Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
20060044.883_887.tp
Clin Chem Lab Med 2006;44(7):883–887 ᮊ 2006 by Walter de Gruyter • Berlin • New York. DOI 10.1515/CCLM.2006.160
Establishment of detailed reference values for luteinizing hormone, follicle stimulating hormone, estradiol, and progesterone during different phases of the menstrual cycle on the Abbott ARCHITECTᮋ analyzer Reto Stricker1,*, Raphael Eberhart1, Marie-
Normal reproductive endocrine function involves a
Christine Chevailler1, Frank A. Quinn2, Paul
wide variety of hormones controlled by a number of
Bischof3 and Rene´ Stricker1
intricate feedback mechanisms (1). This is particularlytrue during the menstrual cycle, in which serum levels
of luteinizing hormone (LH), follicle-stimulating hor-
2 Abbott Diagnostics, Abbott Park, IL, USA
mone (FSH), estradiol, and progesterone follow a
3 Laboratoire d’Hormonologie Maternite´, Department
cyclical pattern closely coordinated by the hypothal-
of Obstetrics and Gynaecology, University of
mic-pituitary-gonadal axis (1, 2). Because LH, FSH,
estradiol, and progesterone play such a central rolein female reproductive function, measurement of theserum concentration of these hormones is important
Abstract
in the diagnosis, treatment, and monitoring of manydifferent conditions (1). According to the Clinical and
During a normal menstrual cycle, serum levels of
Laboratory Standards Institute (CLSI; formerly the
luteinizing hormone (LH), follicle-stimulating hor-
National Committee for Clinical Laboratory Standard-
mone (FSH), estradiol, and progesterone can vary
ization, NCCLS), ‘‘for a decision making process to
widely between cycles for the same woman, as well
occur, reference values are needed for all tests in the
as between different woman. Reliable reference val-
clinical laboratory’’ (3). Assay manufacturers typically
ues based on the local population are important for
provide reference range data for their assays. Ideally,
correct interpretation of laboratory results. The pur-
laboratories should either verify these ranges or
pose of our study was to determine detailed reference
determine their own reference ranges, based on the
values for these hormones throughout the menstrual
populations they serve. However, performing detailed
cycle using the Abbott ARCHITECT system. From 20
reference range studies can be logistically complex,
volunteers (age 20–36 years) with normal cycles andno use of oral contraceptives, samples were taken
and are beyond the capabilities of many clinical
every day during their cycle. Volunteers received
laboratories. This is especially true for reproductive
three vaginal ultrasound examinations (days 10 and
hormones, for which serum concentrations vary sig-
13, and 1 or 2 days after ovulation) to measure follic-
nificantly throughout the menstrual cycle, as well as
ular and corpus luteum development. Hormone levels
from woman to woman, and collection of multiple
were measured using the corresponding ARCHITECT
samples across many days is required to establish
assay and were synchronized to the LH peak. Median,
reference values with any degree of resolution (4).
and 5th and 95th percentile values were determined
The purpose of our study was to obtain detailed ref-
for each day of the cycle, as well as for early follicular
erence values for LH, FSH, estradiol, and progester-
(days y15 to y6), late follicular (days y5 to y1), LH
one for each day and phase of the menstrual cycle
peak (day 0), early luteal (q1 to q4), mid-luteal (days
q5 to q9), and late luteal (days q10 to q14) phases
From 20 apparently healthy female volunteers (age
of the cycle. Based on our data, we were able to
range 20–36 years) with normal menstrual cycles and
establish detailed reference values for LH, FSH, estra-
no use of oral contraceptives or other medications,
diol, and progesterone, which should aid in the inter-
serum samples were collected on every day of the
pretation of results for these reproductive hormones
cycle. Each sample was then assayed for LH, FSH,
estradiol, and progesterone using the Abbott ARCHI-
Park, IL, USA). Reagent list numbers for these assays
Keywords: ARCHITECT analyzer; estradiol; follicle-
were: LH, 6C25; FSH, 6C24; estradiol, 2K25; and pro-
stimulating hormone; luteinizing hormone; progester-
gesterone, 6C26. The ARCHITECT i2000
paramagnetic microparticles and chemiluminescentdetection technology (5). Assays were performed
*Corresponding author: Reto Stricker, DIANALAB SA, 6 ruede la Colline, Geneva, Switzerland
according to the manufacturer’s instructions. Analyt-
ical performance characteristics (e.g., imprecision,
Stricker et al.: Hormone reference values
Reference range data for LH and FSH by day in normal cycling women.
sensitivity, method comparison) for these assays
n-19, 5th and 95th percentile values are reported for
have previously been reported (6–9). Per the manu-
illustrative purposes only, and these data should be
facturer, the assays are standardized accordingly: LH,
interpreted with caution. Data were analyzed using
WHO 2nd IS 80/552; FSH, WHO 2nd IRP 78/549; estra-
Microsoft Excel 2000 (Microsoft, Redmond, WA,
diol, gravimetric, ID-GCMS verified; progesterone,
USA). The study protocol was reviewed and approved
gravimetric, USP grade progesterone. For analysis of
by the internal institutional Review Board.
serum hormone concentrations, variations in the
Data for normal cycling women by day of cycle,
cycle length were normalized by defining ‘‘day 0’’
with median, and 5th and 95th percentiles, are shown
based on the peak LH value for each woman. To
in Table 1 and represented graphically in Figure 1.
ensure a normal cycle was taking place, volunteers
Reference values for different phases of the menstrual
received three vaginal ultrasound examinations (days
cycle are shown in Table 2. During the early follicular
10 and 13, and 1 or 2 days post-ovulation) to measure
phase (days y15 to y6) median, and 5th and 95th
follicular and corpus luteum development. Ovulation
percentile values were: LH, 3.96 (2.01 and 7.80) IU/L;
occurred in all cycles used for data analysis. Owing
FSH, 6.42 (3.91 and 8.76) IU/L; estradiol, 149.74 (77.99
to the highly specialized nature of the sample set
and 266.08) pmol/L; and progesterone, 0.64 (0.32 and
required to perform this study, obtaining a large num-
1.91) nmol/L. For the late follicular phase (days y 5
ber of specimens from many different women repre-
to y1), median, and 5th and 95th percentile values
senting each day of their menstrual cycle was
were: LH, 5.68 (3.24 and 14.68) IU/L; FSH, 4.66 (2.97
logistically challenging. In recommendations for the
and 6.99) IU/L; estradiol, 450.49 (195.43 and 1146.91)
determination of reference values, the CLSI recogniz-
pmol/L; and progesterone, 0.64 (0.32 and 1.59)
es that collecting large numbers of certain sample
nmol/L. During the LH peak (defined as day 0), medi-
types may be ‘‘difficult, if not impossible’’; in such
an, and 5th and 95th percentile values were: LH, 41.19
cases, their guidance is to report ‘‘percentiles appro-
(21.16 and 73.63) IU/L; FSH, 12.82 (5.30 and 15.07)
priate to the number of values obtained’’ (3). In the
IU/L; estradiol, 671.06 (482.00 and 1425.39) pmol/L;
present study, reference values were defined by cal-
and progesterone, 2.54 (1.24 and 4.13) nmol/L. For the
culating the median, and 5th and 95th percentiles in
early luteal phase (days q1 to q4), median, and 5th
sample sets of nG19, the minimum number needed
and 95th percentile values were: LH, 7.86 (3.65 and
to define these percentiles (3). For sample sets with
18.03) IU/L; FSH, 5.62 (3.02 and 11.09) IU/L; estradiol,
Stricker et al.: Hormone reference values
Reference range data for estradiol and progesterone by day in normal cycling women.
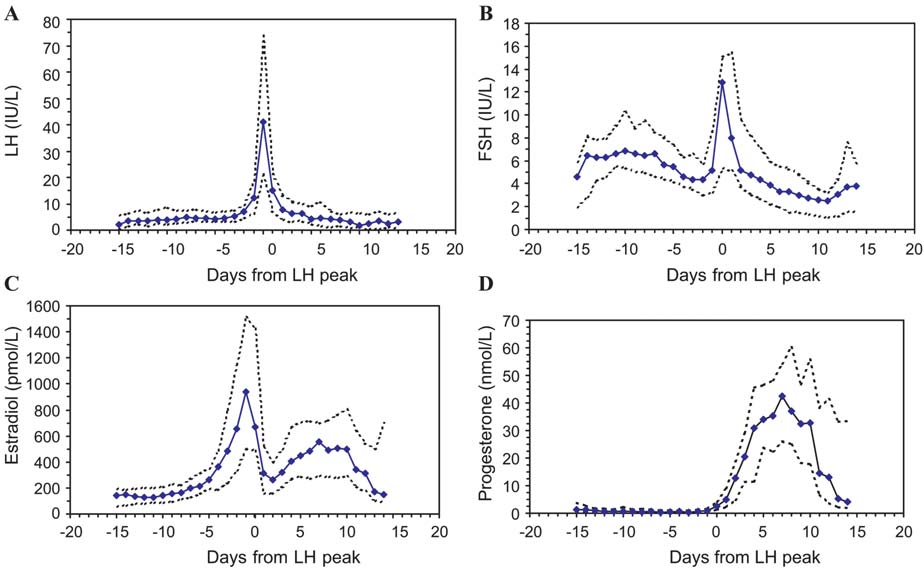
Hormone values in daily serum samples across the menstrual cycle for normal women: (A) luteinizing hormone;
(B) follicle-stimulating hormone; (C) estradiol; and (D) progesterone. Solid lines represent median values; dotted lines rep-resent 5th and 95th percentiles.
Stricker et al.: Hormone reference values
Reference values during different phases of the menstrual cycle.
313.42 (178.14 and 566.43) pmol/L; and progesterone,
important for physicians and laboratories to be aware
13.67 (3.15 and 39.65) nmol/L. During the mid-luteal
of the potential sources of differences that exist
phase (days q5 to q9), median, and 5th and 95th per-
between immunoassay methodologies, and confirm
centile values were: LH, 3.88 (1.05 and 9.73) IU/L; FSH,
that the reference values they use for reproductive
3.14 (1.48 and 5.31) IU/L; estradiol, 495.82 (275.95 and
hormones are valid for the populations they serve.
761.67) pmol/L; and progesterone, 36.25 (21.21 and
Based on our study, we were able to develop detailed
54.28) nmol/L. For the late-luteal phase (days q10 to
reference ranges for LH, FSH, estradiol, and proges-
q14), median, and 5th and 95th percentile values
terone on the Abbott ARCHITECT analyzer during the
were: LH, 2.75 (0.51 and 6.98) IU/L; FSH, 2.85 (1.14 and
normal menstrual cycle. These data should aid labo-
5.64) IU/L; estradiol, 327.36 (100.52 and 787.14)
ratories and physicians in the interpretation of results
pmol/L; and progesterone, 13.99 (1.96 and 49.18)
for these reproductive hormones in a wide variety of
In general, our data are in agreement with those
provided by the assay manufacturer. However, directcomparison is difficult, as our data were analyzed to
References
a higher degree of resolution, allowing establishmentof reference values in greater detail throughout the
1. Gronowski AN, Landau-Levine ME. Reproductive endo-
menstrual cycle. It should be noted that gonadotropin
crine function. In: Burtis CA, Ashwood ER, editors. Tietz
hormones are known to be highly heterogeneous (10,
fundamentals of clinical chemistry. Philadelphia: WB
11). This heterogeneity is presumably one of the fac-
tors that leads to assay differences reported in the
2. Marshall JC. Hormonal regulation of the menstrual cycle
literature (12). These differences can, in turn, affect
and mechanisms of ovulation. In: DeGroot LJ, Jameson
interpretation of results from different assay manu-
JL, editors. Endocrinology. Philadelphia, PA: WB Saun-
facturers or laboratories. For example, FSH concen-
3. Clinical and Laboratory Standards Institute. How to define
tration on day 3 of the menstrual cycle (along with
and determine reference intervals in the clinical labora-
estradiol and inhibin B) is commonly used by physi-
tory; approved guideline, 2nd ed. Document c28-A2. Vil-
cians to evaluate ovarian reserve. Taieb and col-
leagues, in their study of six different immunoassays
4. Dighe AS, Moy JM, Hayes FJ, Sluss PM. High-resolution
for FSH, noted statistically significant differences for
reference ranges for estradiol, luteinizing hormone, and
day-3 FSH values, depending on which immunoassay
follicle stimulating hormone in men and women using theAxSYM assay system. Clin Biochem 2005;38:175–9.
was used. Their data prompted them to recommend
‘‘that it is advisable to refer patients to selected lab-
Wild D, editor. The immunoassay handbook, 3rd ed.
oratories using analytical methods for which they
have defined reference values «’’ (12). Similarly,
6. Yang DT, Owen WE, Ramsay CS, Xie H, Roberts WL. Per-
measurement of serum estradiol is important in eval-
formance characteristics of eight estradiol immunoas-
uating a variety of conditions, including abnormal
says. Am J Clin Pathol 2004;122:332–7.
7. Hendriks HA, Kortlandt W, Verweij WM. Analytical per-
menstrual cycles. However, measurement of steroid
formance comparison of five new generation immuno-
hormones (such as estradiol) by immunoassay is
assay analyzers. Ned Tijdschr Klin Chem 2000;25:170–7.
notoriously difficult, and differences in assay perform-
8. Verheecke P, Quinn FA. Laboratory evaluation of repre-
ance significant enough to affect clinical utility have
sentative disease state assays on the Abbott ARCHITECTᮋ
been reported (6). For these reasons, it is especially
i2000ᮋ analyzer. J Assoc Lab Automat 2000;5:30–3.
Stricker et al.: Hormone reference values
9. Rufo G, Brookhart P, Barnes W, Frels M, Sheu M, White
gonadotropins through the normal menstrual cycle and
M, et al. Performance characteristics of the Abbott
in the post-menopause state. Mol Hum Reprod 1998;47:
ARCHITECT progesterone assay wabstractx. Clin Chem
12. Taieb J, Olivennes F, Birr AS, Benattarc C, Righini C,
10. Stanton PG, Burgon PG, Hearn MT, Robertson DM.
Frydman R, et al. Comparison of day 3 FSH values as
Structural and functional characterization of hFSH and
determined by six different immunoassays. Hum Reprod
hLH isoforms. Mol Cell Endocrinol 1996;125:133–41.
11. Anobile CJ, Talbot JA, McCann SJ, Padmanabhan V,
Received February 1, 2006, accepted April 18, 2006
(Rev. Esp. Anestesiol. Reanim. 2005; 52: 109-114) CASO CLÍNICO Tratamiento con radiofrecuencia pulsada en dos casos de neuralgiaglosofaríngea idiopática y secundaria. Resultados preliminaresD. Abejón*, S. García del Valle**, C. Nieto*, C. Delgado***, J. I. Gómez-Arnau****Área de Anestesia, Reanimación y Cuidados Críticos. Unidad de Dolor. Fundación Hospital Alcorcón. Alcorcón. Madr
For carers and relatives of people with fronto-temporal Happy New Year! Sorry for the delay in sending this latest edition of the newsletter – we realise it’s been a while but we wanted to be able to confirm a date for the next meeting before getting in touch. Thanks to all of you who attended our meeting on the 25th October. In this meeting Sarah
 Stricker et al.: Hormone reference values
Reference range data for estradiol and progesterone by day in normal cycling women.
Stricker et al.: Hormone reference values
Reference range data for estradiol and progesterone by day in normal cycling women.