smokers. Circulation 1996; 94: 6–9.
particles. J Immunol 1998; 161: 4382–7.
# 2003 International Society on Thrombosis and Haemostasis
Vitamin C, procoagulant microparticles and MI 177
44 Mesri M, Altieri DC. Leukocyte microparticles stimulate endothelial
of monocytes and neutrophils. Proc Natl Acad Sci USA 1999; 96:
cell cytokine release and tissue factor induction in a JNK1 signaling
pathway. J Biol Chem 1999; 274: 23111–8.
47 Boulanger CM, Scoazec A, Ebrahimian T et al. Circulating micropar-
45 Joop K, Berckmans RJ, Nieuwland R et al. Microparticles from patients
ticles from patients with myocardial infarction cause endothelial dys-
with multiple organ dysfunction syndrome and sepsis support coagula-
function. Circulation 2001; 104: 2649–52.
tion through multiple mechanisms. Thromb Haemost 2001; 85: 810–20.
48 Burlacu A, Jinga V, Gafencu AV, Simionescu M. Severity of oxidative
46 Leitinger N, Tyner TR, Oslund L et al. Structurally similar
stress generates different mechanisms of endothelial cell death. Cell
oxidized phospholipids differentially regulate endothelial binding
# 2003 International Society on Thrombosis and Haemostasis
Working Guidelines Sarah MATHESON and John OSHA, Deputy Reporters General Anne Marie VERSCHUR, Sara ULFSDOTTER and Kazuhiko YOSHIDA Second medical use and other second indication claims Introduction This question seeks to determine the type, scope and enforcement of patent protection for new uses of known chemical compounds when a known substance is found to have a new therapeutic us
Anais do VIII Seminário de Iniciação Científica e V Jornada de Pesquisa e Pós-Graduação UNIVERSIDADE ESTADUAL DE GOIÁS Constituintes Químicos de Cochlospermum regium (Martius e Schrank) Pilger (Bixaceae) *1ANTUNES, M. N.; 2LIMA, R. S.; 2OLIVEIRA, C. R.; 2PEREIRA, A. G.; 1. Laboratório de Bioquímica e Parasitologia, Fundação de Medicina Tropical do Tocantins (FMT-
 Vitamin C, procoagulant microparticles and MI 173
Table 1 Baseline characteristics and medical history
Fig. 1. Circulating procoagulant microparticles levels at day 5
Time from onset of pain to intervention (h)
following Myocardial Infarction in vitamin C and placebo groups. Whole
population (vitamin C: n ¼ 29; placebo: n ¼ 32), diabetes mellitus
Left ventricular ejection fraction assessed
(DM þ vitamin C: n ¼ 12; DM þ placebo n ¼ 11), dyslipidemic
(DL þ vitamin C: n ¼ 18; DL þ placebo: n ¼ 18), high-risk patients(HR þ vitamin C: n ¼ 20; HR þ placebo: n ¼ 18). Microparticles werecaptured onto annexin V. MP procoagulant phospholipid content was
measured as nanomolar phosphatidylserine equivalents (nmol LÀ1PhtdSer Eq) by functional prothrombinase assay.
Vitamin C, procoagulant microparticles and MI 173
Table 1 Baseline characteristics and medical history
Fig. 1. Circulating procoagulant microparticles levels at day 5
Time from onset of pain to intervention (h)
following Myocardial Infarction in vitamin C and placebo groups. Whole
population (vitamin C: n ¼ 29; placebo: n ¼ 32), diabetes mellitus
Left ventricular ejection fraction assessed
(DM þ vitamin C: n ¼ 12; DM þ placebo n ¼ 11), dyslipidemic
(DL þ vitamin C: n ¼ 18; DL þ placebo: n ¼ 18), high-risk patients(HR þ vitamin C: n ¼ 20; HR þ placebo: n ¼ 18). Microparticles werecaptured onto annexin V. MP procoagulant phospholipid content was
measured as nanomolar phosphatidylserine equivalents (nmol LÀ1PhtdSer Eq) by functional prothrombinase assay.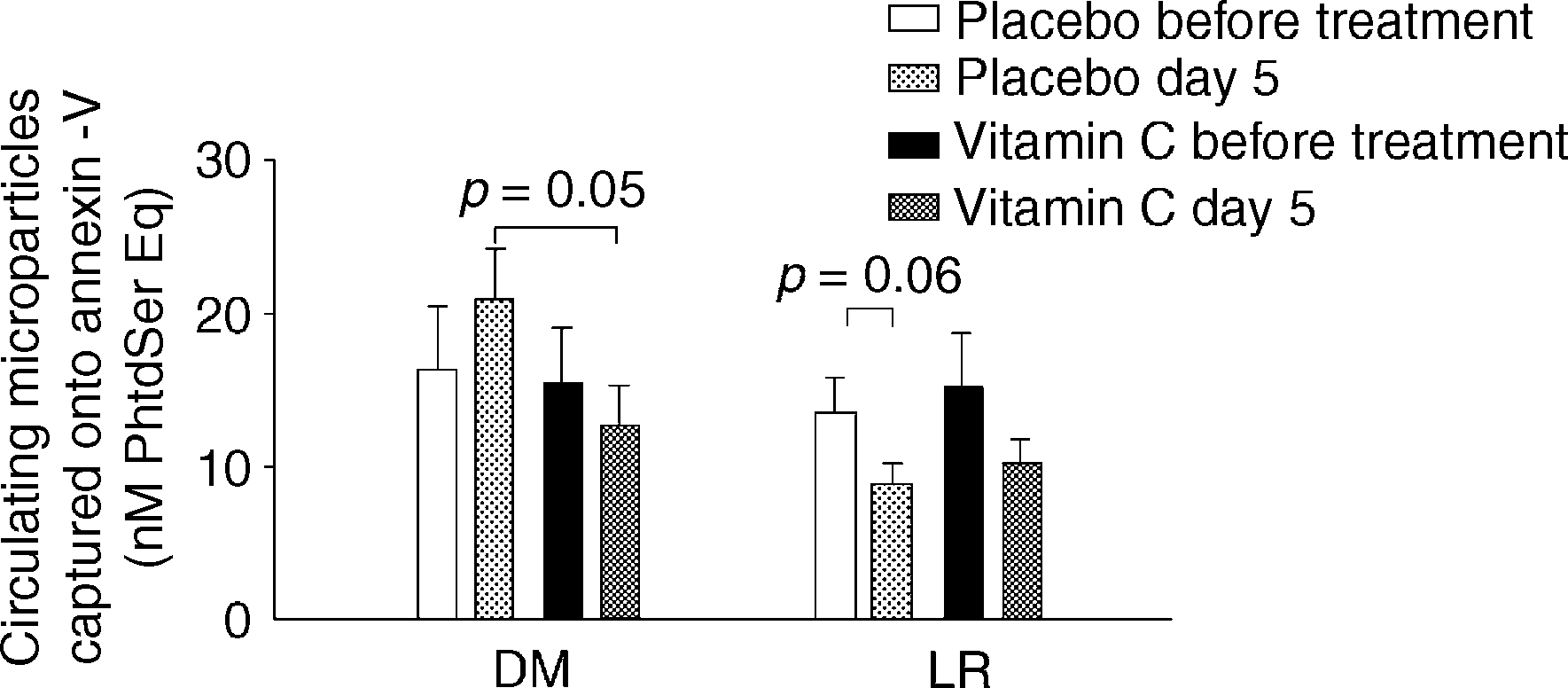
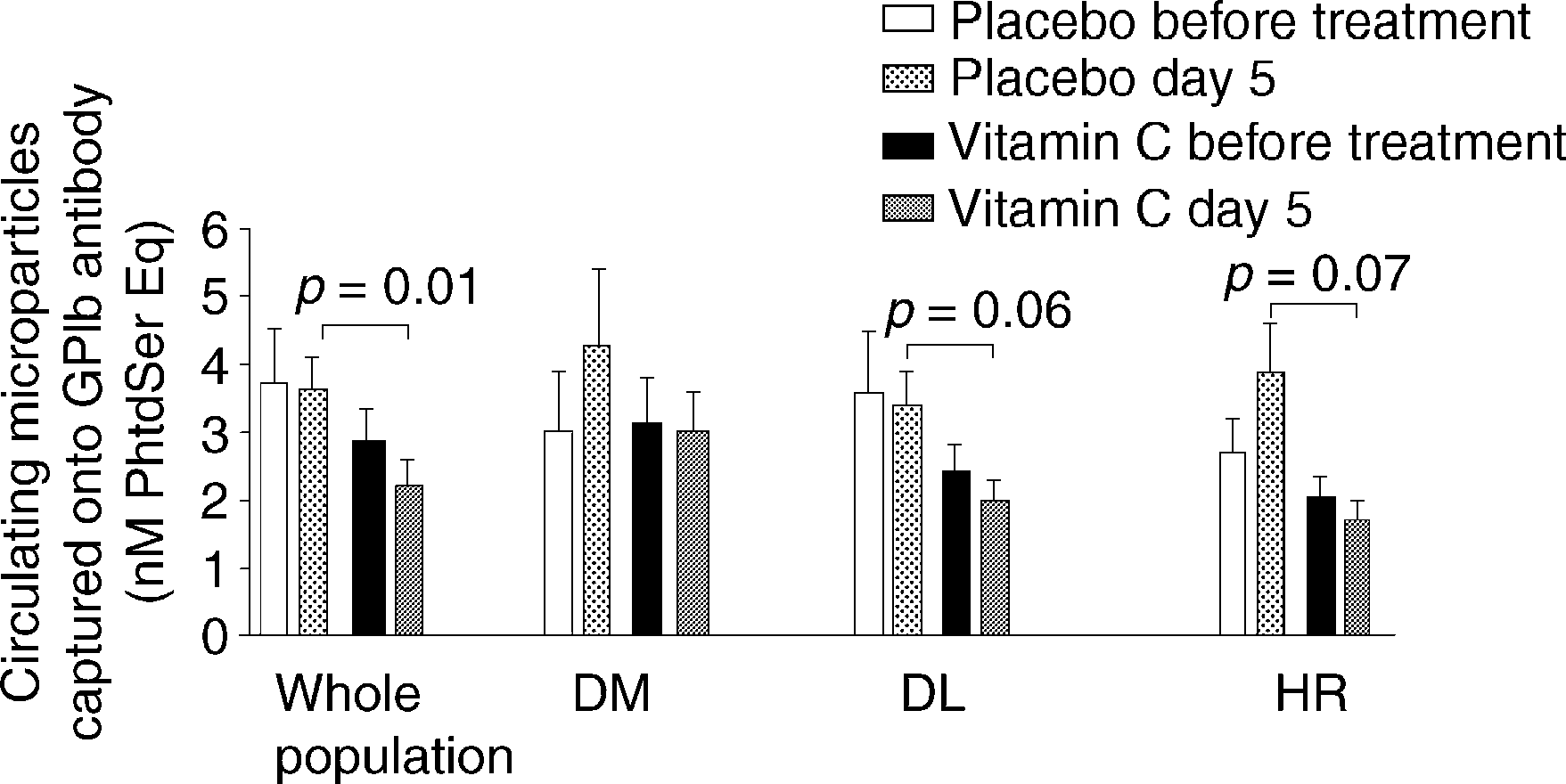
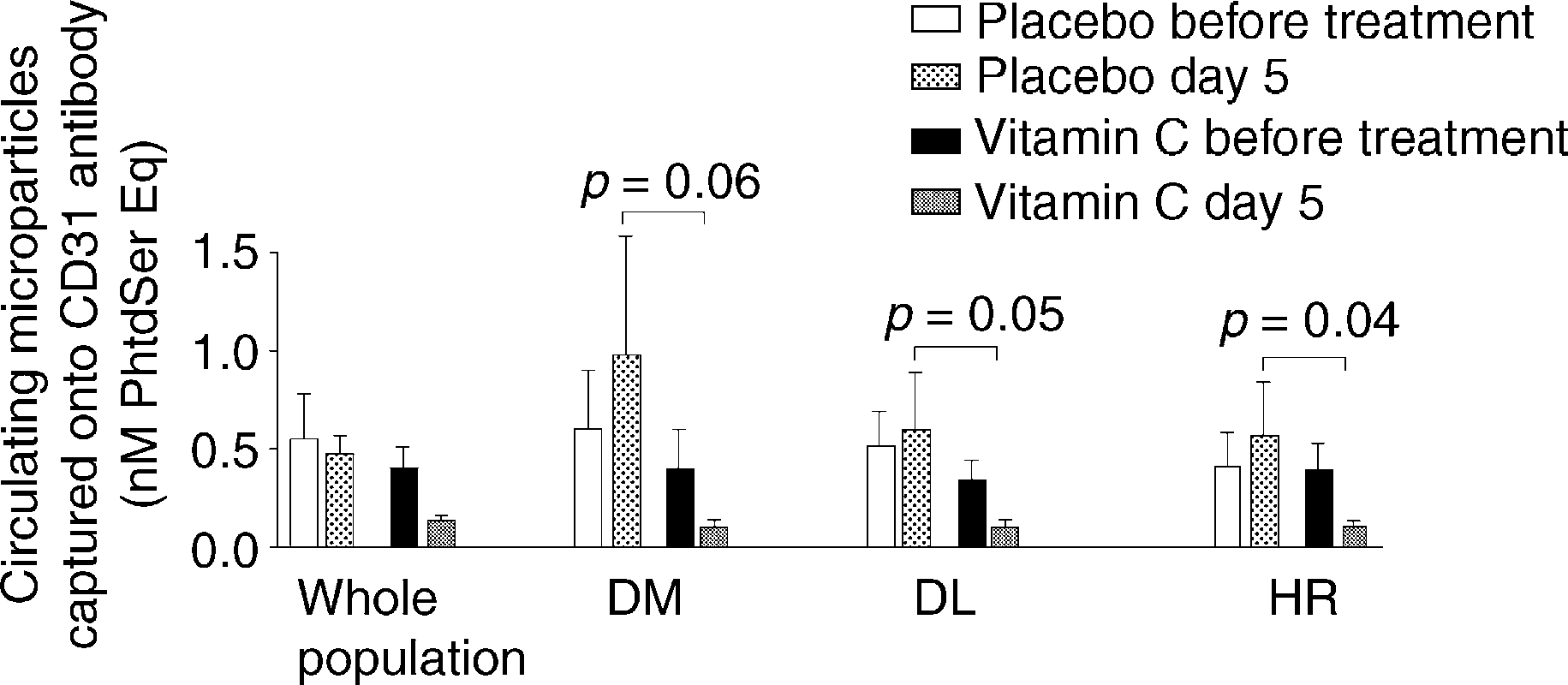 Fig. 2. Circulating procoagulant microparticles levels at day 5 followingMyocardial Infarction in diabetes mellitus and low-risk patients (LR).
Fig. 2. Circulating procoagulant microparticles levels at day 5 followingMyocardial Infarction in diabetes mellitus and low-risk patients (LR).