Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
Determining the optimal pelvic floor muscle training regimen for women with stress urinary incontinence
Neurourology and Urodynamics 30:746–753 (2011)
Determining the Optimal Pelvic Floor Muscle Training Regimen for Women with Stress Urinary Incontinence Chantale Dumoulin,1∗ Cathryn Glazener,2§ and David Jenkinson2 1Faculty of Medicine, School of Physiotherapy, University of Montreal, Montreal, Canada2Health Services Research Unit, University of Aberdeen, Aberdeen, UK
Pelvic floor muscle (PFM) training has received Level-A evidence rating in the treatment of stress urinary incontinence(SUI) in women, based on meta-analysis of numerous randomized control trials (RCTs) and is recommended in manypublished guidelines. However, the actual regimen of PFM training used varies widely in these RCTs. Hence, to date,the optimal PFM training regimen for achieving continence remains unknown and the following questions persist: howoften should women attend PFM training sessions and how many contractions should they perform for maximal effect?Is a regimen of strengthening exercises better than a motor control strategy or functional retraining? Is it better toadminister a PFM training regimen to an individual or are group sessions equally effective, or better? Which is better,PFM training by itself or in combination with biofeedback, neuromuscular electrical stimulation, and/or vaginal cones?Should we use improvement or cure as the ultimate outcome to determine which regimen is the best? The questions areendless. As a starting point in our endeavour to identify optimal PFM training regimens, the aim of this study is (a) toreview the present evidence in terms of the effectiveness of different PFM training regimens in women with SUI and(b) to discuss the current literature on PFM dysfunction in SUI women, including the up-to-date evidence on skeletalmuscle training theory and other factors known to impact on women’s participation in and adherence to PFM training. Neurourol. Urodynam. 30:746–753, 2011. 2011 Wiley-Liss, Inc. Key words: pelvic floor muscle training; stress urinary incontinence; women INTRODUCTION PFM TRAINING ALONE VERSUS NO TREATMENT STUDIES
National and international clinical practice guidelines recom-
The effects of PFM training for women with urinary incon-
mend supervised pelvic floor muscle (PFM) training as a first-line
tinence (UI) as compared to no treatment, a placebo or sham
treatment for stress urinary incontinence (SUI) in women (Level
treatment were recently evaluated in a Cochrane Review.2 The
of evidence A).1--4 The goal is to improve the functioning
Cochrane Incontinence Group’s Specialised Trials Register and
of the PFMs.2 Essentially, PFM training can be prescribed to
the reference lists of relevant articles were searched (February
18, 2009). Randomized and quasi-randomized trials and the tar-geted population (women with stress, urgency, or mixed UI)
• PFM strength (the maximum force generated by a muscle in a
were among the selection criteria. In this review, at least one
component of each trial had to include PFM training. The com-
• PFM endurance (the ability to perform repetitive contractions
parators were no treatment, a placebo or a sham treatment, or
or to sustain a single contraction over time), and
another type of inactive control treatment.
• PFM coordination (muscular activity prior to effort and on
Fourteen trials involving 836 women met the inclusion cri-
teria. Within the 14 trials, only 8 (370 women) contributed
data exclusively for women with SUI and were also suitablefor analysis (Table I). There were considerable variations in the
Supervised by a trained health professional, progressive PFM
exercise regimens and often their descriptions were not exten-
training involves various PFM exercises either with or without
sive. Generally, the exercise programmes consisted of strength,
adjunctive biofeedback, electro-neurostimulation, intra-vaginalresistance, and/or a bladder diary.1 The uncertainty aboutwhich of these strategies are most effective in training womento use their PFM to cure or improve symptoms of SUI has beenidentified by a wide panel of patients and experts to be one of
Linda Brubaker led the review process.
the key clinical questions which needs to be prioritized.5
In order to determine the best regimen for treating SUI in
The work was performed at ICI-RS 2010. §
women, this study begins with a review of the up-to-date evi-
Professor of Health Research. Research Fellow.
dence of the effectiveness of PFM training regimens alone as
∗Correspondence to: Chantale Dumoulin, Ph.D., Associate Professor, Facult´e de
compared to no treatment or a placebo treatment, the evi-
M´edecine, ´Ecole de R´eadaptation, Universit´e de Montr´eal, C.P. 6128 Succ. Centre-
dence for the comparative effectiveness of different types of PFM
ville, Montr´eal, Qu´ebec, Canada H3C 3J7. E-mail: chantal.dumoulin@umontreal.caReceived 3 February 2011; Accepted 15 February 2011
training regimens and, finally, the evidence for PFM training in
Published online 15 June 2011 in Wiley Online Library (wileyonlinelibrary.com).
combination with various adjunct therapies.
Optimal Training For Women With Stress Incontinence
TABLE I. PFM Training Programs From RCTs Comparing PFM Training to a Control
Short programme aimed at improving coordination
between a VPFMC and a rise in intra-abdominalpressure
Set: 8--12 high-intensity maximal VPFMC with a 6- 8 sec
hold followed by 3--4 fast contractions at the end of
each, and a 6 sec rest between maximal contractions
Exercises done in different body positions included
supine, kneeling, sitting, and standing—all with thelegs apart
Set: 10 VPFMC, with 5 sec hold and 10 sec rest. Progressed
at 2 weeks to 10 sec hold and 20 sec rest
VPFMC confirmed by surface electromyography with
Set: not stated (not clear if 30 total or 30 each), taking
Strength: burst of intense activity lasting a few secondsEndurance: 6 sec holds progressed by 1 sec/week to 12 secSets per day: 30 VPFMC
Set: 10 VPFMC with 3 sec hold, and 10 VPFMC with 10 sec
hold. Progressed by 10 per set to daily maximum of 200
Weekly clinic visits with nurseDrop out: 10 group not
Sets: 5 VPFMC with 10 sec hold, 10 VPFMC with 5 sec hold,
20 PFMC with 2 sec hold, 20 VPFMC with 1 sec hold, 5
Sets: 10 VPFMC with 3 sec hold, 10 VPFMC with 10 sec
hold in sitting, lying, and standing positions with the
PFM, pelvic floor muscle; VPFMC, voluntary PFM contraction; PFMT, PFM training; Set, one episode or sequence of PFM contractions or training, including lengthof time of holding contraction, positions while performing contractions and number of repetitions of contractions.
endurance or coordination training, or a combination of these:
Despite these difficulties, the review found that PFM-trained
women with SUI were about 17 times more likely to report cure
1. Programmes with a low number of repetitions and high
of incontinence compared to those having non-active control
loads (maximal effort) were classified as strength training.
management in one trial (RR 16.8, 95% CI: 2.4--119.0). Addition-
2. Those that included a high number of repetitions
ally, PFM-trained women with SUI were 17 times more likely to
or prolonged contractions with low-to-moderate loads
report improvement or cure of their symptoms (RR 17.33, 95% CI:
(submaximal contractions) were classified as endurance
4.31--69.64, in two trials). Moreover, they experienced between
0.8 and 3 fewer leakage episodes per 24 hr compared to women
3. Those that employed the repeated use of a PFM contraction
in non-active treatments. Finally, PFM-trained women with SUI
in response to a specific situation (e.g., prior to cough, “The
were 5--16 times more likely to be continent on a short pad test
Knack”) were classified as coordination training.
4. For the most part, PFM training programmes were diffi-
Overall, the best conclusion that could be derived from the
cult to categorize because they described either a mixed
review is that PFM training is better than no treatment, placebo
(e.g., strength and endurance) programme or omitted a key
drug, or inactive control treatments for women with SUI. Vari-
training parameter (e.g., the amount of voluntary effort per
ations in the PFM training programmes were a major source
contraction, number or duration of contractions per set, dura-
of clinical heterogeneity, preventing a comparative analysis of
tion or frequency of sets per day, Table I).
the training programmes and their potential effectiveness. The
Neurourology and Urodynamics DOI: 10.1002/nau
study trials, however suggested that treatment effects (in terms
to cure incontinence than no treatment (Fig. 1). Furthermore,
of self-reported cure/improvement) might be greater in women
all of the interventions examined (with the exceptions of PFM
with SUI participating in a supervised PFM training programme
training with vaginal cones and biofeedback, and PFM training
with Duloxetine), were significantly better than no treatmentat improving SUI (HTA monograph18 Fig. 32, p. 105). Moreover,there was also clear evidence that when women attended forPFM training in more than 2 sessions per month it was more
COMPARISON OF DIFFERENT PFM TRAINING REGIMENS
effective than 2 or fewer sessions per month (cure: medianodds ratio 8.36, 95% credible interval 3.74--21.7; improvement:
Twelve trials comparing different PFM exercise regimens in
median odds ratio 5.75, 95% credible interval 2.11--16.2). There-
SUI women were found in the literature review, very few of
fore, PFM training reinforced with biofeedback or PFM provided
which compared the same regimens. In most trials, the partici-
in extra sessions appear to be the most effective interventions,
pant numbers were few; consequently the confidence intervals
although there is some uncertainty surrounding this.18
were wide and the results were inconclusive (Table II).6--17
So in summary, in terms of treatments specifically targeting
Because of this limitation, the review of the available data was
women with SUI, the up-to-date evidence does not clearly iden-
unable to discern clear differences between the following train-
tify an optimal PFM training regime. However, the evidence
does suggest that supervised PFMT programmes delivered more
often (more than 2 sessions per month) or augmented with
maximal versus submaximal strength training,6
biofeedback appear to be more effective. In order to identify
strength/motor relearning versus motor relearning alone,7
the parameters of an optimal PFM training, rigorous adequately
PFM training with and without deep abdominal muscle
powered RTCs must be conducted in which different models of
exercises in the supine position versus a combination of posi-
This being said, there are, however, certain elements in the
literature pertaining to (a) the biological rationale for PFM train-
direct PFM training versus indirect or imitation PFM training
ing, (b) PFM dysfunction in women with SUI, (c) skeletal muscle
through the hip abductor muscles,10,11 or
training theory as progressive overload, and (d) behavior and
adherence strategies which impact on women’s participationand adherence to PFM training programmes. These are dis-
cussed in detail below and must be taken into consideration
cure/improvement if PFMT was taught and supervised by
when designing optimal PFM training regimens which might
a health professional versus self-administered.14 Further,
be amenable to testing by randomized control trial (RCT).
self-reported cure or cure/improvement in SUI women wasmore likely with more health professional contact during PFMTversus less health professional contact (Table II).15,16
BIOLOGICAL RATIONALE FOR PFM TRAINING
The biological rationale for using PFM training is twofold. PFM TRAINING IN COMBINATION WITH VARIOUS ADJUNCT
Firstly, a voluntary contraction before and during a cough (a
THERAPIES STUDIES
maneuver termed “The Knack”) has been shown to effectivelyreduce urinary leakage during a cough.19 Hence, simply learn-
More recently, the effectiveness of PFM training combination
ing to contract the PFM before a cough may be, in and of itself,
with various adjunct therapies has been studied using mixed
sufficient treatment for those women who experience leakage
treatment comparison models. These are sophisticated meta-
during coughing; and as such should be included in all PFM
analyses that handle evidence about several interventions from
training regimens for SUI women. Secondly, improving PFM
many trials in one analysis, producing comparisons between
strength is thought to build up long-lasting structural support
all pairs of interventions, including those which have not been
of the pelvis by elevating the levator plate to a higher location in
directly compared in any trial.18 The Cochrane Incontinence
the pelvis: this is also enhanced by hypertrophy of the muscles
Group’s Specialised Trials Register and the reference lists of
which will increase the stiffness of the PFMs and connective
relevant articles were searched (up to June 2008). Randomized
tissues.20 Thus, improving PFM strength could prevent perineal
and quasi-randomized trials where more than 50% of partic-
descent during increased intra-abdominal pressure and facil-
ipants had SUI were eligible. The primary outcome measures
itate PFM before and during effort, thereby reducing SUI in
were (1) cure and (2) improvement of the symptoms of SUI.
women. Given the above biological rationale, when treating SUI
These outcomes were measured in the trials as either patient-
the focus of any PFM training should be to improve the timing
reported (where available), or clinician-reported (as a proxy for
(of the contraction relative to a stressor), strength, and stiffness
the patient-reported outcome when this was not reported).
Eighty-eight trials were identified (9,721 women).18 The
mixed treatment comparison analysis compared 14 interven-tions (including “no active treatment”) and included data from55 trials (6,608 women) that reported cure or improvement. PFM DYSFUNCTION LITERATURE IN WOMEN WITH SUI
Interventions were on average more effective than no treat-ment. Further, there was clear evidence that PFM training either
Further to the biological rationale, a growing body of liter-
with extra sessions (more than 2 per month) or combined with
ature focuses on the differences in PFM function in continent
biofeedback, was better than no treatment, for cure of incon-
and SUI women. Using instruments such as dynamometers,
tinence, while a basic frequency of PFM training sessions (2
which can provide direct measurements of PFM function (mus-
or less per month) was not. Vaginal cones, bladder training,
cle tone, strength, coordination, and endurance), and other
PFM training with electrical stimulation and PFM training with
innovative technologies such as ultrasound (US) and magnetic
both bladder training and biofeedback were also more likely
resonance imaging (MRI), these studies have provided a unique
Neurourology and Urodynamics DOI: 10.1002/nau
Optimal Training For Women With Stress Incontinence
TABLE II. PFM Training Programs From RCTs Comparing Different Programs
Course: sets of 8--12 VPFMC with 6--8 sec
rest, 3 times a day, at least 3 days a week
VPFMC with 1--2 sec hold, 4 daysweekly + Knack
contraction for 6- 8 sec with feet crossed
at the ankles. 3 sets of long and 2 sets of
Neurourology and Urodynamics DOI: 10.1002/nau
TABLE II. (Continued )
PFMT: 1/4 (25%)Modified pilates: 3/6 (50%)RR 0.5 (95% CI: 0.08--3.27),
Supine PFMT: 12/22 (55%)Different position PFMT:
Standard care: given a leaflet + 4 clinic
Standard care: 53/75 (71%)RR 0.86 (95% CI: 0.69--1.09),
contractions daily in lying, sitting, and
PFM, pelvic floor muscle; VPFMC, voluntary PFM contraction; PFMT, PFM training; HP, health professional; Set, one episode or sequence of PFM contractions ortraining, including length of time of holding contraction, positions while performing contractions and number of repetitions of contractions. Neurourology and Urodynamics DOI: 10.1002/nau
Optimal Training For Women With Stress Incontinence
Fig. 1. Mixed treatment comparison: odds ratio for cure of urinary incontinence for each treatment versus no treatment. Posterior distributors median (circle) with 95% central credible intervals. The horizontal axis is plotted on the log scale. PFMT basics: ≤2 sessions per month; PFMT basics: >2 sessions per month; VC, vaginal cones; SNRI, Duloxetine; BF, biofeedback; BT, bladder training; ES, electrical stimulation.
way of studying PFM function, displacement, and morpholog-
nal support to the urethra, reducing displacement, velocity, and
ical integrity in continent women versus those with SUI. Such
acceleration. In women with SUI, this PFM pre-contraction did
studies have already increased our understanding of SUI patho-
not occur; consequently, the urethras of women with SUI had to
physiology, determined the causes of functional abnormalities,
move further and faster for a longer duration.
and might, in future, enable us to identify and better tailor PFM
Finally, using MRI, Hoyte25 found differences between conti-
training regimens to SUI women. Some examples include:
nent and SUI women in terms of the position of the levator plate
In a cohort study evaluating PFM function in 59 pre-
at rest, which is indicative of stiffness; the levator plate being
menopausal women, using dynamometry, Morin et al.21
demonstrated that incontinent women as compared to con-
All these findings indicate that PFM function is deficient in
tinent women had lower passive force at rest (muscle tone),
SUI women at rest (in terms of tone and stiffness), during
showed lower endurance, and were unable to produce as many
a maximal voluntary contraction (maximal strength, rapid-
rapid contractions in 15 sec; indicative of PFM dysfunction at
ity, and endurance), and during effort (timing and maximal
rest and during an active contraction.
strength). Therefore, PFM assessments could be used to identify
In another study by the same author, which evaluated PFM
which aspects of structure or function are deficient; subsequent
function in 34 continent women and 33 post-menopausal
training regimens could then be designed to address these dys-
women with SUI, incontinent women showed a reduction of
functions by using a diversity of exercises, possibly tailored
the PFM involuntary response during a maximal cough such as
to individual women’s abilities. Ultimately, the development
a lower PFM-contraction rapidity, a decrease in maximal PFM
of clinical prediction rules based on such assessments could
force, and a reduction of the PFM force measured at peak max-
improve clinical practice, enabling SUI women to be matched
imum intra-abdominal pressure. This indicates abnormalities
to the optimal intervention for their condition.
in the involuntary responses of the PFM during coughing inwomen with SUI.22
Conversely, Verelst and Leivseth,23 in a study evaluating PFM
function using dynamometry on 26 control and 20 SUI parous
SKELETAL MUSCLE TRAINING THEORY AS PROGRESSIVE
women, concluded that normalized strength differed between
OVERLOAD
continent and SUI women; the incontinent women had weakerPFMs.
The American College of Sports Medicine recently issued a
Further, in Lovegrove et al.24 used US to characterize the dis-
special communication on evidence-based progression models
placement, velocity, and acceleration of the PFM during a cough
for resistance training in healthy adults.26 These recommen-
in 23 asymptomatic and 9 SUI women. They found that dur-
dations could be used to elaborate exercise regimen protocols
ing a cough, PFM activation in continent women produced a
aimed at improving timing, strength, and stiffness. The arti-
timely compression of the PFMs and provided additional exter-
cle sets out the basic principles, including progressive overload,
Neurourology and Urodynamics DOI: 10.1002/nau
specificity, and periodization, that need to be incorporated into
ing into their lives using either a routine or ad hoc approach.
any resistance-training programme in order to achieve maxi-
Those participants who used a routine approach were 12 times
more likely (than those employing an ad hoc approach) to have a
PFM training regimens should also adhere to these principals.
high adherence level at 3 months (OR = 12.4, 95% CI = 4.0--38.8,
For example, in relation to PFM training, progressive overload
P < 0.001) and were significantly more likely to have maintained
implies that the intensity of the exercises and the number of
that level 12 months post-intervention (OR = 2.7, CI = 1.2--6.0,
repetitions should be gradually increased throughout the exer-
P < 0.014). Practicing bladder training was also related to high
cise programme, the speed or tempo of the repetitions with
submaximal loads should be adjusted according to the desired
Finally, two trials have investigated the use of adherence
goal (i.e., to train for either endurance or strength), the rest peri-
strategies as a means of rendering PFM training more effec-
ods should be shortened for endurance-improvement training
tive in women with SUI. In both trials, two groups followed the
or lengthened for strength and power training, and, finally, the
same daily home-based PFM training programme, but one was
overall volume of training should be increased gradually.
provided with an adherence strategy.30,31 In the Sugaya study,
Further, in order to increase muscle strength, the progression
participants were provided with a device emitting a rhyth-
model suggests using a repetition range of 8--12 maximum con-
mic beep, signaling them to undertake a contraction; they also
tractions at moderate velocity, a 1- to 2-min rest between sets,
pressed a button on the device to record each contraction.30
an initial training frequency of 2--3 times per week progressing
Participants in the Gallo study were given an audiotape of
to 4--5 times, and the application of a 2--10% increase in load
exercise instructions that counted out 25 consecutive PFM
when an individual can perform the current workload for 1--2
contractions.31 Participants who used the beeping device to
repetitions over the targeted number.
cue PFM contractions were more compliant and more likely
For endurance training, the progression model suggests the
to be satisfied with the treatment outcome, compared to the
need for light to moderate loads (40--60% of maximal load)
control group (RR 3.17, 95% CI: 1.02--9.88).30 Those who used
with high repetitions (>15) and short rest periods (<90 sec). In
the audiotape of exercise instructions were more likely to per-
PFM training this can be achieved by changing positions from
form the exercises twice daily, as per instruction (RR 7.05; 95%
gravity-free to anti-gravity (i.e., from lying to sitting to standing)
CI: 2.78--17.88).31 Whether these adherence strategies impact
or through the introduction of cones into the exercise sessions.
on objective continence outcomes remains inconclusive, as the
Finally, rapidity and coordination training (“The Knack”)
results were not significant in Sugaya’s study and impact was
would include the use of repetitive, voluntary PFM contrac-
tions in response to specific situations; for example, prior to
Interestingly, the ability to incorporate an exercise regime
and during coughing, lifting an object, or jumping.
into one’s daily routine or using an adherence strategy wereboth facilitators for adherence to the home-based exerciseprogramme, including its continuation post-treatment. Resultsfrom these studies should be taken into consideration whendefining protocols for PFM training regimens to achieve optimal
TYPES OF BEHAVIOR AND ADHERENCE STRATEGIES FOR
participation during training, at home and, most importantly,
EFFECTIVE PFM TRAINING
A few studies have examined factors that impact on women’s
participation in and adherence to a PFM training regimenduring treatment (in class and at home), as well as in the long-term, post-treatment.27--29 In a qualitative descriptive study
CONCLUSION
using individual and focus-group interviews, In 2006, Milneand Moore27 studied the self-care strategies employed by
PFM training has been shown to be effective in treating SUI in
community-dwelling individuals to adhere to the PFM train-
women. However, to date there are only limited indications as
ing regimen at home. Factors that facilitated home-based PFM
to which type of PFM training is the most effective. While super-
training included realistic goals and expectations, positive affir-
vised PFM training which is delivered more often (more than 2
mations, follow-up, and a regular exercise routine. Barriers
sessions per month) or augmented with biofeedback appear to
noted were insufficient information about the exercise, the
be more effective, data and hence consensus are lacking as to
characteristics of the exercises, competing interests, financial
which elements of a PFM training regimen are most effective,
such as the strength and duration of the muscle contractions,
In 2007, Martin and Dumoulin28 also studied factors that
the type of training employed, the number of contraction rep-
facilitate or impede the participation of women with UI in a
etitions used, the positions in which exercises are performed,
weekly PFM-exercise classes and their adherence to a daily,
the inclusion or exclusion of the use of ancillary muscles
home-based PFM exercise programme. Four facilitating fac-
(such as abdominal ones), and the treatment session approach
tors in terms of participation in a weekly PFM exercise classes
(e.g., individual versus a class approach), among many others.
were identified: a desire to reduce UI, a sense of responsibility
Moreover, factors and treatment strategies that affect compli-
towards the programme, close supervision by a physiother-
ance and long-term adherence are only just beginning to be
apist, and group support. Impediments were illness, medical
appointments, and planned social activities. Facilitators for the
It is no longer a question of whether PFM training pro-
home-based PFM exercise programme were a desire to reduce
grammes work but what components (including adjunct
UI and commitment to making exercises part of a daily routine.
therapies) and combinations thereof are most effective. Nor
Impediments were a busy schedule, the length of the exercise
can PFM training be studied without due consideration of
PFM dysfunction, resistance training and adherence factors
Hines et al.29 conducted a survey 1-year post-treatment of
and strategies, derived from physiological theory and innova-
164 community-dwelling, post-menopausal women to identify
tive technological investigations. Future RTCs which incorporate
predictors of long-term adherence to PFM and bladder training
methods and strategies that have been shown to be effective,
exercises. Results indicated that women incorporated PFM train-
both for treatment for and to encourage long-term adherence,
Neurourology and Urodynamics DOI: 10.1002/nau
Optimal Training For Women With Stress Incontinence
are needed to address some of the uncertainties in how best to
14. Zanetti MR, Castro RA, Rotta AL, et al. Impact of supervised physiotherapeutic
pelvic floor exercises for treating female stress urinary incontinence. Sao Paulo
PFM training programmes work but the how and for whom is
15. Bo K, Hagen RH, Kvarstein B, et al. Pelvic floor muscle exercise for the treatment
still ill understood. In order to improve treatment for SUI women
of female stress urinary incontinence: III. Effects of two different degrees of
more studies in the following areas are required:
pelvic floor muscle exercises. Neurourol Urodyn 1990;9:489--502.
16. Konstantinidou E, Apostolidis A, Kondelidis N, et al. Short-term efficacy of
1. Which PFM components impact, and to what degree, on the
group pelvic floor training under intensive supervision versus unsupervisedhome training for female stress urinary incontinence: a randomized pilot study.
success of PFM training: strength and duration of the mus-
cle contractions, number of contraction repetitions, exercise
17. Wong KS, Fung BKY, Fung ESM, et al. Randomized prospective study of the
positions, inclusion or exclusion of ancillary muscles, and
effectiveness of pelvic floor training using biofeedback in the treatment of gen-
individual versus group treatment approach?
uine stress urinary incontinence in Chinese population (Abstract). Proceedingsof the International Continence Society (ICS), 27th Annual Meeting, 1997 Sep
2. Do adjunct therapies make PFMT more effective; and is
success really linked to frequency of contact with health
18. Imamura M, Abrams P, Bain C, et al. Systematic review and economic
modelling of the effectiveness and cost-effectiveness of non-surgical treat-
3. Which clinical and patient-specific characteristics determine
ments for women with stress urinary incontinence. Health Technol Assess2010;14:97--108.
the effectiveness and acceptability of PFM training?
19. Miller JM, Ashton-Miller JA, DeLancey JOL. A pelvic muscle precontraction can
4. Which, if any, PFM assessment indicators best predict
reduce cough-related urine loss in selected women with mild SUI. J Am Geriatr
patient-specific outcomes enabling clinicians to better
match women to the optimal intervention for their condi-
20. Bø K. Pelvic floor muscle training is effective in treatment of female stress uri-
nary incontinence, but how does it work? Int Urogynecol J Pelvic Floor Dysfunct
5. Which physiological and psychological factors and/or
21. Morin M, Bourbonnais D, Gravel D, et al. Pelvic floor muscle function in
treatment strategies influence compliance and long-term
continent and stress urinary incontinent women using dynamometric mea-
surements. Neurourol Urodyn 2004;23:668--74.
22. Morin M, Dumoulin C, Gravel D, et al. Reliability of speed of contraction and
endurance dynamometric measurements of the pelvic floor musculature instress incontinent parous women. Neurourol Urodyn 2007;26:397--403, discus-sion 404.
23. Verelst M, Leivseth G. Force and stiffness of the pelvic floor as function of mus-
REFERENCES
cle length: a comparison between women with and without stress urinaryincontinence. Neurourol Urodyn 2007;26:852--7.
1. Hay Smith J, Berghmans B, Burgio B, et al. Adult conservative management in
24. Lovegrove Jones RC, Peng Q, Stokes M, et al. Mechanisms of pelvic floor-
Incontinence, 4th edition. P. Abrams, L. Cardozo, S. Khoury, A. Wein (Eds.). 2009;
musclefunction and the effect on the urethra during a cough. Eur Urol
2. Dumoulin C, Hay Smith J. Pelvic floor muscle training versus no treatment,
25. Hoyte L, Schierlitz L, Zou K, et al. Two- and 3-dimensional MRI comparison of
or inactive control treatments, for urinary incontinence in women. Cochrane
levator ani structure, volume, and integrity in women with stress incontinence
and prolapse. Am J Obstet Gynecol 2001;185:11--9.
oder A, Abrams P, Andersson KE, et al. Incontinence in women. Guidelines
26. Ratamess NA, Alvar BA, Evetoch T, et al. American College of Sports Medicine
on urinary incontinence. Arnhem, The Netherlands: European Association of
Position stands—progression models in resistance training for healthy adults.
Med Sci Sports Exerc 2009;41:687--708.
4. Lucas M, Bosch R, Cruz F, et al. 2010. Addendum to 2009 urinary incontinence
27. Milne JL, Moore KN. Factors impacting self-care for urinary incontinence. Urol
guidelines. Arnhem, The Netherlands: European Association of Urology (EAU);
28. Martin C, Dumoulin C. Factors impacting incontinent women’s participation to
5. Buckley BS, Grant AM, Tincello DG, et al. Prioritizing research: patients, carers,
a pelvic floor muscle exercise class and home program. Abstract book, World
and clinicians working together to identify and prioritize important clinical
Congress of Physical Therapy (WCPT), Vancouver. 2007.
uncertainties in urinary incontinence. Neurourol Urodyn 2010;29:708--14.
29. Hines SH, Seng JS, Messer KL, et al. Adherence to a behavioral program to
6. Johnson VY. Effects of a submaximal exercise protocol to recondition the pelvic
prevent incontinence. West J Nurs Res 2007;29:36--56, discussion 57--64.
floor musculature. Nurs Res 2001;50:33--41.
30. Sugaya K, Owan T, Hatano T, et al. Device to promote pelvic floor muscle training
7. Hay-Smith EJ. Pelvic floor muscle training for female stress urinary inconti-
for stress incontinence. Int J Urol 2003;10:416--22.
nence [PhD]. Dunedin, NZ: University of Otago Department of Physiotherapy;
31. Gallo ML, Staskin DR. Cues to action: Pelvic floor muscle exercise compliance in
women with stress urinary incontinence. Neurourol Urodyn 1997;16:167--77.
8. Dumoulin C, Morin M, Lemieux MC, et al. Efficacy of deep abdominal train-
32. Bo K, Talseth T, Holme I. Single blind, randomised controlled trial of pelvic floor
ing when combined with pelvic floor muscle training for stress urinary
exercises, electrical stimulation, vaginal cones, and no treatment in manage-
incontinence: a single blind randomized controlled trial. Proceedings of the
ment of genuine stress incontinence in women. BMJ 1999;318:487--93.
3rd International Consultation on Incontinence. Monaco Progr`es Urol 2004;
33. Aksac B, Aki S, Karan A, et al. Biofeedback and pelvic floor exercises for the reha-
bilitation of urinary stress incontinence. Gynecol Obstet Invest 2003;56:23--7.
9. Borello-France DF, Zyczynski HM, Downey PA, et al. Effect of pelvic-floor muscle
34. Yoon HS, Song HH, Ro. YJ. A comparison of effectiveness of bladder training
exercise position on continence and quality-of-life outcomes in women with
and pelvic muscle exercise on female urinary incontinence. Int J Nurs Stud
stress urinary incontinence. Phys Ther 2006;86:974--86.
10. Ramsay IN, Thou M. A randomised, double blind, placebo controlled trial of
35. Burns PA, Pranikoff K, Nochajski TH, et al. A comparison of effectiveness of
pelvic floor exercises in the treatment of genuine stress incontinence (Abstract).
biofeedback and pelvic muscle exercise treatment of stress incontinence in
older community-dwelling women. J Gerontol 1993;48:M167--74.
11. Ghoniem GM, Van Leeuwen JS, Elser DM, et al. A randomized controlled trial
36. Henalla SM, Hutchins CJ, Robinson P, et al. Non-operative methods in the
of duloxetine alone, pelvic floor muscle training alone, combined treatment
treatment of female genuine stress incontinence of urine. J Obstet Gynaecol
and no active treatment in women with stress urinary incontinence. J Urol
37. Castro RA, Arruda RM, Zanetti MR, et al. Single-blind, randomized, controlled
12. Savage AM. Is lumbopelvic stability training (using the Pilates model) an effec-
trial of pelvic floor muscle training, electrical stimulation, vaginal cones, and
tive treatment strategy for women with stress urinary incontinence? A review
no active treatment in the management of stress urinary incontinence. Clinics
of the literature and report of a pilot study. J Assoc Chartered Physiother
(Sao Paulo, Brazil) 2008;63:465--72.
38. Kim H, Suzuki T, Yoshida Y, et al. Effectiveness of multidimensional exercises for
13. Williams KS, Assassa RP, Gillies CL, et al. A randomized controlled trial of
the treatment of stress urinary incontinence in elderly community-dwelling
the effectiveness of pelvic floor therapies for urodynamic stress and mixed
Japanese women: a randomized, controlled, crossover trial. J Am Geriatr Soc
incontinence. BJU Int 2006;98:1043--50. Neurourology and Urodynamics DOI: 10.1002/nau
Votre médecin vous a prescrit une coloscopie. Afin que vous soyez parfaitement informé(e) sur l’examen, ses indications, sa préparation indispensable, etc., nous avons rédigé le document qui suit. Si vous avez encore des questions ou des inquiétudes après sa lecture, n’hésitez pas en parler aux médecins et infirmières de gastro-entérologie. Le jour de votre coloscopie, nous vous dem
Anesth Pain Med. 2011 July; 1(1): 10–14. Research Article Comparison of the Efficacy of Adding Clonidine, Chlorpromazine, Promethazine, and Midazolam to Morphine Pumps in Postoperative Pain Farnad Imani 1; Poupak Rahimzadeh 1,*; Seyyed Hamid Reza Faiz 21Department of Anesthesiology and Pain Medicine, Rasoul-Akram Medical Center, Tehran University of Medical Sciences, Tehran, IR Iran2Depar
 Neurourology and Urodynamics 30:746–753 (2011)
Determining the Optimal Pelvic Floor Muscle Training Regimen
Neurourology and Urodynamics 30:746–753 (2011)
Determining the Optimal Pelvic Floor Muscle Training Regimen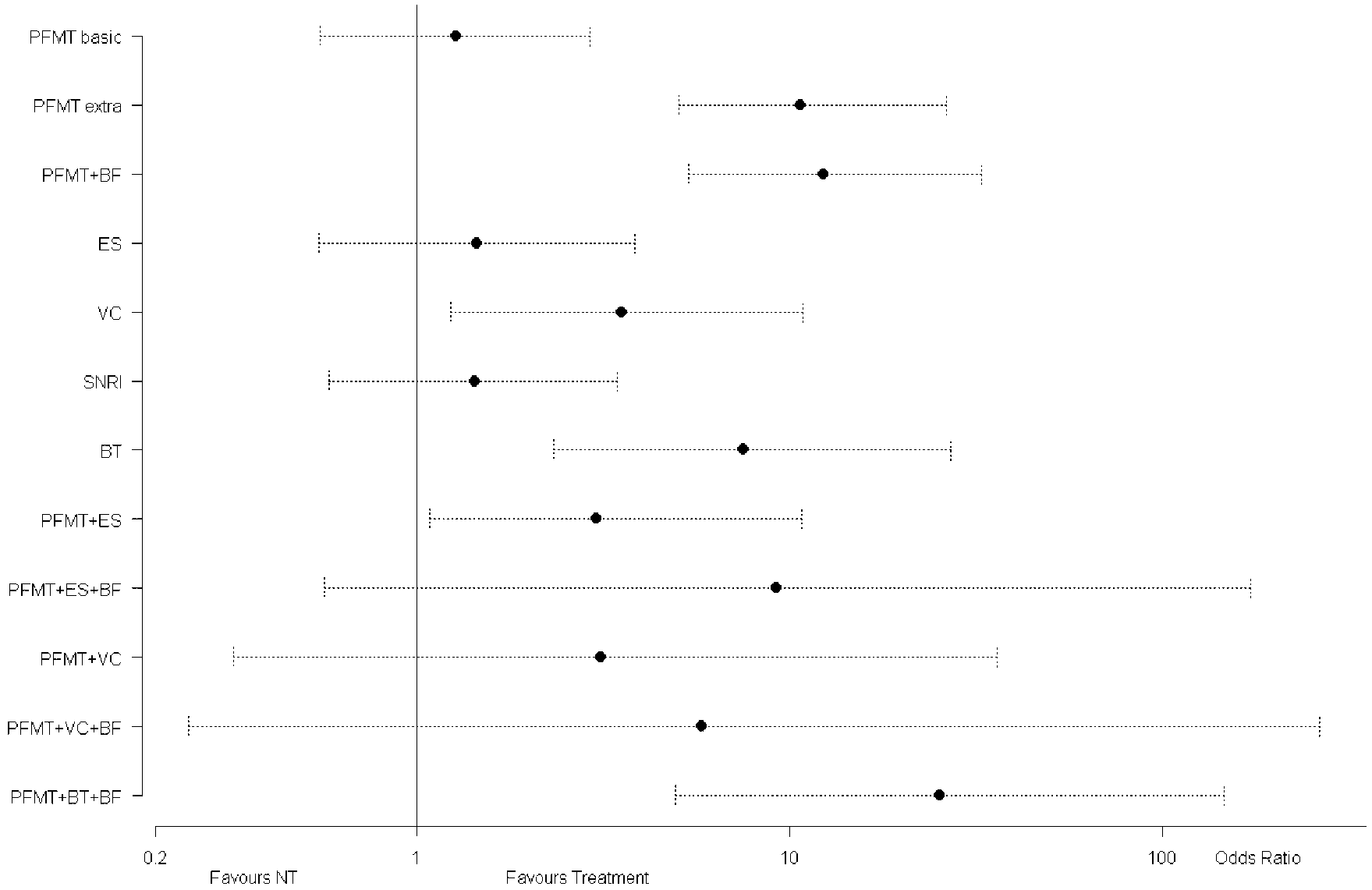 Optimal Training For Women With Stress Incontinence
Fig. 1. Mixed treatment comparison: odds ratio for cure of urinary incontinence for each treatment versus no
Optimal Training For Women With Stress Incontinence
Fig. 1. Mixed treatment comparison: odds ratio for cure of urinary incontinence for each treatment versus no