Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
Macc.org.mt
Ulcerative Colitis Medications
There are four major classes of medicines that are used to treat ulcerative colitis. Details of how they work, when they might be used, and possible considerations are outlined below. Class of Medicine: 5-ASAs (5- aminosaliclic acid) Type of ulcerative colitis treated: Mild Moderate How it works: Anti-inflammatory medication Formulation: Oral (tablet), Rectal (enema or suppository) Benefits: Relief in 4–8 weeks. Without inflammation, diarrhoea, rectal bleeding and pain are reduced. Considered safe when used long-term Side-effects: Generally considered safe Examples: Mesalazine, Balsalazide, Olsalazine, Sulfasalazine Class of Medicine: Corticosteroids Type of ulcerative colitis treated: Moderate Severe How it works: Reduces inflammation (suppresses the immune system) Formulation: Oral (tablet), Rectal (enema), Intravenous (injection) Benefits: May bring relief in 1–3 weeks. Remission may be reached in 6–8 weeks Side-effects: Side effects (elevated blood sugar, high blood pressure, cataracts, osteoporosis) mean that medication is not safe for long-term use Examples: Prednisone, Methyl prednisolone (oral), Triamcinolone, Budesonide (rectal) Class of Medicine: Immuno-suppressants Type of ulcerative colitis treated: Maintenance of remission in refractory patients* How it works: Reduces inflammation (suppresses the immune system) Formulation: Oral Benefits: May bring relief in ~3 months. Often taken in conjunction with other medications Side-effects: Myelosuppression (lowering of the bone marrow’s ability to make platelets and blood cells), risk of infection, inflammation of pancreas and liver. Regular monitoring is essential Examples: Azathioprine, 6-mercaptopurine (6-MP) Class of Medicine: Biological therapies (Anti-TNFα) Type of ulcerative colitis treated: Moderate Severe How it works: Reduces inflammation (antibodies block specific molecules in the inflammation process) Formulation: Injection (home), Intravenous (hospital) Benefits: Relief in 2–4 weeks Side-effects: Before taking medication, you should be screened for tuberculosis (either by chest X- ray and/or skin test). Risk of infection (although lower than with corticosteroids), hypersensitivity reactions (joint pain, transient reaction or fever), heart failure (in elderly patients – check for swollen ankles and shortness of breath) or skin disorders. Examples: (In Europe:) Infliximab
*Patients who do not respond to standard medications
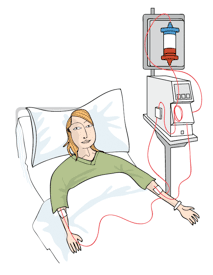
Medical devices Apheresis (leukocytapheresis)
Cells of the immune system called white blood cells (or leukocytes) defend the body against infections. In people with active IBD types of leukocytes called granulocytes and monocytes are often increased or over active. Large numbers of these cells enter the wall of the intestines and can release substances that cause bowel injury and stimulate inflammation. It is believed that the watery diarrhoea
seen in severe IBD is a result of injury to the absorptive epithelium which makes it unable to absorb water.
Apheresis, or leukocytapheresis, is performed with a medical device that selectively binds excess or activated granulocytes and monocytes from the blood. Blood is pumped from a vein in one arm (via a simple venopuncture) through a column containing cellulose acetate beads or a filter. This binds granulocytes and monocytes while the rest of the blood passes right through and is infused back into the body through the other arm. The outcome is a reduction in the number of inflammatory cells that can move from the blood into the intestinal wall. As a result, the symptoms of IBD are relieved, and the bowel gets a chance to heal.
The treatment lasts for 1 hour and is usually given once a week for 5 weeks. It can be performed in hospital or in an outpatient setting.
Leukocytapheresis involves mainly adults with IBD – there is some debate as to whether it is suitable for children. It can be used to reduce symptoms during a severe flare up, or in
moderate to severe active IBD in which satisfactory effects have not been achieved with corticosteroids or other immunosuppressive therapy.
Some temporary side effects can occur, such as low blood pressure, palpitations, and hot flushes; however, little is known about the long-term side effects of apheresis.
The biological processes through which leukocytapheresis affects the course of disease remain largely unknown, and it is difficult to draw conclusions from the existing clinical trial data on how effective the treatment really is.
APPENDIX A Appendix A tabulates the monthly cost (US $) of available anti-hypertensive and lipid lowering drugs individually in each SAARC country. For each drug within a class the minimum effective and the ceiling recommended dosage has been listed. For both, the minimum and the maximum monthly cost packages have been calculated. These cost packages are based on the available minimum and max
Tetrabenazine Tablets Tetrabenazine Tablets are not addictive. Consumer Medicine Information What is in this leaflet Before you take Tetrabenazine It does not contain all of the available When you must not take it Do not take Tetrabenazine Tablets • You are allergic to tetrabenazine or against the benefits they expect it will If you have any concerns about
 seen in severe IBD is a result of injury to the absorptive epithelium which makes it unable to absorb water.
Apheresis, or leukocytapheresis, is performed with a medical device that selectively binds excess or activated granulocytes and monocytes from the blood. Blood is pumped from a vein in one arm (via a simple venopuncture) through a column containing cellulose acetate beads or a filter. This binds granulocytes and monocytes while the rest of the blood passes right through and is infused back into the body through the other arm. The outcome is a reduction in the number of inflammatory cells that can move from the blood into the intestinal wall. As a result, the symptoms of IBD are relieved, and the bowel gets a chance to heal.
seen in severe IBD is a result of injury to the absorptive epithelium which makes it unable to absorb water.
Apheresis, or leukocytapheresis, is performed with a medical device that selectively binds excess or activated granulocytes and monocytes from the blood. Blood is pumped from a vein in one arm (via a simple venopuncture) through a column containing cellulose acetate beads or a filter. This binds granulocytes and monocytes while the rest of the blood passes right through and is infused back into the body through the other arm. The outcome is a reduction in the number of inflammatory cells that can move from the blood into the intestinal wall. As a result, the symptoms of IBD are relieved, and the bowel gets a chance to heal.