Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
Clinical course of sepsis in children with acute leukemia admitted to the pediatric intensive care unit
Clinical course of sepsis in children with acute leukemia admitted to the pediatric intensive care unit*
Kanakadurga Singer, MD, MA; Perla Subbaiah, PhD; Raymond Hutchinson, MD;Folafoluwa Odetola, MD, MPH; Thomas P. Shanley, MD
Objective: To describe the clinical course, resource use, and inotropic and/or vasopressor drugs (p ؍ .01), and renal replace- mortality of patients with leukemia admitted to the pediatric ment therapy (p ؍ .028) than nonsepsis admission. There was intensive care unit with sepsis and nonsepsis diagnoses over a higher mortality among children with sepsis than other diagnoses 10-yr period. (52% vs. 17%, p ؍ .004). Also, mortality among children with Design: Retrospective analysis. sepsis was higher among those with acute lymphoblastic leuke- Setting: Tertiary medical–surgical pediatric intensive care unit mia (60% vs. 44%) compared with acute myelogenous leukemia. at C.S. Mott Children’s Hospital, University of Michigan. Administration of stress dose steroids was associated with higher Patients: All patients with leukemia admitted to the pediatric mortality (50% vs. 17%, p ؍ .005) and neutropenia. Patients with intensive care unit from January 1, 1998, to December 31, acute lymphoblastic leukemia and sepsis showed the greatest mortality and resource use. Interventions: None; chart review. Conclusions: Patients with acute leukemia and sepsis had a Measurements and Main Results: Clinical course was charac- much higher mortality rate compared with previously described terized by demographics, leukemia diagnosis, phase of therapy, sepsis mortality rates for the general pediatric intensive care unit leukocyte count on admission, presence of sepsis, steroid admin- patient populations. Patients who received steroids had an in- istration, intensity of care, and Pediatric Risk of Mortality score on creased mortality rate, but given the retrospective nature of this admission to the pediatric intensive care unit. The primary out- study, we maintain a position of equipoise with regard to this come was survival to pediatric intensive care unit discharge. association. Variation in mortality and resource use by leukemia Among 68 single admissions to the pediatric intensive care unit type suggests further research is needed to develop targeted with leukemia during the study period, 33 (48.5%) were admitted intervention strategies to enhance patient outcomes. (Pediatr Crit with sepsis. Admission to the pediatric intensive care unit for Care Med 2011; 12:649 – 654) sepsis was associated with greater compromise of hemodynamic KEY WORDS: sepsis; leukemia; mortality; severity of illness; and renal function and use of stress dose steroids (p ؍ .016), length of stay; natural history
Sepsisisaleadingcauseofpe- velopmentofevidence-basedguidelines targetinterventionalrandomizedcon-
limited by difficulty in performing ran-
domized controlled trials in this patient
pediatric deaths with associated signifi-
often unclear, there is current consensus
pediatric sepsis also relates to the wide
that aggressive treatment of pediatric pa-
tients with leukemia is appropriate given
current positive long-term outcomes (3). *See also p. 680.
The last reported 5-yr mortality for acute
From the Department of Pediatrics and Communi-
cable Diseases (KS, RH, FO, TPS), University of Mich-
igan Health System, Ann Arbor, MI; and the Depart-
of pediatric sepsis is to study pediatric
ment of Mathematics and Statistics (PS), OaklandUniversity, Rochester, MI.
Supplemental digital content is available for this ar-
ticle. Direct URL citations appear in the printed text and
are provided in the HTML and PDF versions of this article
nesses, in part related to aggressive anti-
on the journal’s Web site (www.pccmjournal.org).
The authors have not disclosed any potential con-
For information regarding this article, E-mail:
(5, 6). Other related risk factors for de-
severely ill children. As such, high-risk
Copyright 2011 by the Society of Critical Care
Medicine and the World Federation of Pediatric Inten-
kemia include the use of central vascular
catheters, frequent hospitalizations, and
DOI: 10.1097/PCC.0b013e31821927f1
Pediatr Crit Care Med 2011 Vol. 12, No. 6
Data Source and Subject Identification. All
Table 1. Relapse rates among patient groups
children 0 –20 yrs of age diagnosed with leu-
kemia between January 1, 1998, and Decem-
rence in patients with leukemia, even be-
ber 31, 2008, were identified in the University
fore the occurrence of sepsis (8). Current
of Michigan Comprehensive Cancer CenterRegistry. Thereafter, their inpatient hospital-
pediatric sepsis guidelines emphasize the
ization records at the C.S. Mott Children’s
Hospital were searched for with the EMERSE
(12) search program to identify those patients
do not address specific comorbid diagno-
hospitalized in the PICU during the study pe-
riod. Patients admitted to the neonatal inten-
Study Variables. Patients with culture-
positive sepsis were identified using the fol-
lowing key terms: “sepsis,” “infection,” and
all patients with leukemia admitted to the
“culture.” To avoid potential bias toward over-
diagnosing sepsis when these broader criteria
administration of “stress” dose steroids in
75% were in initial treatment. As seen in
are used, we decided a priori to report only on
addition to the mainstay of broad-spectrum
culture-positive sepsis to avoid potential cap-
Table 1, most of the patients with relapse
antibiotic therapy. For instance, during in-
ture of patients exhibiting a systemic inflam-
matory response as a result of nonspecific trig-
there is often administration of high doses
gers other than systemic infection (e.g.,
group. Of the 68 patients admitted to the
of steroids with subsequent risk for adrenal
adverse reaction to chemotherapy, viral upper
insufficiency. On the other hand, patients
respiratory illness, etc.) that is common in
sepsis by clinical symptoms and a positive
with AML do not typically receive steroids
this cohort. Furthermore, given the retrospec-
blood culture with bacteria (Enterobacter,
during induction therapy and are expected
tive nature of the study, it was not possible to
Pseudomonas, Klebsiella, Enterococcus,
ensure accurate identification of “culture-
to be at lower risk of adrenal suppression.
coagulase-positive Staphylococcus, Strep-
negative” sepsis patients on the basis of clini-
Knowledge of the outcomes of patients sub-
tococcus), viruses (cytomegalovirus, para-
cal judgment by the medical team. Data col-
jected to steroid therapy is, however, very
influenza), and fungi (Aspergillus, Can-
demographic information (age, gender, length
dida). Fifteen of the 33 patients with sepsis
of PICU stay, source of admission), leukemia
these patients has long been debated (10).
diagnosis (ALL or AML), phase of therapy,
35 patients without sepsis were diagnosed
Specific studies have not been performed
white blood cell count on admission, and in-
tensity of PICU care. Indicators of the intensity
admissions were for a variety of reasons,
of care included use of mechanical ventilation,
including 11% gastrointestinal, 11% post-
mia impact outcomes from sepsis (11).
arterial catheterization, central venous cathe-
therapy, use of inotropic and/or vasopressor
in children with leukemia and the overall
agents, and fluid resuscitation. Severity of pa-
high mortality in patients with leukemia,
tient illness was further characterized by the
No significant differences were observed
we conducted a retrospective study to in-
Pediatric Risk of Mortality (PRISM) score on
in age, gender distribution, or length of
vestigate the clinical course among crit-
admission to PICU when available (13). The
stay among patients according to the diag-
ically ill children with leukemia accord-
primary outcome variable of the study was
survival to PICU discharge or death. Statistical Analysis. Continuous variables
no sepsis. We present a large case series
are presented as median values and categorical
variables as frequencies. Comparisons among
multiple groups of continuous variables were
pediatric intensive care unit at C.S. Mott
other intensive care units within the study
made using the Kruskal-Wallis test. Compari-
Children’s Hospital at the University of
hospital, referring hospitals, emergency de-
sons of proportions were made using Fisher’s
exact test. A p value of .05 was taken as the
threshold for statistical significance. Calcula-
tions were performed on the Minitab software
formulate a description of clinical course
platform (Minitab 15, Minitab Inc., State Col-
PICU resource use to try to identify fac-
tors that could be used for potential treat-
individual inpatients carried the diagno-
MATERIALS AND METHODS
sis of acute leukemia and 68 of these were
Subjects. A retrospective analysis with
medical chart review was performed. Approval
for the study was obtained from the institu-
tional review board of the University of Mich-
Pediatr Crit Care Med 2011 Vol. 12, No. 6
Table 2. Patient characteristics
ED, emergency department; OSH, outside hospital.
Tables 3 and 4 [see Supplemental DigitalContent 1, http://links.lww.com/PCC/A33]). There was a significantly higher medianwhite blood cell count in patients with AMLwithout sepsis compared with all othergroups (p ϭ .009; Kruskal-Wallis test) asshown in Table 2. Intensive Care Unit Course. To better
characterize the intensity of illness andrequisite care in the PICU, use of PICUresources was compared among patientswith and without sepsis. There were nosignificant differences in the use of me-chanical ventilation, arterial catheteriza-tion, central venous catheterization, orfluid resuscitation among patients withand without sepsis (Table 4). However, agreater proportion of patients with sepsisreceived inotropic and/or vasopressoragents (p ϭ .001), stress dose steroids
Figure 1. Median length of stay of patients admitted to the pediatric intensive care unit (PICU). ALL,
(p ϭ .016), and continuous renal replace-
acute lymphocytic leukemia; AML, acute myelogenous leukemia.
ment therapy (p ϭ .028). This suggeststhat although there was significant ill-ness in both groups, the sepsis group had
penic patients in the sepsis group (19 of
portions of neutropenic patients in the sub-
with sepsis was significantly higher than
of 34 [41%]) is not statistically significant
(p ϭ .218, Fisher’s exact test). In assess-
significantly different (Supplemental Table
17%, p ϭ .0044). This increased mortal-
ity and significant differences in use of
basis of receiving received steroids or not
portions of neutropenic patients in the four
dant with their increased severity of ill-
ceived steroids and were septic (17 of 24
also significantly associated with mortal-
group eight of 15 [53%], sepsis death group
ity (p ϭ .004). This relationship appeared
with the other subclasses with neutropenia.
11 of 17 [65%]) are homogeneous (p ϭ
The proportions of neutropenic patients in
.226, chi-square test). Similarly, the pro-
sepsis, although it was not statistically
portions of neutropenic patients in the four
significant (Table 5). Similar associations
sepsis (non sepsis nonsteroid group ten of
20 [50%], nonsepsis steroid group four of
eight [25%], sepsis steroid group 17 of 24
[71%]) are significantly different (p ϭ .033,
(p ϭ .873, chi-square test) (Supplemental
Pediatr Crit Care Med 2011 Vol. 12, No. 6
Table 3. Distribution of patients in subgroups of steroid use, neutropenia, and death
NN, not neutropenic; N, neutropenic; ND, not death; D, death. aIn both the nonsepsis/steroid group and sepsis/no steroid group, a single patient had no absolute neutrophil count data recorded and thus was not
Table 4. Comparison of intensive care unit course in patients with and without sepsis
comes of patients with acute leukemiaadmitted to the PICU at a single tertiary
care center over a 10-yr period. Patients
with leukemia who were admitted forsepsis had higher illness severity and pre-
scoring and ultimately higher death rates
than those admitted for other reasons.
The mortality rate in this specific cohort
Median Pediatric Risk of Mortality severity of illness
Median Pediatric Risk of Mortality-predicted mortality
much broader, heterogeneous population(1, 8, 14). Studies of severe sepsis havereported higher mortality rates (17%),
Table 5. Mortality rates among patients receiving
steroids during the intensive care unit course
that rate (15, 16). This subgroup mortal-
ity is also much higher then the reported
and without sepsis. A significantly larger
sis received fluid resuscitation, continu-
in sepsis patients alone of 7.4% (18).
out sepsis (Table 6). Consequently, given
without sepsis, who still required inten-
sive care. Interestingly, similar differ-
without sepsis (Table 6). Interestingly, no
of illness measure was not available for all
significant differences in intensive care
require further investigation, but one po-
tential contributor this observed differ-
sepsis group, n ϭ 31 in nonsepsis group),
there was significantly increased severity
(Table 6). There were no significant dif-
of illness (p ϭ .036) and predicted mor-
tality (p ϭ .013) among patients with
mortality scores in the subgroup analysis.
pression profiles that may be activated in
sepsis vs. those without sepsis. This dif-
the setting of sepsis. A number of inves-
DISCUSSION
expression profiles with notable differ-
Pediatr Crit Care Med 2011 Vol. 12, No. 6
Table 6. Comparison of frequency of use of intensive care unit technology and outcomes among
no benefit (34) from the use of cortico-
patient subgroups with acute myelogenous leukemia and acute lymphocytic leukemia
steroids in the treatment of septic shock. It is unclear what protocol to follow in
children, and this question is the subjectof ongoing debate, but our observations
inquiry merits further investigation, par-ticularly in this high-risk cohort (35, 36).
help identify those with adrenal insuffi-
we suggest a position of clinical equipoise
with regard to the association of steroids
ciency may serve as a stratification tool. Some studies have suggested the poten-
tial association between levels of C-reac-
associated molecular patterns (19 –22).
may be as long as 4 – 8 months (26 –28).
tive protein or interleukin-8 with patient
outcomes and therefore serve as a strati-
itary–adrenal axis with the low-dose ad-
fication method for subsequent targeting
renocorticotropin test (27, 29), baseline
of therapies (39, 40). However, interleu-
leukemia cohorts may differ to influence
have focused only on adult populations.
lation were mostly in a relapse state and
their applicability to the pediatric popu-
tients with acute leukemia with sepsis for
CONCLUSIONS
that this population used more resources,
likely as a result of heightened severity of
adrenal axis suppression, the use of cor-
parison to other populations of critically
ill children with sepsis. This study sug-
ticosteroids is often prompted by a state
gests the need for further investigation of
of “relative adrenal insufficiency” in
cohort, it is also likely that PRISM may be
the differential mortality and significant
gree of physiological stress (31). Eighty-
ological progression of organ failure oc-
overall increased mortality in individuals
receiving steroid treatment, but given the
ing timeframe of the initial 24 hrs of care
steroids during hospitalization died, al-
though it is difficult to ascertain in this
maintain a position of equipoise with re-
initiated and what doses of steroids were
used. Overall, the group of patients with
roids at induction, it is possible that ALL
mortality. Formal testing for adrenal in-
tions in sepsis may lead to better patient
thalamic–pituitary–adrenal axis occurs
REFERENCES
6 – 8 wks after induction with high dose
adrenal axis, although the use of this test-
1. Watson RS, Carcillo JA: Scope and epidemi-
ology of pediatric sepsis. Pediatr Crit Care
2. Marshall JC, Vincent JL, Guyatt G, et al:
Outcome measures for clinical research in
thalamic–pituitary–adrenal axis suppres-
evidence of short-term benefit (32, 33) or
sepsis: A report of the 2nd Cambridge Collo-
Pediatr Crit Care Med 2011 Vol. 12, No. 6
quium of the International Sepsis Forum.
17. Odetola FO, Clark SJ, Dechert RE, et al:
coid therapy in children with acute lympho-
Crit Care Med 2005; 33:1708 –1716
Going back for more: An evaluation of clini-
blastic leukemia. Med Pediatr Oncol 2003;
3. Dalton HJ, Slonim AD, Pollack MM: Multi-
cal outcomes and characteristics of readmis-
sions to a pediatric intensive care unit. Pedi-
29. Rix M, Birkebaek NH, Rosthoj S, et al: Clin-
tients requiring intensive care. In: 96th In-
atr Crit Care Med 2007; 8:343–347; CEU quiz
ical impact of corticosteroid-induced adrenal
suppression during treatment for acute lym-
Thoracic Society; May 3–10, 2000. Toronto,
18. Odetola FO, Clark SJ, Gurney JG, et al: Effect
phoblastic leukemia in children: A prospec-
Canada, Taylor & Francis Inc, 2000, pp
of interhospital transfer on resource utiliza-
tive observational study using the low-dose
tion and outcomes at a tertiary pediatric in-
adrenocorticotropin test. J Pediatr 2005;
4. Linet MS, Ries LA, Smith MA, et al: Cancer
tensive care unit. J Crit Care 2009; 24:
surveillance series: Recent trends in child-
30. Silva IN, Cunha CF, Finch FL, et al: Evalua-
hood cancer incidence and mortality in the
19. Lyons PA, Koukoulaki M, Hatton A, et al:
tion of hypothalamic–pituitary–adrenal axis
United States. J Natl Cancer Inst 1999; 91:
Microarray analysis of human leucocyte sub-
recovery after corticotherapy by using basal
sets: The advantages of positive selection and
cortisol secretion [in Portuguese]. Arq Bras
5. Pancera CF, Costa CM, Hayashi M, et al:
rapid purification. BMC Genomics 2007; 8:64
Endocrinol Metabol 2006; 50:118 –124
Severe sepsis and septic shock in children
20. Feezor RJ, Baker HV, Mindrinos M, et al:
31. de Jong MF, Beishuizen A, Spijkstra JJ, et al:
with cancer [in Portuguese]. Rev Assoc Med
Whole blood and leukocyte RNA isolation for
Relative adrenal insufficiency as a predictor
gene expression analyses. Physiol Genomics
of disease severity, mortality, and beneficial
6. Hung IJ, Yang CP: Early-onset sepsis in chil-
effects of corticosteroid treatment in septic
dren with acute lymphoblastic leukemia.
21. De AK, Miller-Graziano CL, Calvano SE, et al:
shock. Crit Care Med 2007; 35:1896 –1903
J Formos Med Assoc 1996; 95:746 –753
Selective activation of peripheral blood T cell
32. Sprung CL, Annane D, Singer M, et al: Ste-
7. Hakim H, Flynn PM, Srivastava DK, et al:
subsets by endotoxin infusion in healthy hu-
roids in patients with septic shock. Chest
Risk prediction in pediatric cancer patients
with fever and neutropenia. Pediatr Infect
chemokine activation. J Immunol 2005; 175:
33. Annane D, Bellissant E, Bollaert PE, et al:
Corticosteroids in the treatment of severe
8. Odetola FO, Gebremariam A, Freed GL: Pa-
22. Kloppenburg M, Brinkman BM, de Rooij-Dijk
sepsis and septic shock in adults: A system-
tient and hospital correlates of clinical out-
HH, et al: The tetracycline derivative mino-
atic review. JAMA 2009; 301:2362–2375
comes and resource utilization in severe pe-
cycline differentially affects cytokine produc-
34. Markovitz BP, Goodman DM, Watson RS, et
diatric sepsis. Pediatrics 2007; 119:487– 494
tion by monocytes and T lymphocytes. Anti-
al: A retrospective cohort study of prognostic
9. Carcillo JA, Fields AI: Clinical practice pa-
microb Agents Chemother 1996; 40:934 –940
factors associated with outcome in pediatric
rameters for hemodynamic support of pedi-
23. Yeh TS, Pollack MM, Holbrook PR, et al:
severe sepsis: What is the role of steroids?
atric and neonatal patients in septic shock.
Assessment of pediatric intensive care—
Pediatr Crit Care Med 2005; 6:270 –274
Crit Care Med 2002; 30:1365–1378
Application of the Therapeutic Intervention
35. Aneja R, Carcillo JA: What is the rationale for
10. Dobriner K, Kappas A, Gallagher TF: Studies
Scoring System. Crit Care Med 1982; 10:
hydrocortisone treatment in children with
in steroid metabolism. XXVI. Steroid isola-
infection-related adrenal insufficiency and
tion studies in human leukemia. J Clin In-
24. Kuperman H, Damiani D, Chrousos GP, et al:
septic shock? Arch Dis Child 2007; 92:
Evaluation of the hypothalamic–pituitary–
11. Heying R, Schneider DT, Korholz D, et al:
adrenal axis in children with leukemia before
36. Zimmerman JJ: Moving beyond Babel. Pedi-
Efficacy and outcome of intensive care in
and after 6 weeks of high-dose glucocorticoid
pediatric oncologic patients. Crit Care Med
therapy. J Clin Endocrinol Metab 2001; 86:
37. Langer M, Modi BP, Agus M: Adrenal insuf-
ficiency in the critically ill neonate and child.
12. Hanauer DA: EMERSE: The Electronic Med-
25. Felner EI, Thompson MT, Ratliff AF, et al:
Curr Opin Pediatr 2006; 18:448 – 453
ical Record Search Engine. AMIA Annu
Time course of recovery of adrenal function
38. Hildebrandt T, Mansour M, Al Samsam R:
in children treated for leukemia. J Pediatr
The use of steroids in children with septice-
13. Pollack MM, Ruttimann UE, Getson PR: Pe-
mia: Review of the literature and assessment
diatric Risk of Mortality (PRISM) score. Crit
26. Einaudi S, Bertorello N, Masera N, et al:
of current practice in PICUs in the UK. Pae-
Adrenal axis function after high-dose steroid
14. Watson RS, Carcillo JA, Linde-Zwirble WT, et
therapy for childhood acute lymphoblastic
39. Hamalainen S, Kuittinen T, Matinlauri I, et
al: The epidemiology of severe sepsis in chil-
leukemia. Pediatr Blood Cancer 2008; 50:
al: Neutropenic fever and severe sepsis in
dren in the United States. Am J Respir Crit
adult acute myeloid leukemia (AML) patients
27. Mahachoklertwattana P, Vilaiyuk S, Hongeng
15. Nadel S: RESOLVE-ing sepsis in children—
S, et al: Suppression of adrenal function in
and consequences. Leuk Lymphoma 2008;
children with acute lymphoblastic leukemia
16. Nadel S, Goldstein B, Williams MD, et al:
following induction therapy with corticoste-
40. Wong HR, Cvijanovich N, Wheeler DS, et al:
Drotrecogin alfa (activated) in children with
roid and other cytotoxic agents. J Pediatr
Interleukin-8 as a stratification tool for in-
severe sepsis: A multicentre phase III ran-
terventional trials involving pediatric septic
domised controlled trial. Lancet 2007; 369:
28. Petersen KB, Muller J, Rasmussen M, et al:
shock. Am J Respir Crit Care Med 2008;
Impaired adrenal function after glucocorti-
Pediatr Crit Care Med 2011 Vol. 12, No. 6
Département Recherches et Analyses M ax u la B o u rse Réalisations de AD W Y A au 3 0 / 0 9 / 2 0 0 9 Le s r é a l i s a t i o n s d e A D W Y A s e r a p p o r t a n t a u t r o i s i è m e t r i m e s t r e 2 0 0 9 t é m o i g n e n t d ’ u n e c a d e n c e c r o i s s a n t e d e s e s r e v e n u s T O T A L D E S V E N T E S L O C A
Dumping Syndrome: A Practical Approach to Diagnosis and Management . Andrew Ukleja, MD, CNSP. Cleveland Clinic Florida, Weston, Florida Learning objectives: Upon completion of this session you will be able to learn about diagnostic tests and diet and medical therapy for dumping syndrome. 1. Recognize which patients are at risk for dumping syndrome. 2. Select diagnostic test for early and
 Clinical course of sepsis in children with acute leukemia admitted
Clinical course of sepsis in children with acute leukemia admitted Data Source and Subject Identification. All
Table 1. Relapse rates among patient groups
Data Source and Subject Identification. All
Table 1. Relapse rates among patient groups
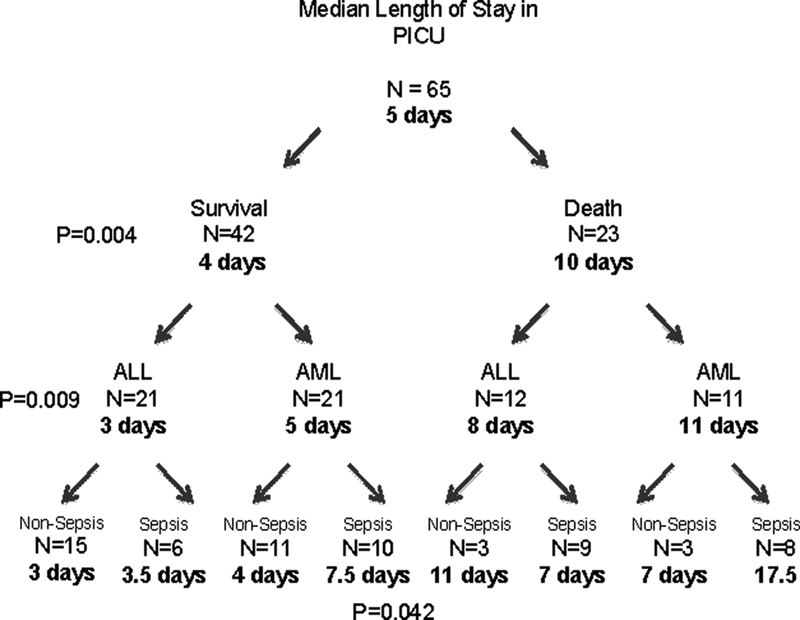 Table 2. Patient characteristics
Table 2. Patient characteristics Table 3. Distribution of patients in subgroups of steroid use, neutropenia, and death
Table 3. Distribution of patients in subgroups of steroid use, neutropenia, and death Table 6. Comparison of frequency of use of intensive care unit technology and outcomes among
Table 6. Comparison of frequency of use of intensive care unit technology and outcomes among quium of the International Sepsis Forum.
quium of the International Sepsis Forum.