Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
Doi:10.1016/j.trstmh.2006.03.004
Transactions of the Royal Society of Tropical Medicine and Hygiene (2006) 100, 1013—1018
a v a i l a b l e a t w w w . s c i e n c e d i r e c t . c o m
j o u r n a l h o m e p a g e : w w w . e l s e v i e r h e a l t h . c o m / j o u r n a l s / t r s t
Efficacy of chloroquine and sulfadoxine/pyrimethamine for the treatment of uncomplicated falciparum malaria in Koumantou, Mali Xavier de Radigu` es , Kandian I. Diallo , Mouctar Diallo , Paul Akisa Ngwakum , Hamma Maiga , Abdoulaye Djimd´ Massambou Sacko , Ogobara Doumbo , Jean-Paul Guthmann
a Epicentre, 42 bis, Boulevard Richard Lenoir, 75011 Paris, Franceb M´edecins sans Fronti`eres, 70, rue de Gasperich, L-1617, Luxembourgc Malaria Research and Training Centre, DEAP/FMPOS/University of Bamako, BP 1805, Bamako, Malid Programme National de Lutte contre le Paludisme, Division de la Pr´evention et de la Lutte Contre la Maladie,Direction Nationale de la Sant´
Received 18 August 2005; received in revised form 29 March 2006; accepted 29 March 2006Available online 12 June 2006
KEYWORDS
We report the results of an in vivo antimalarial efficacy study with chloroquine (CQ)
and sulfadoxine/pyrimethamine (SP) conducted between 2003 and 2004 in Koumantou, south-
ern Mali. A total of 244 children were included in the study; 210 children were followed-up for
28 days according to WHO recommendations, with PCR genotyping to distinguish late recrude-
scence from re-infection. Global failure proportions at Day 14, without taking into account
re-infections, were 44.2% (95% CI 34.9—53.5%) in the CQ group and 2.0% (95% CI 0.0—4.8%) in
the SP group. PCR-adjusted failure proportions at Day 28 were even higher in the CQ group
(90.5% (95/105), 95% CI 84.8—96.2%) and relatively low in the SP group (7.0% (7/100), 95% CI
1.9—12.1%). These results show that CQ is no longer efficacious in Koumantou. The use of SP in
monotherapy is likely to compromise its efficacy. We recommend the use of artemisinin-basedcombination therapy as first-line treatment for uncomplicated Plasmodium falciparum malariain Koumantou. 2006 Royal Society of Tropical Medicine and Hygiene. Published by Elsevier Ltd. All rightsreserved.
∗ Corresponding author. Present address: Epicentre, 8 rue Saint Sabin, 75011 Paris, France. Tel.: +33 140 21 29 14; fax: +33 140 21 28 03.
0035-9203/$ — see front matter 2006 Royal Society of Tropical Medicine and Hygiene. Published by Elsevier Ltd. All rights reserved. 1. Introduction
Medicine, Pharmacy and Odonto-Stomatology, University ofBamako, Mali.
In Africa, resistance of Plasmodium falciparum to com-
Children aged 6—59 months living within <20 km from the
mon antimalarials represents a major obstacle for malaria
centre, weighing >5 kg and with suspicion of malaria (axillary
control. Resistance to antimalarials is responsible for an
temperature ≥37.5 ◦C) were screened. Children with a P. fal-
increase in morbidity and mortality in many sub-Saharan
ciparum monoinfection and asexual parasitaemia between
2000/l and 200 000/l, no signs of severity or severe
southern Africa shows that recent improvements in child-
malaria (including severe anaemia defined by haemoglobin
hood mortality due to diarrhoeal and vaccine-preventable
<5 g/dl), no history of allergic reactions to the respective
diseases have been counterbalanced by rising malaria deaths
study drugs, no presence of a concomitant febrile condi-
tion with the potential to confound the study outcome,
health problem with an annual incidence of 40.9 per 1000,
and no severe malnutrition were included if their guardians
accounting for 33% of all consultations for health care
consented in writing. Recent intake of antimalarials was
not an exclusion criteria. As no information on the effi-
the major at-risk population and account for 63% of total
cacy of these drugs in the study area was available for
cases. In this age group, 59% of all deaths are due to
any of the drugs, sample size estimates were based on
a 50% failure proportion for each drug. Applying a level
Resistance levels to chloroquine (CQ), the first-line rec-
of significance of 95% and a precision of 10%, 96 chil-
ommended drug, of 17—30% have been reported
dren per treatment arm were required. Allowing for a 10%
A recent study reported 60% resistance to CQ in
loss to follow-up, the final sample size was thus raised
to 106 children per treatment arm, i.e. 212 children in
studies were used, which have been shown to have low sen-
Children received one of the study drugs under direct
observation and were followed-up for 28 days. Because
showed high efficacy of sulfadoxine/pyrimethamine (SP),
the transmission season was well advanced and to ensure
the second-line drug in Mali, and a recent molecular-based
that recruitment could be finished in at least one of the
study did not find the DHFR-DHPS quin-
arms, the two drugs under study were tested consecu-
tuple mutant genotype associated with in vivo SP failure
tively, starting with CQ. Outcomes were both clinical and
parasitological, with PCR genotyping performed to distin-
transmission areas of Mali are needed in order to update
guish re-infections from recrudescences due to therapeutic
treatment policy-makers. Therefore, a study was carried out
and the Malaria Research and Training Centre (MRTC), Uni-
2.3. Treatment and follow-up
versity of Bamako, to evaluate the efficacy of these twoantimalarial drugs.
Upon inclusion, children received either: CQ 25 mg/kg basegiven at 10 mg/kg on Day 0 and Day 1 and at 5 mg/kg
2. Methods
1.25 mg/kg of pyrimethamine and 25 mg/kg of sulfadoxine
2.1. Study site
on Day 0 (Fansidar®; Roche, Basel, Switzerland). Dosageswere expressed as fraction of tablets and adapted to sim-
The study was carried out between October 2003 and
plify prescription. Drugs were crushed and mixed with water
March 2004 in the town of Koumantou, in the Sikasso
and sugar, given in a spoon or a syringe to smaller children.
region located in the southern part of Mali. The Kouman-
All doses were directly observed and repeated if vomiting
tou area is a rural area with 27 000 inhabitants spread
occurred within 30 min. Post-treatment visits were on Days
over 23 villages. Malaria is present throughout the year,
3, 7, 14, 21 and 28, or any other day in the case of recurrent
with a marked increase during the rainy season (i.e.
illness. At each visit, children were assessed clinically, axil-
May—November). The site was selected because of the exis-
lary temperature was recorded, and thick and thin blood
tence of a functional health centre with well trained per-
films were inspected. Haemoglobin was measured on Days
0, 14 and 28. Patients who presented haemoglobin <7 g/dl
in the neighbouring town of Bougouni. A survey con-
Rescue therapy in cases of uncomplicated malaria
mented common use of CQ, often given at an inappropriate
was oral artemisinin-based combination therapy (ACT)
of artemether 20 mg and lumefantrine 120 mg (AT + LU;Coartem®; Novartis, Zurich, Switzerland), whilst i.v. orintrarectal quinine (10 mg/kg/8 h) followed by oral AT + LU
2.2. Study design and procedures
was used in cases of complicated malaria.
On Day 0, a blood sample on filter paper was also taken
The study adhered to the latest WHO guidelines for assess-
for genotypic analysis and a second sample was collected in
ment of therapeutic efficacy of antimalarial treatment in
cases of symptomatic parasitaemia on or after Day 9, and at
high transmission settings (The study proto-
the end of follow-up in the presence of parasitaemia without
col was approved by the ethics committee of the Faculty of
Efficacy of CQ and SP for uncomplicated falciparum malaria
2.4. Endpoint classification 2.6. Data entry and analysis
Efficacy endpoints (failure or cure) were assigned according
Data were recorded in an individual record form and entered
to the latest WHO classification Patients were
into a locked Excel® spreadsheet and all entries were ver-
classified as early treatment failure (ETF) if they met any
ified. The data set was analysed using Stata® 8.02 (Stata
of the following criteria: (i) progression to severe malaria
Corp., College Station, TX, USA). Baseline characteristics of
in the presence of parasitaemia on Days 1, 2 or 3; (ii) par-
patients in each group were compared using a 2 test for cat-
asitaemia on Day 2 higher than on Day 0; (iii) any density
egorical variables and the Mann—Whitney U-test for contin-
of parasitaemia on Day 3 in the presence of fever; or (iv)
uous variables non-normally distributed. Failure proportions
parasitaemia on Day 3 ≥25% of the Day 0 count, irrespective
at Day 14 and Day 28 were calculated as the total number of
of fever. After Day 3, patients with recurrent parasitaemia
failures (ETF + LCF + LPF) over the total number of analysable
were classified as late clinical failure (LCF) if febrile, or late
outcomes, and expressed as a percentage with associated
parasitological failure (LPF) if they remained afebrile until
95% CI. PCR analysis results were used to adjust failure pro-
Day 28. All other children were classified as adequate clini-
portions at Days 9—28. Only treatment failures proven to
be recrudescence or mixed recrudescence and re-infection
Children were withdrawn from the study in the case of:
were classified as true failures. Patients for which the PCR
(i) vomiting any study dose twice; (ii) withdrawal of consent;
result was inconclusive (no DNA isolated) or reported as a
(iii) onset of a serious febrile illness other than malaria; (iv)
pure re-infection, patients lost to follow-up and secondary
intake of any drug with antimalarial properties; (v) skipping
exclusions were all excluded from the analysis.
any treatment dose; (vi) mixed parasitaemia; or (vii) anyprotocol violation. Patients who missed follow-up visits and
3. Results
did not come on successive days despite tracing were con-sidered lost to follow-up.
A total of 382 children were screened, of which 244 metthe inclusion criteria: 142 were assigned to the CQ arm
2.5. Laboratory procedures
and 102 to the SP arm One patient (0.4%) waslost to follow-up and 33 (13.5%) were withdrawn (31 inthe CQ arm and 2 in the SP arm). Reasons for withdrawal
Capillary blood was obtained by fingerprick sampling. Micro-
included intake of antimalarials (4), mixed parasitaemia (4),
scopic examination was performed according to WHO guide-
onset of serious illness (2), allergy to study drug (1), twice
lines (Thick and thin films were prepared on the
vomiting the study drug (11) and protocol violation (11).
same slide and stained with 10% Giemsa (pH 7.2) for 15 min.
Amongst the protocol violations, eight were due to para-
Asexual parasitaemia was quantified against 200—500 leuko-
sitaemia >200 000/l and three to parasitaemia <2000/l
cytes, assuming a white blood cell count of 8000/l. All
that appeared at the second reading of the Day 0 slides.
the Day 0, Day 2 and Day 3 slides, and at least 10% of
The number of patients analysable at Day 14 was 113 and
the follow-up slides, were re-read randomly every day and
100 in the CQ and SP arms, respectively. The number of
any discordance was resolved by a third reader. Exter-
patients analysable at Day 28 was 110 and 100 in the CQ
nal quality control on a random sample of slides (n = 152)
and SP groups, respectively. Baseline characteristics were
was carried out at the MRTC in Bamako, and by an inde-
similar across treatment groups, with the exception of tem-
pendent laboratory technician in France, yielding an end-
perature, haemoglobinaemia and parasite density: children
point affecting discordance in <4% of cases. Haemoglobin
had a higher temperature (P = 0.04), were more anaemic
was measured using a HemoCue® type haemoglobinome-
(P = 0.01), but had a lower parasitaemia (P < 0.01) in the CQ
Global failure proportions at Day 14, without taking into
In high-transmission settings, re-infections occur fre-
account re-infections, were 44.2% (95% CI 34.9—53.5%) in
quently and confound LCF and LPF endpoints. To identify
the CQ group and 2.0% (95% CI 0.0—4.8%) in the SP group.
true failures (recrudescence), blood samples were collected
PCR-adjusted failure proportions at Day 28 were even higher
on Whatman No. 3 filter paper and analysed at the MRTC
in the CQ group (90.5% (95/105), 95% CI 84.8—96.2%),
by PCR of P. falciparum DNA extracted from the Day 0 and
but were still low in the SP group (7.0% (7/100), 95% CI
failure day samples. Procedures in this laboratory relied
1.9—12.1%); ETFs were frequent in the CQ group (29.5%
(31/105), 95% CI 20.7—38.4%); in the SP group, there were
Cartwright comparing the Day 0 and failure day
two ETFs Only 16.0% (17/106) of CQ-treated
alleles of the merozoite surface proteins msp-1 and msp-2 as
patients but 83.0% (83/100) of those receiving SP were para-
well as glurp gene loci. Possible outcomes were: (i) recrude-
site free on Day 3. In the CQ group, the majority of treatment
scence if the alleles of the pre- and post-treatment samples
failures were pure or mixed recrudescence (90.5% (57/63)),
were the same for msp-1, msp-2 and glurp; (ii) re-infection
whereas none of the children in the SP arm experienced a
if the alleles of the pre- and post-treatment samples were
distinct; (iii) mixed recrudescence and re-infection if similaralleles were found in the pre- and post-treatment samplesfor all the markers as mentioned above, but with additional
4. Discussion
distinct alleles identified; or (iv) no DNA isolated, if eitheror both the pre- and post-treatment samples could not be
This study provides estimates of the in vivo antimalarial effi-
cacy of first- and second-line drugs in Mali, where current
Details of study inclusion and follow-up of patients in the in vivo antimalarial efficacy study, Koumantou, Mali, 2003—2004.
CQ: chloroquine; SP: sulfadoxine/pyrimethamine.
Baseline (Day 0) characteristics of patients included in the in vivo antimalarial efficacy study, Koumantou, Mali,
Antimalarial treatment before inclusion, n (%)
Axillary temperature (◦C) (median (IQR))
Moderate anaemia (<8 g/dl), n (%)
Asexual parasitaemia (l) (geometric mean
CQ: chloroquine; SP: sulfadoxine/pyrimethamine; IQR: interquartile range (25—75%). a Two missing values. b Three missing values.
data regarding CQ and SP were urgently needed. Method-
results between the two arms. A second limitation is the rel-
ologically, the 28-day follow-up combined with adjustment
atively high number of withdrawals in the CQ arm owing to
of the results by PCR analysis provided more realistic esti-
some misunderstandings by the staff at the beginning of the
mates of efficacy than the traditional 14-day studies.
study. Nevertheless, measures taken (such as further train-
The major limitation of our study was the method of
ing of nurses and laboratory staff) have probably limited
treatment allocation, which was not randomised. This could
potential biases. The validity of our data is further supported
explain the unequal level of fever, haemoglobin and parasite
by the almost non-existent loss to follow-up and the low pro-
density at inclusion and does not allow a strict comparison of
Failure proportions at Day 28 (clinical and parasitological failures, after PCR adjustment) for the in vivo antimalarial
efficacy study, Koumantou, Mali, 2003—2004
CQ: chloroquine; SP: sulfadoxine/pyrimethamine; ETF: early treatment failure; LCF: late clinical failure; LPF: late parasitological failure.
Efficacy of CQ and SP for uncomplicated falciparum malaria
We have shown that the in vivo resistance to CQ, the first-
Koumantou team for their enthusiasm and excellent work:
line antimalarial treatment in Mali, was unquestionably very
Dr Hamadoun Yattara, Christiane Dembele, Ali Poudougou,
high in Koumatou area, confirming previous reports from
Brahima Sidebe, Mamadou Kone, Moussa Diakate, Adama
Doumbia, Brehima Koulibaly, Lassina Kone, Aminata Konate
erard Fabrice. Many thanks to Dr Bakary Fofana of the
MRTC for his help with PCR analysis, and to Dr Amagana Dolo
is thus well above the 25% value considered by the WHO
of the same institution for performing the external quality
as the threshold for changing the drug policy
control. Thanks to Kodzo Tupko for performing the second
The dramatic impact of CQ resistance on childhood mor-
quality control in France. Thanks to Evelyn Depoortere (Epi-
bidity and mortality has been well described in western
centre), Rony Zachariah and Martin De Smet (MSF, Belgian
Africa In Kenya, 69% of deaths due to malaria
section) for their external support. This study was funded
were attributed to ineffective CQ treatment (
In vivo resistance to SP, which was the second-line anti-
References
malarial in Mali, was relatively low, well below the WHOthreshold and confirming the existing MRTC data
Abacassamo, F., Enosse, S., Aponte, J.J., Gomez-Olive, F.X., Quinto,
L., Mabunda, S., Barreto, A., Magnussen, P., Ronn, A.M., Thomp-
be used as monotherapy as resistance to SP is known to
son, R., Alonso, P.L., 2004. Efficacy of chloroquine, amodi-
develop rapidly Furthermore, recent studies
aquine, sulfadoxine—pyrimethamine and combination therapy
with artesunate in Mozambican children with non-complicated
reported unacceptable levels of resistance to
malaria. Trop. Med. Int. Health 9, 200—208.
Checchi, F., Roddy, P., Kamara, S., Williams, A., Morineau, G.,
In the face of spreading antimalarial drug resistance, the
Wurie, A.R., Hora, B., Lamotte, N., Baerwaldt, T., Heinzel-
WHO recommends that monotherapeutic options be aban-
mann, A., Danks, A., Pinoges, L., Oloo, A., Durand, R., Ranford-
doned in favour of combination therapy (This
Cartwright, L., Smet, M., Stivanello, E., Cavailler, P., Cas-
approach, already in use for tuberculosis and AIDS, is essen-
sano, F., Omar, S.A., Kariuki, D., Mwangi, J., Piola, P., Guth-mann, J.P., 2005. Evidence basis for antimalarial policy change
tial not only to improve efficacy but also to protect remain-
in Sierra Leone: five in vivo efficacy studies of chloroquine,
ing viable antimalarials against further spread of resistant
sulfadoxine—pyrimethamine and amodiaquine. Trop. Med. Int.
ommends that combinations including an artemisinin deriva-
Coulibaly, D., Diallo, D.A., Thera, M.A., Dicko, A., Guindo, A.B.,
Kone, A.K., Cissoko, Y., Coulibaly, S., Djimde, A., Lyke, K.,
The results of this study clearly discourage the combina-
Doumbo, O.K., Plowe, C.V., 2002. Impact of preseason treat-
tion of CQ with artemisinin derivatives. SP + artesunate (AS)
ment on incidence of falciparum malaria and parasite density at
has been tested elsewhere in Africa and showed good effi-
a site for testing malaria vaccines in Bandiagara, Mali. Am. J.
cacy in sites where resistance to SP was low
Diourte, Y., Djimde, A., Doumbo, O.K., Sagara, I., Coulibaly, Y.,
Dicko, A., Diallo, M., Diakite, M., Cortese, J.F., Plowe, C.V.,
disappointing where SP resistance was already well devel-
1999. Pyrimethamine—sulfadoxine efficacy and selection for
mutations in Plasmodium falciparum dihydrofolate reductase
ACT represents a good alternative to be used as first-line
and dihydropteroate synthase in Mali. Am. J. Trop. Med. Hyg.
antimalarial treatment in Koumantou. AT + LU is another ACT
that could be proposed. It is a highly efficacious fixed combi-
Djimde, A., Doumbo, O.K., Cortese, J.F., Kayentao, K., Doumbo,
nation but is relatively expensive (approximately US$2.4 for
S., Diourte, Y., Dicko, A., Su, X.Z., Nomura, T., Fidock, D.A.,
treating an adult). Amodiaquine (AQ) + AS is another option,
Wellems, T.E., Plowe, C.V., Coulibaly, D., 2001. A molecular
providing that AQ efficacy remains acceptable. Its price,
marker for chloroquine-resistant falciparum malaria. N. Engl.
when available in blister, is similar to that of the SP + AS
combination (approximately US$1.5), and a fixed combina-
Djimde, A.A., Dolo, A., Ouattara, A., Diakite, S., Plowe, C.V.,
Doumbo, O.K., 2004. Molecular diagnosis of resistance to anti-
tion should be marketed in the near future.
malarial drugs during epidemics and in war zones. J. Infect. Dis.
Our data support the decision made by the Ministry of
Health of Mali, which recently changed its malaria treat-
Korenromp, E.L., Williams, B.G., Gouws, E., Dye, C., Snow, R.W.,
ment guidelines and adopted AS + AQ or AT + LU as first-line
2003. Measurement of trends in childhood malaria mortality in
Africa: an assessment of progress toward targets based on verbalautopsy. Lancet Infect. Dis. 3, 349—358. Conflicts of interest statement
Kublin, J.G., Dzinjalamala, F.K., Kamwendo, D.D., Malkin, E.M.,
The authors have no conflicts of interest concerning the work
Cortese, J.F., Martino, L.M., Mukadam, R.A., Rogerson, S.J.,
Lescano, A.G., Molyneux, M.E., Winstanley, P.A., Chimpeni, P.,Taylor, T.E., Plowe, C.V., 2002. Molecular markers for failure of
Acknowledgements
sulfadoxine—pyrimethamine and chlorproguanil—dapsone treat-ment of Plasmodium falciparum malaria. J. Infect. Dis. 185,380—388.
This study benefited from the kind attention of the National
Nosten, F., Brasseur, P., 2002. Combination therapy for malaria: the
Malaria Control Programme of Mali. We wish to express
our gratitude to Dr Ouatara, Bougouni Medical Director,
Olliaro, P.L., Taylor, W.R., 2003. Antimalarial compounds: from
for his kind support. Many thanks to the members of the
bench to bedside. J. Exp. Biol. 206, 3753—3759.
Plowe, C.V., Doumbo, O.K., Djimde, A., Kayentao, K., Diourte, Y.,
2000. Child malaria treatment practices among mothers in the
Doumbo, S.N., Coulibaly, D., Thera, M., Wellems, T.E., Diallo,
district of Yanfolila, Sikasso region, Mali. Trop. Med. Int. Health
D.A., 2001. Chloroquine treatment of uncomplicated Plasmod-ium falciparum malaria in Mali: parasitologic resistance versus
Trape, J.F., 2001. The public health impact of chloroquine resis-
therapeutic efficacy. Am. J. Trop. Med. Hyg. 64, 242—246.
tance in Africa. Am. J. Trop. Med. Hyg. 64, 12—17.
Priotto, G., Kabakyenga, J., Pinoges, L., Ruiz, A., Eriksson, T.,
von Schenck, H., Falkensson, M., Lundberg, B., 1986. Evaluation
Coussement, F., Ngambe, T., Taylor, W.R., Perea, W., Guth-
of ‘HemoCue,’ a new device for determining hemoglobin. Clin.
mann, J.P., Olliaro, P., Legros, D., 2003. Artesunate and
sulfadoxine—pyrimethamine combinations for the treatment of
von Seidlein, L., Milligan, P., Pinder, M., Bojang, K., Anyalebechi,
uncomplicated Plasmodium falciparum malaria in Uganda: a ran-
C., Gosling, R., Coleman, R., Ude, J.I., Sadiq, A., Duraisingh,
domized, double-blind, placebo-controlled trial. Trans. R. Soc.
M., Warhurst, D., Alloueche, A., Targett, G., McAdam, K., Green-
wood, B., Walraven, G., Olliaro, P., Doherty, T., 2000. Efficacy of
Ranford-Cartwright, L.C., Taylor, J., Umasunthar, T., Taylor, L.H.,
artesunate plus pyrimethamine—sulfadoxine for uncomplicated
Babiker, H.A., Lell, B., Schmidt-Ott, J.R., Lehman, L.G., Wal-
malaria in Gambian children: a double-blind, randomised, con-
liker, D., Kremsner, P.G., 1997. Molecular analysis of recrudes-
trolled trial. Lancet 355, 352—357.
cent parasites in a Plasmodium falciparum drug efficacy trial in
White, N.J., 1992. Antimalarial drug resistance: the pace quickens.
Gabon. Trans. R. Soc. Trop. Med. Hyg. 91, 719—724.
J. Antimicrob. Chemother. 30, 571—585.
Sangho, H., Diawara, A., Diallo, M., Sow, S., Sango, H.A., Sacko,
WHO, 1996. Assessment of therapeutic efficacy of antimalarial drugs
M., Doumbo, O., 2004. [Assessment of chloroquine resistance
for uncomplicated falciparum malaria in areas with intense
two years after stopping chemoprophylaxis in 0 to 9-year-old
transmission. Division of Control of Tropical Diseases, World
children living in a malaria-endemic village of Mali]. Med. Trop.
Health Organization, Geneva, WHO/MAL/96.1077.
WHO, 2001. The Use of Antimalarial Drugs: Report of an Informal
Snow, R.W., Trape, J.F., Marsh, K., 2001. The past, present and
WHO consultation, 13—17 November 2000. World Health Organi-
future of childhood malaria mortality in Africa. Trends Parasitol.
zation, Geneva, WHO/CDS/RBM/2001.33.
WHO, 2002. WHO urges countries to act on new anti-resistance
Stepniewska, K., Taylor, W.R., Mayxay, M., Price, R., Smithuis, F.,
malaria medicines. World Health Organization, Geneva, Press
Guthmann, J.P., Barnes, K., Myint, H.Y., Adjuik, M., Olliaro, P.,
Pukrittayakamee, S., Looareesuwan, S., Hien, T.T., Farrar, J.,
WHO, 2003. Assessment and monitoring of antimalarial drug efficacy
Nosten, F., Day, N.P., White, N.J., 2004. In vivo assessment of
for the treatment of uncomplicated falciparum malaria. World
drug efficacy against Plasmodium falciparum malaria: duration
Health Organization, Geneva, WHO/HTM/RBM/2003.50.
of follow-up. Antimicrob. Agents Chemother. 48, 4271—4280.
WHO Roll Back Malaria, 2001. Country strategies and resource
Stivanello, E., Cavailler, P., Cassano, F., Omar, S.A., Kariuki, D.,
Mwangi, J., Piola, P., Guthmann, J.P., 2004. Efficacy of chloro-
quine, sulfadoxine—pyrimethamine and amodiaquine for treat-
Zucker, J.R., Ruebush 2nd, T.K., Obonyo, C., Otieno, J., Campbell,
ment of uncomplicated Plasmodium falciparum malaria in Kajo
C.C., 2003. The mortality consequences of the continued use of
Keji county, Sudan. Trop. Med. Int. Health 9, 975—980.
chloroquine in Africa: experience in Siaya, western Kenya. Am.
Thera, M.A., D’Alessandro, U., Thiero, M., Ouedraogo, A., Packou,
J., Souleymane, O.A., Fane, M., Ade, G., Alvez, F., Doumbo, O.,
_______________________________ Indian Public Health Standard (IPHS) Community Health Centres Level _______________________________ Draft Guidelines Directorate General of Health Services Ministry of Health and Family Welfare Government of India Executive Summary Introduction Requirements in CHC Quality Assurance in Service Delivery C
[1] B Brown, M E Dewey, and A P Day. An objective automated method for digitising pictorialmaterial for computer manipulation. Behavior Research Methods and Instrumentation, 8:378–381,1976. [2] M E Dewey, G M Stephenson, and A C Thomas. Organisational unit size and individual attitudes. Sociological Review, 26:125–137, 1978. [3] D R Rutter, G M Stephenson, and M E Dewey. Visual communicati

 Transactions of the Royal Society of Tropical Medicine and Hygiene (2006) 100, 1013—1018
Transactions of the Royal Society of Tropical Medicine and Hygiene (2006) 100, 1013—1018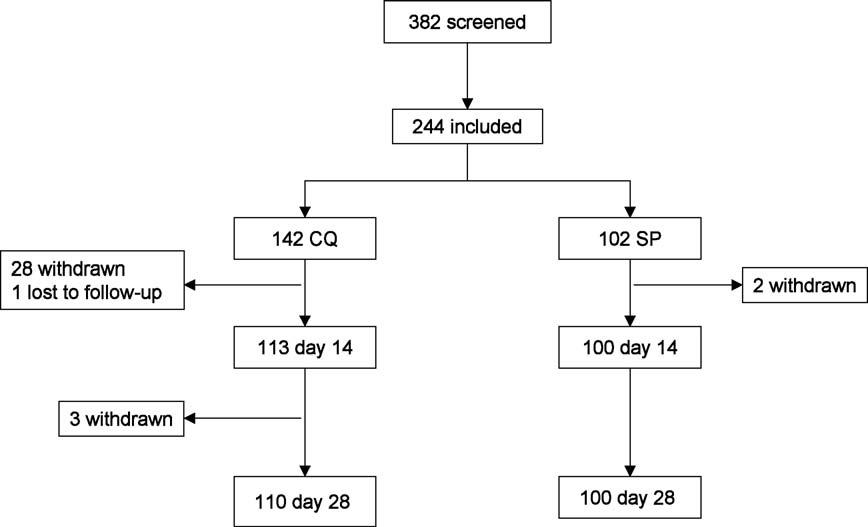 Details of study inclusion and follow-up of patients in the in vivo antimalarial efficacy study, Koumantou, Mali, 2003—2004.
Details of study inclusion and follow-up of patients in the in vivo antimalarial efficacy study, Koumantou, Mali, 2003—2004.