Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
Case presentation_ringelstein_7_en.indd
Case Presentation Optical Coherenc Tomography (OCT) in Susac´s syndrome
Marius Ringelstein, MD Resident Neurologist, Dr. med., MD Molecular Neurology Research Group (Head: Prof. O. Aktas), Department of Neurology (Chairman: Prof. H.-P. Hartung), Heinrich-Heine-University, Medical Faculty, Düsseldorf, Germany
A 19-year old previously healthy woman presented with disturbances of memory and orientation, inadequate behaviour and lethargy developing gradually over a period of 2 weeks after a car accident in 2005. She showed substantial neuro-psychological defi cits and a mild left-arm paresis as well as gait ataxia in the neurological examination. A cranial MRI revealed multiple infl ammatory periventricular T2-lesions with thalamic and cerebellar involvement and in close relati-on to the corpus callosum. The cerebrospinal fl uid showed a mild pleocytosis and negative oligoclonal bands. In 2007 the patient experienced an acute hearing loss in her right ear. Audiometry revealed bilateral hearing loss, predominantly of low frequencies. In 2008 she complained of noticeable painless scotoma on the left, a few weeks later, also on the right eye.
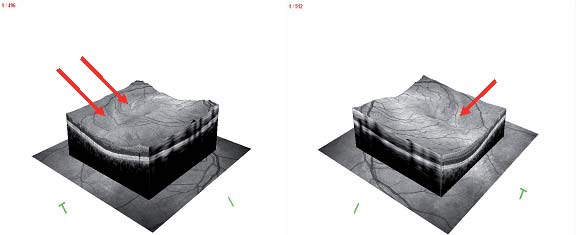
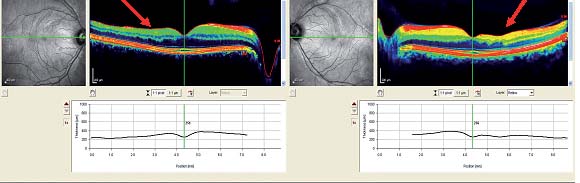
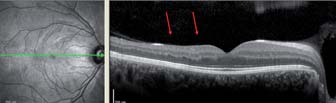
A Spectral-Domain OCT device (SPECTRALIS® OCT with Nsite Axonal Analytics™; Heidelberg Engineering) was used to obtain perifoveal volumetric macula scans consisting of 25 single horizontal axial scans (scanning area: 6 x 6 mm, Figure 1). Furthermore a single high-resolution horizontal scan through the middle of the fovea to evaluate the deeper retinal layers (Figure 2) and a circular scan with a diameter of approximately 3.4 mm (1536 A-scans) to assess the peripapillar retinal nerve fi ber layer (RNFL), were performed (Figure 3). Figure 1 Perifoveal volumetric macular scan of the right (OD) and left eye (OS). Figure 2 Single high-resolution horizontal scan through the middle of the fovea of OD and OS. Figure 3 Circular scan to assess the peripapillar retinal nerve fi ber layer (RNFL) of OD and OS.
The OCT volume scan in fi gure 2 shows a marked reduction of the total macular volume. The inner retinal layers (e.g. the ganglion cell layer) and the RNFL (red arrows) show thinning in different sectors that are not evenly distributed over the posterior pole. Areas of choroidal infarction are indicated by yellow arrows in the fundus images. These Local retinal strokes are caused by branch retinal artery occlusions (BRVO) detectable by fl uorescent angiography (not shown here).
In 2005 an acute demyelinating encephalomyelitis (ADEM) was suspected due to the cranial MRI results and CSF fi n-dings and the patient was successfully treated with i.v. steroids. After the unilateral hearing loss with bilateral audiome-tric pathologies in 2007 peripheral otogenic dysfunction was diagnosed and was again successfully treated with steroids. Suffering from bilateral scotoma in 2008 retinal fl uorescence angiography showed bilateral branch retinal artery occlu-sion (BRAO), multifocal leakage of fl uorescence dye, and choroidal infarctions. A vasculitic process was assumed. Visual fi eld defects partially improved on i.v. steroid pulse.
The patient‘s fi nal diagnosis in 2009 was Susac‘s syndrome (SS), a rare microangiopathy affecting the precapillary arteri-oles of the brain, retina and inner ear, presumably resulting from an autoimmune endotheliopathy. The typical clinical triad reveals subacute encephalopathy with confusion, amnesia and headache, scotoma and uni- or bilateral hearing loss.
The patient was treated with azathioprine (150 mg/d), prednisolone (10/d) and acetylsalicylic acid (100 mg/d) but still experienced relapsing scotoma on both eyes every 6 months. Since 2010 she is relapse-free on a treatment with myco-phenolate mofetil, in combination with i.v. immunoglobulins every 4 weeks, and acetylsalicylic acid 100 mg daily.
Painless Scotoma as index event in young patients (female male ratio 3:1), or in combination with a history of subacute encephalopathy and/or uni- or bilateral hearing loss should prompt our attention to Susac‘s syndrome. Spectral domain-OCT can help to accurately identify location and extend of retinal infarction. Moreover, fl uorescence angiography can visualize a capillary leakage, particularly in the acute phase. Due to some overlap in the clinical presentation and the patterns of MRI fi ndings, optic neuritis and multiple sclerosis (MS) are often considered in patients with Susac‘s syn-drome. Even though the median age and female preponderance are similar in both diseases, brain MRI of patients with Susac’s syndrome may show typical callosal “snow ball” like lesions (Susac et al. J. Neurol. Sci 2006) and CSF oligoclonal bands are usually absent. In contrast to optic neuritis (ON) visual impairment is painless in Susac’s syndrome. OCT shows substantial retinal atrophy scattered over different areas of the posterior pole in patients with Sucac‘s syndrome. Fluorescence angiography reveals bilateral BRAO, fi ndings not seen in ON.
SPECTRALIS HRA and SPECTRALIS OCT are registered trademarks of Heidelberg Engineering GmbH.
www.HeidelbergEngineering.com
Copyright 2004 by the Genetics Society of AmericaDOI: 10.1534/genetics.104.026716 Virulence, Multiple Infections and Regulation of Symbiotic Population in the Wolbachia -Asobara tabida Symbiosis Laurence Mouton,*,1 Franck Dedeine,*,† He´le`ne Henri,* Michel Boule´treau,* Ne´rina Profizi‡ and Fabrice Vavre* * Laboratoire de Biome´trie et Biologie Evolutive (UMR-CNRS 5558)
Prof. Dr. Lorenz, Günter Forschungsschwerpunkt Intelligente Produkte, Prozesse und Services Forschungsgebiete Reaktive Extrusion Biomaterialien Oberflächenmodifizierung Netzwerke Fachbeirat Ingenieurwerkstoffe des VDI Leistungsangebot Polymersynthese im Technikumsmaßstab mittels Reaktiver Extrusion Anpassung von Polymereigenschaften an Prozesse und Anwendung Polymerc




 Case Presentation Optical Coherenc Tomography (OCT) in Susac´s syndrome
Marius Ringelstein, MD
Case Presentation Optical Coherenc Tomography (OCT) in Susac´s syndrome
Marius Ringelstein, MD 
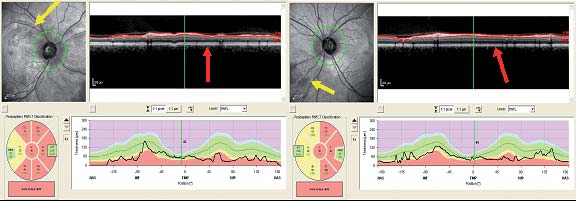 Figure 3
Figure 3