Le m├®tronidazole (Flagyl) reste la r├®f├®rence dans le traitement des infections ana├®robies et des parasitoses comme la giardiase ou lÔÇÖamibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irr├®versibles de lÔÇÖADN bact├®rien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gyn├®cologiques. LÔÇÖadministration prolong├®e est associ├®e ├á des effets neurologiques, incluant neuropathies p├®riph├®riques et enc├®phalopathies r├®versibles. LÔÇÖassociation avec lÔÇÖalcool d├®clenche une r├®action de type antabuse. Les guides th├®rapeutiques signalent que flagyl generique est mentionn├® dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
Doi:10.1016/s0003-9993(03)00357-5
High-Frequency Vibration Training Increases Muscle Power in Postmenopausal Women Cosimo Roberto Russo, MD, Fulvio Lauretani, MD, Stefania Bandinelli, MD, Benedetta Bartali, MD, Chiara Cavazzini, MD, Jack M. Guralnik, MD, PhD, Luigi Ferrucci, MD, PhD
ABSTRACT. Russo CR, Lauretani F, Bandinelli S, Bartali
age. Although evidence is overwhelming that physical exercise
B, Cavazzini C, Guralnik JM, Ferrucci L. High-frequency
positively affects muscle strength at all ages, compliance of
vibration training increases muscle power in postmenopausal
older persons with traditional exercise programs has generally
women. Arch Phys Med Rehabil 2003;84:1854-7.
been low, and only a small percentage of older persons exerciseregularly.3
Objective: To test whether training on a high-frequency
Vibration exercise on ground-based platforms that oscillate
(28Hz) vibrating platform improves muscle power and bone
at high frequency has recently been proposed as an intervention
characteristics in postmenopausal women.
for the prevention and the treatment of osteoporosis.4-6 High-
Design: Randomized controlled trial with 6-month follow-
frequency (28Hz), very-low-magnitude (0.3g) vibration exer-
cise has recently been reported to increase bone mass in ex-
Setting: Outpatient clinic in a general hospital in Italy. Participants: Twenty-nine postmenopausal women (inter-
mechanism by which vibrations influence the bone tissue re-
vention group, n¤¡14; matched controls, n¤¡15). Intervention: Participants stood on a ground-based oscillat-
The high-frequency postural displacements induced by the
ing platform for three 2-minute sessions for a total of 6 minutes
alternating movements of the platform produce reflex muscle
per training session, twice weekly for 6 months. The controls
contractions aimed at stabilizing posture.11 Thus, vibration can
did not receive any training. Both groups were evaluated at
be viewed as a special form of muscle training that may
particularly affect muscle power.12 It has been proposed that
Main Outcome Measure: Muscle power, calculated from
the force applied to bone during muscle contraction has a
ground reaction forces produced by landing after jumping as
pivotal role in the homeostatic and adaptive regulation of bone
high as possible on a forceplate, cortical bone density, and
strength.13,14 This hypothesis may explain, in part, the mecha-
nism by which vibration improves bone strength. To test this
Results: Over 6 months, muscle power improved by about
hypothesis, we conducted a small, randomized controlled trial
5% in women who received the intervention, and it remained
(RCT) to discover whether training on a high-frequency vibrat-
unchanged in controls (P¤¡.004). Muscle force remained stable
ing board for 6 months would improve muscle power in post-
in both the intervention and control groups. No significant
menopausal women and, in turn, positively influence bone
changes were observed in bone characteristics. Conclusion: Reflex muscular contractions induced by vibra-
tion training improve muscle power in postmenopausal
Key Words: Bone density; Exercise; Muscles; Postmeno-
pause; Rehabilitation; Vibration; Women. 2003 by the American Congress of Rehabilitation Medi-
All the study procedures, including recruitment, measure-
cine and the American Academy of Physical Medicine and
ments, and intervention, were performed in the Nuovo San
Giovanni di Dio Hospital in Florence, Italy. The recruitmentphase began in spring 1999 and was completed in fall 1999. MUSCLE POWER, the capacity of muscles to produce The intervention began in the winter 1999ÔÇô2000 and was
work in the environment, declines significantly over the
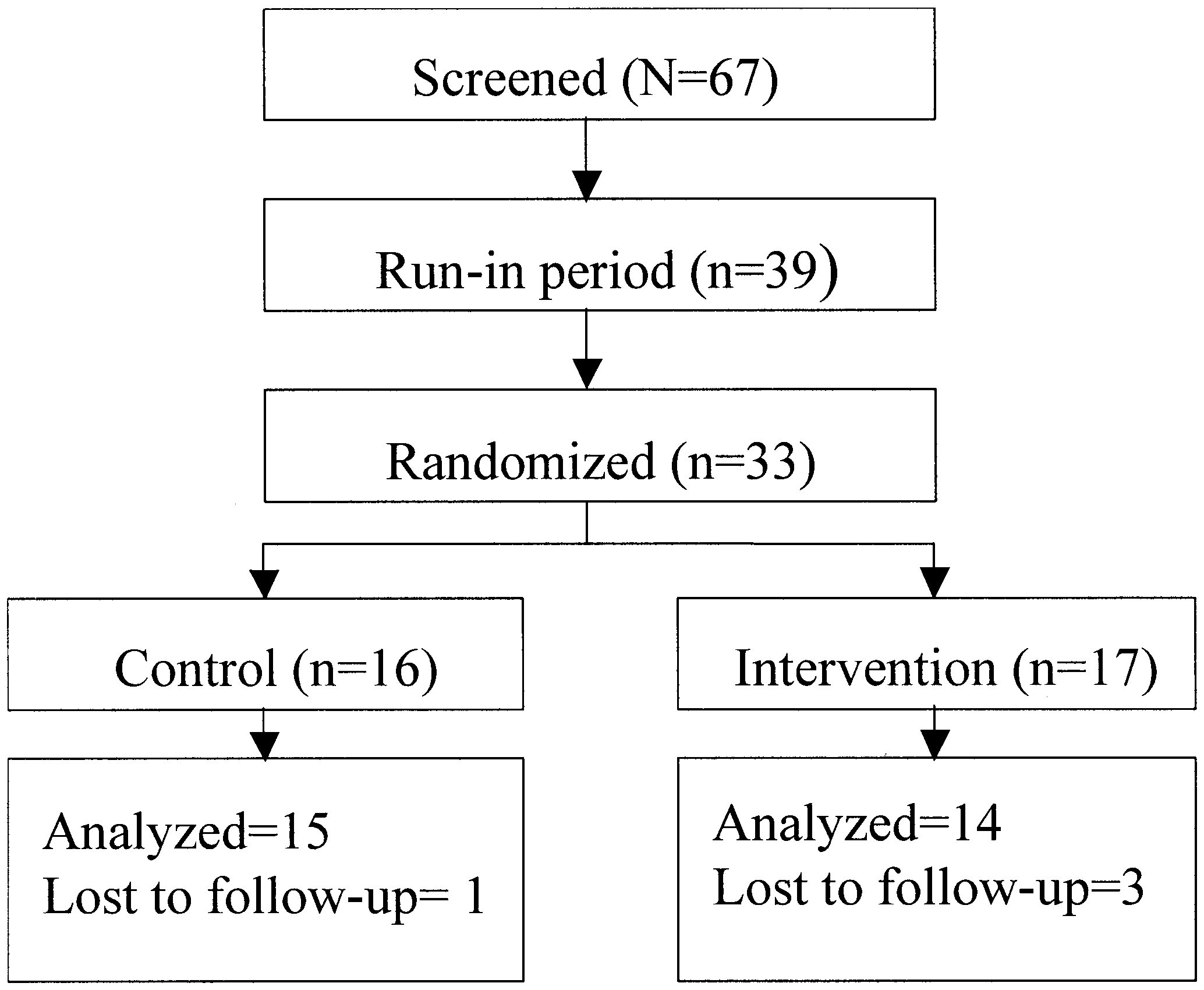
completed by summer 2000. Among the 67 women belonging
life span. In women, the rate of decline accelerates after meno-
to a hospital volunteers association (Associazione Volontari
pause and leads to reduction in physical functioning.1 It has
Ospedalieri), 39 women who were at least 1 year postmeno-
been hypothesized that this process may be responsible for the
pausal and not affected by conditions that contraindicated the
development of physical frailty and mobility disability1,2 in old
vibration training were enrolled in the study population (fig 1). Women on hormone replacement therapy were consideredeligible. Women with metabolic bone disorders were excludedfrom the trial.
From the Laboratory of Clinical Epidemiology, INRCA Geriatric Department,
The screened women entered a 3-month run-in phase during
Florence, Italy (Russo, Lauretani, Bandinelli, Bartali, Cavazzini); Laboratory of
which they received daily 1g of calcium carbonate and .25ÔÉ«g
Epidemiology, Demography, and Biometry, National Institute on Aging, Bethesda,
of activated vitamin D (calcitriol). This supplementation was
MD (Guralnik); and Longitudinal Studies Section, ASTRA Unit, Clinical ResearchBranch, National Institute on Aging, Baltimore, MD (Ferrucci).
administered to all the participants for the entire study period to
Stratec Medizintechnik, Novotec, and Unitrem provided the peripheral quantitative
avoid any influence of insufficient calcium or vitamin D intake
computerized tomograph and the forceplates.
on the effects of vibration exercise on bone apposition and
No commercial party having a direct financial interest in the results of the research
mineralization. Because of the nature of the intervention, no
supporting this article has or will confer a benefit upon the author(s) or upon anyorganization with which the author(s) is/are associated.
blinding or placebo was considered. Of the 67 screened
Reprint requests to Luigi Ferrucci, MD, PhD, Longitudinal Studies Section, Clin-
women, 33 agreed to participate in the study, signed an in-
ical Research Branch, Gerontology Research Center, National Institute on Aging,
formed consent, and were randomized to either vibration or
5600 Nathan Shock Dr, Rm 6BN, Baltimore, MD 21224.
control group. A simple randomization procedure was applied
0003-9993/03/8412-7841$30.00/0doi:10.1016/S0003-9993(03)00357-5
using a series of random numbers. Six of the 39 eligible women
Arch Phys Med Rehabil Vol 84, December 2003 VIBRATION TRAINING INCREASES MUSCLE POWER, Russo
cross-sectional image of the tibial diaphysis at 38% of the tibiallength from its distal end. In these images, all of the voxelswith a density above 710mg/cm3 were considered to belong tocortical bone. Intervention
The active intervention consisted of brief training sessions
conducted twice weekly for 6 months. In each session, vibra-tion was provided by a commercially available device (Galileo2000d). By means of an oscillating board, this device delivershigh-frequency vibration through the legs to the whole body. Participants stood with feet side by side on the board, whichproduced lateral oscillations of the whole body with accelera-tions in the range of 0.1 to 10g. At the beginning of thetraining, participants stood on the board with the knees slightlyflexed and received three 1-minute bouts of vibration separatedby 1-minute resting periods. During the first month of treat-ment, the frequency of vibration was progressively increasedfrom 12 to 28Hz to allow for gentle adaptation. During thefollowing 5 months of treatment, the frequency was always setat 28Hz, and the bouts of vibration were prolonged to 2
Fig 1. Flow diagram of the RCT.
minutes. Participants were invited to separate the feet as far astolerated to increase the amplitude and speed of the verticaldisplacement. Previous studies11 have demonstrated that theoscillating movement of the board produces muscle stretching,
refused to participate in the trial owing to family problems
which elicits alternating reflex contraction of the flexor and
extensor leg muscle groups. Participants in the active group
Measurements
attended on average 34 sessions, corresponding to about 200minutes of treatment, out of 44 sessions potentially available.
Blood and urine tests were performed to exclude from the
trial subjects affected by metabolic bone disorders like primary
Statistical Analysis
hyperparathyroidism or hyperparathyroidism secondary to re-nal failure. All blood samples were drawn in the morning
All analyses were performed using the SAS, version 8.2,
statistical software.e Data are reported as mean ¤« standard
chemical parameters, which included total serum calcium, se-
error (SE). Baseline characteristics of the intervention and
rum phosphorus, and creatinine, were measured using standard
control group were compared by 1-way analysis of variance
laboratory methods. Serum parathyroid hormone (PTH) was
(ANOVA). The magnitude of change over time in muscle and
measured by a double-antibody chemoluminescence methoda
bone parameters in the intervention versus control group was
(interassay cell volume [CV]¤¡2%), and serum bone-specific
compared using a repeated-measures ANOVA.
alkaline phosphatase was measured using an immunoenzy-matic methodb (interassay CV¤¡5%). Deoxipiridinoline and
N-terminal telopeptide were measured using a 1-step chemolu-
Women who received the active intervention were similar to
minescence methoda (interassay CV¤¡3%) and immunoenzyi-
controls in age, baseline muscle power, years since menopause,
matic methodc (interassay CV¤¡10%), respectively. To collect
anthropometric measures, routine biochemical measurements,
the 2-hour morning urine, participants were instructed to get up
and biomarkers of bone turnover (table 1). Final measurement
early in the morning and void. After 2 hours of fasting, during
of the primary outcome (muscle power) was obtained in 29 of
which only ingestion of water was allowed, participants voided
the 33 women who had been originally randomized (14 active
again, and all urine samples were collected and used for mea-
treatment, 15 controls). Dropouts in the intervention group
surements. To assess muscle power, participants, starting from
were caused by family problems (n¤¡2) and knee pain (n¤¡1).
a standstill, jumped as high as possible and landed on a force-
In 1 control, a measure of muscle power at the final follow-up
plated that measured ground reaction forces.15 The best of 4
could not be obtained because of posttraumatic muscle pain.
attempts was used in the analysis. The acceleration of the
After 6 months, muscle power improved by about 5% (from
center of gravity (COG) was calculated as the ratio of force (N)
178.9¤«9.6W to 187.3¤«9.5W) in women who received the
and body mass (kg). The integration of acceleration by time
active treatment (table 2), whereas it declined slightly in con-
gives the instantaneous velocity of the COG (m/s). The power
trols. In a repeated-measure ANOVA, change over time in
(W) is obtained as the product of force and velocity. Tibial
muscle power differed statistically between the 2 groups
bone density, mass, and geometry were assessed by a recent
(P¤¢.02). Overall, muscle power improved in 80% of the
generation, high-resolution, peripheral quantitative computed
women in the treatment group and in 46% in the controls
tomography device (XCT 2000d). Volumetric total bone den-
(P¤¡.06). The velocity increased in the intervention group to a
sity (mg/cm3) was measured as the average density of the
similar extent as the power (from 163.7¤«6.2m/s to 171.7¤«
whole cross-section of the tibial metaphysis (4% of the tibial
5.3m/s, P¤¢.005), whereas muscle force did not change signif-
length from its distal end); that is, the section mainly composed
of trabecular bone surrounded by a thin cortical shell. At the
Cortical bone density remained stable in the intervention
same site we assessed trabecular bone density (mg/cm3) by
group, whereas it declined significantly in the control group
excluding cortical bone. Measures of cortical bone density
(P¤¢.05). However, in a repeated-measure ANOVA, the de-
(mg/cm3) and cross-sectional area (mm2) were obtained from a
cline in cortical bone density over time did not differ statisti-
Arch Phys Med Rehabil Vol 84, December 2003 VIBRATION TRAINING INCREASES MUSCLE POWER, Russo Table 1: Characteristics of the Participants at Baseline
Abbreviations: BMI, body mass index; HRT, hormone replacement therapy.
cally between the 2 groups (P¤¡.09). All other bone parameters,
occurrence in the life of a woman, perhaps contributing to
including biochemical indices of bone turnover, did not change
physical frailty and mobility disability in late life.2 Studies17
significantly during the study period in either group.
have demonstrated that such a decline may be slowed by
Transient, slight lower leg itching and erythema, a known
strength training exercise. However, the compliance of older
side effect of the vibration exercise,16 was also observed in 6 of
persons in traditional exercise programs is poor.
17 treated participants in this study. In no case, however, did
High-frequency vibration on a ground-based platform stim-
this problem persist after the first 3 training sessions or cause
ulates continuously alternating reflex contractions of flexor and
interruption of the intervention. Knee pain of moderate inten-
extensor muscle groups of the lower extremities.11 We hypoth-
sity, without objective clinical signs, was observed in 2 over-
esized that vibration is a special type of exercise that may be
weight participants with preexisting knee osteoarthritis. The
particularly suitable for older persons. It does not require much
pain subsided in both participants after a few days of rest. One
time or effort, does not cause potentially traumatic vertical
of them, however, refused to continue and was dropped from
displacements of the involved joints, and specifically trains
type II muscle fibers, which are selectively lost during theaging process.16,18 The availability of a simple, safe, and well-
DISCUSSION
accepted training method that can improve muscle power in
In the present study, 200 minutes of high-frequency whole-
postmenopausal women opens a new perspective for the pre-
body vibration, distributed in biweekly sessions over 6 months,
vention of age-associated loss of muscle function in this group
improved muscle power and the velocity of movement in
postmenopausal women without significant changes in muscle
Previous studies have demonstrated that vibration exercise
force. These results suggest that vibration training improves
improves bone mineral density in animal and human models.
muscle power mainly by enhancing the pattern of recruitment
Our findings provide a possible explanation for this effect of
vibration exercise. Mechanical stress produced by muscle con-
This study is the first to show an improvement of muscle
traction plays a critical role in the maintenance of bone
power in postmenopausal women using vibration exercise. The
strength.19,20 Thus, improvement in muscle force and power
decline in muscle power is an early and apparently inexorable
may be a strategy for improving bone characteristics and pre-
Table 2: Effect of 6 Months of High-Frequency Vibration Training on Muscle and Bone Parameters
Trabecular volumetric bone density (mg/cm3)
Cortical volumetric bone density (mg/cm3)
*Testing whether change over time in the specific parameter differed between groups. ÔÇáMean values are calculated only with subjects who had valid measures both at baseline and at 6-month follow-up. Arch Phys Med Rehabil Vol 84, December 2003 VIBRATION TRAINING INCREASES MUSCLE POWER, Russo
venting osteoporosis in postmenopausal women. In accordance
5. Rubin C, Xu G, Judex S. The anabolic activity of bone tissue,
with this hypothesis, our study showed that the decline in
suppressed by disuse, is normalized by brief exposure to ex-
cortical bone density tended to be greater among control
tremely low-magnitude mechanical stimuli. FASEB J 2001;15:
women than among women who received the active treatment.
Our findings on cortical bone volumetric density are consistent
6. Rubin C, Turner AS, Bain S, Mallinckrodt C, McLeod K. Anab-
with earlier reports21 and support the hypothesis that vibration
olism. Low mechanical signals strengthen long bones. Nature
exercise may positively affect bone characteristics.10 However,
clinical trials that address these issues would require longer
7. Rubin C, Turner AS, Muller R, et al. Quantity and quality of
follow-up and, probably, a more intensive intervention. Based
trabecular bone in the femur are enhanced by a strongly anabolic,noninvasive mechanical intervention. J Bone Miner Res 2002;17:
on earlier reports and on the present findings, our conclusion is
that vibration exercise may be a more useful tool for the
8. Flieger J, Karachalios T, Khaldi L, Raptou P, Lyritis G. Mechan-
prevention and treatment of osteoporosis than pharmacologic
ical stimulation in the form of vibration prevents postmenopausal
treatment of osteoporosis,22,23 a disease that is generally under-
bone loss in ovariectomized rats. Calcif Tissue Int 1998;63:510-4.
9. Ward KA, Alsop CW, Brown S, Caulton J, Adams JE, Maughal Z.
The vibration training was safe overall. The only clinically
A randomised, placebo controlled, pilot trial of low magnitude,
significant side effect was knee pain, which was observed in 2
high frequency loading treatment of low bone mineral density in
participants with preexisting osteoarthritis of the knee. This
children with disabling conditions [abstract]. J Bone Miner Res
pain caused cessation of treatment in 1 subject. The frequent
occurrence of transient lower leg erythema reported16 previ-
10. Eisman JA. Good, good, good . . . good vibrations: the best option
ously was often observed in the present study, but it was
for better bones? Lancet 2001;358:1924-5.
always transient, mild, and not disturbing.
11. Seidel H. Myoelectrical reaction to ultra-low frequency and low
The present study has several limitations. First, the small
frequency whole body vibration. Eur J Appl Physiol 1988;57:558-62.
number of participants and the relatively short duration of the
12. Ferrucci L, Russo CR, Lauretani F, Bandinelli S, Guralnik JM. A
intervention might have prevented us from identifying treat-
role for sarcopenia in late-life osteoporosis. Aging Clin Exp Res
ment effects on secondary outcomes such as muscle force or
bone parameters. However, the effect on the primary outcome,
13. Frost HM, Ferretti JL, Jee WS. Perspectives: some roles of me-
muscle power, was small but clear-cut and therefore unlikely to
chanical usage, muscle strength, and the mechanostat in skeletal
be due to chance. Likewise, the treatmentÔÇÖs safety clearly needs
physiology, disease, and research. Calcif Tissue Int 1998;62:1-7.
to be tested in larger studies. Second, the compliance with the
14. Turner CH. Three rules for bone adaptation to mechanical stimuli.
treatment sessions was suboptimal; in fact, only 34 of 44
sessions were attended on average. However, an important
15. Rittweger J, Gunga HC, Felsenberg D, Kirsch KA. Muscle and
bone-aging and space. J Gravit Physiol 1999;6:P133-6.
reason for the low attendance was the restricted choice of days
16. Rittweger J, Beller G, Felsenberg D. Acute physiological effects
and time offered to the participants for the training sessions
of exhaustive whole-body vibration exercise in man. Clin Physiol
(because of our lack of financial resources). The training was
perceived as very useful by the participants, who uniformly
17. Nied RJ, Franklin B. Promoting and prescribing exercise for the
reported an improved well-being as a consequence of the
elderly. Am Fam Physician 2002;65:419-26.
training. Moreover, it can be considered a striking finding of
18. Evans WJ. What is sarcopenia? J Gerontol A Biol Sci Med Sci
this study that a substantial improvement in muscle power was
obtained with only 200 minutes of training.
19. Schonau E. The development of the skeletal system in children
and the influence of muscular strength. Horm Res 1998;49:27-31. CONCLUSION
20. Blain H, Vuillemin A, Teissier A, Hanesse B, Guillemin F,
Jeandel C. Influence of muscle strength and body weight and
The results of this small RCT suggest that high-frequency
composition on regional bone mineral density in healthy women
vibration exercise is a feasible, safe, convenient, and effica-
aged 60 years and over. Gerontology 2001;47:207-12.
cious intervention, which could prevent the decline in muscle
21. Adami S, Gatti D, Braga V, Bianchini D, Rossini M. Site-specific
and bone strength in postmenopausal women. Such interven-
effects of strength training on bone structure and geometry of
tion can easily be added as a component of an exercise-based
ultradistal radius in postmenopausal women. J Bone Miner Res
prevention program or even prescribed as the sole intervention
when traditional exercise is not feasible.
22. Ferrucci L, Benvenuti E, Bartali B, et al. Preventive health care for
older women: life-style recommendations and new directions. Aging Clin Exp Res 2000;12:113-31. Acknowledgments:
23. Marcus R. Role of exercise in preventing and treating osteoporo-
formed all of the biochemical measurements.
sis. Rheum Dis Clin North Am 2001;27:131-41. References
24. Siris ES, Miller PD, Barrett-Connor E, et al. Identification and
1. Thomas M, Fiatarone MA, Fielding RA. Leg power in young
fracture outcomes of undiagnosed low bone mineral density in
women: relationship to body composition, strength, and function.
postmenopausal women: results from the National Osteoporosis
Med Sci Sports Exerc 1996;28:1321-6.
Risk Assessment. JAMA 2001;286:2815-22.
2. Suzuki T, Bean JF, Fielding RA. Muscle power of the ankle
25. Chesnut CH III. Osteoporosis, an underdiagnosed disease. JAMA
flexors predicts functional performance in community-dwelling
older women. J Am Geriatr Soc 2001;49:1161-7.
3. Mazzeo RS, Tanaka H. Exercise prescription for the elderly:
Suppliers
current recommendations. Sports Med 2001;31:809-18.
a. Medical Systems, Via Rio Torbido 40, 16165 Genoa, Italy.
4. Russo CR. High frequency vibration exercise: evaluation of a new
b. Quidel Ltd, Via Gobetti 2, 20017 Rho, Milan, Italy.
treatment through a prospective, randomised, controlled trial. Pa-
c. Bouty, Via Casiraghi 471, 20099 Sesto S. Giovanni, Milan, Italy.
per presented at: the XII National Meeting of the Italian Society of
d. Unitrem, Via Gioia Tauro 22, 100040 Morena, Rome, Italy.
Osteoporosis; 2000 Oct 11-14; Abano Terme, Padua (Italy).
e. SAS Institute Inc, 100 SAS Campus Dr, Cary, NC 27513. Arch Phys Med Rehabil Vol 84, December 2003
Medizinische Informationen zu HIV und AIDSFunktionsst├Ârungenbei M├ñnnern mit HIV & AIDSDas Gesicht der HIV-Infektion hat sich durch die neuen Therapiem├Âglich-keiten stark ver├ñndert: Standen fr├╝her schwer zu behandelnde Krankhei-ten wie zum Beispiel das Kaposi-Sarkom im Vordergrund, sind es heutemehr die mittel- und langfristigen Nebenwirkungen der antiretroviralenMedikamente. Dazu geh├
Resident Events for 2012 London and Surrey eventsKent eventsSussex eventsIf you need further information on any of these events, please call 0800 121 6060 and ask for the member of staff specified with the event. APRIL 2012 EVENTS: information please contact KentWendy Tipton - Resident information please contact KentWendy Tipton - Resident Teynham Village Hall, 10.00am ÔÇô 12.00pminf
 VIBRATION TRAINING INCREASES MUSCLE POWER, Russo
VIBRATION TRAINING INCREASES MUSCLE POWER, Russo