Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
Microsoft word - pain in the elderly1.2-chopra.doc
Pain is defined by The International Association for the Study of Pain as an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. In the elderly many complex issues may contribute to the emotional experience of pain including: a long history of various pain experiences, multiple chronic comorbid conditions, proximity to death, dependency issues and family support issues. Presbyalgos is defined as advanced age systematically influencing pain sensitivity and perception in the later years of life. Over the last century, the life expectancy has increased from 48 years to 76 years in the United States of America. An increasing number of people are growing into the seventh, eighth and ninth decades. Studies have shown a peak or plateau on the prevalence of pain by 65 years of age. There is then a decline in reported pain after 75 years, even though there is an age related increase in diseases associated with pain (e.g. degenerative joint disease). During this decade the increase in the elderly population will be moderate. However, between 2010 and 2030 the ‘baby boomer’ population will begin entering the over-65 generation. The expected population in this age group by 2030 will be between 19% and 21% of the total population. Gerontologists have identified subgroups of the elderly population. The most frequently used grouping is by age:
1. Young-old: 65 years to 75 years. This is a generally healthy and active
2. Old-old: 76 years to 90 years. This subgroup is characterized by
decreasing independence and increasing morbidity with an increasing demand on health care services.
3. Oldest-old: 90 years and above. There is a high level of morbidity in
this subgroup. They also present with difficult to manage pain.
Studies have shown wide variations in the prevalence of pain in the elderly. One of the earliest studies conducted by Crook et al, showed increased pain complaints with increasing age. They also showed that the prevalence of temporary pain was the same at all ages with a decline in persistent pain over time on occasion in the same individuals. A review of major studies on the prevalence of chronic pain in the elderly by Helme suggested a peak or plateau in the prevalence of pain by age 65 and a decline in the old-old and the oldest-old groups. The decline in pain in these groups is surprising considering the significant increases in diseases that cause increased pain such as degenerative joint disease. The reasons for this wide variation for reporting of pain in the elderly may be due to methodological variations, number of subjects in each age group and variation in response rates in the different sub groups of the elderly (especially the oldest-old e.g. educational status, unreliability of the memory of pain and early dementia). One of the reasons for increased pain in the elderly undoubtedly is the increased number of coexisting diseases. The incidence of post herpetic neuralgia, degenerative joint disease, spinal stenosis, osteoarthritis, osteoporosis, fractures and stroke are significantly higher in this age group and continues to increase with advancing age. In the old-old and oldest-old subgroups of the elderly there appears a decrease in pain reporting. This decline in pain reporting may be secondary to the elderly beginning to lose more and more of their independence. Elderly patients tend to be sequestered in institutions as a result of which reporting of pain amongst the elderly in the community is lower. Some possible contributing factors for less reporting of pain in the elderly include: loss of cognitive functions, a tendency to be stoic in dealing with pain, other significant issues in their life overshadowing pain complaints (e.g. loss of a partner or a loved one), preoccupation in dealing with their disability and altered nociceptive pathways.
The effect of pain in patients with dementia is unclear. These patients have a loss of communication skills, cognitive function and eventually failure of basic reflexes (e.g. gag reflex) in the later stages. Many of these functions are critical for pain expression. It is unclear if the reduced response to pain is due to decreased sensitivity to pain stimulus or if they have an apathy to pain. They appear to have a loss of interest and decreased response to any noxious stimulus. The pain response in dementia maybe a combination of different etiologies including loss of cognitive skills and indifference or anhedonia. As dementia becomes more advanced, caution should be used when relying on self reporting of pain. Pain assessment in these patients should factor in direct observations as in facial expressions and input from significant others. There may exist age related physiological changes leading to decreased perception of nociceptive pain, however this remains uncertain. There is a decreased density of myelinated and unmyelinated nerve fibers in the elderly. Nerve conduction studies have shown prolonged latencies in the peripheral sensory nerves in older healthy persons. Studies have reported that older patients report pain only after C-fiber activation. In comparison, younger adults use additional information from Aδ fibers when reporting pain. Furthermore, when the Aδ fiber input was blocked in young adults, age related differences in pain threshold and subjective ratings in pain intensity disappeared. Therefore it is conceivable that analgesic strategies for the elderly should be directed towards modulation of the C-fiber input. Cerebral event-related potential (CERP) is an electroencephalogram response study to any stimulus. There is a strong relationship between peak amplitude and subjective ratings of pain in response to increasing stimulation. It represents an integrated response to CNS processing of afferent input. The CERP in response to noxious stimulus is altered with increasing age. This finding supports that there is slowing in the cognitive processing of noxious stimulus and decreased activation of cortical responses in the elderly.
Acute pain
Acute pain reporting in the elderly is strikingly different and consistent across all subgroups of the elderly population. Common acute processes in the elderly leading to acute pain include: infection, inflammation (e.g. diverticulitis), ischemia (e.g. myocardial infarction), tissue insult, trauma, surgery and osseous fractures. They may report less pain associated with an acute pathology. Pain tends to be reported in an atypical manner making the diagnosis of the condition difficult. Pathological conditions that produce pain in the young may instead present with mental status changes such as lethargy, confusion, restlessness and anorexia in the elderly. Ambepitiya et al reported that of the elderly who suffered acute myocardial infarction, 305 did not report any acute symptoms and another 30% had atypical symptoms. Atypical presentations have also been reported in acute intra abdominal pathology. Treatment of acute pain in the elderly carries with it the challenges of maximizing side effects. Continuous peripheral neural blockade (if feasible and appropriate) may provide optimal results in various situations. Traditional methods of acute pain management (especially in the Perioperative period) such as intravenous patients controlled analgesia (PCA) or epidural analgesics (with or without patient controlled mode) are used in the elderly. It is often prudent to start with a lower does (e.g. start low and go slow) when treating acute pain with these strategies, in the elderly. For example, intravenous PCA hydromorphone doses for adults typically range from 0.15mg to 0.25mg. However, in the elderly a starting dose of 0.1mg is often utilized. When using epidural analgesia in adults, the concentrations may be fentanyl 4 mcg/cc or hydromorphone 20 mcg/cc, in the elderly a starting concentration for fentanyl would be 1 mcg/cc to 2 mcg/cc or hydromorphone 5 mcg/cc to 10 mcg/cc. The coping mechanisms adapted by the elderly with chronic pain are very different than mechanisms adapted by the younger patients. The elderly tend to use passive coping strategies such as spiritual solace and mental distraction. Therefore it is conceivable that the elderly may respond well to behavioral and psychological strategies.
Cultural beliefs in coping with pain are very important in the elderly. Many of them believe that pain is part of growing old and accept it as a physiological change. Personal and cultural belief’s affect how the elderly accept pain. These beliefs may influence the way they self report pain, seek treatment and comply with treatment. Very often mild aches and pains are attributed to the normal aging process and they tend not to seek medical attention. The elderly as a group is reluctant to acknowledge the contribution of psychological factors in their pain experience. Physicians should initiate discussions with their elderly patients about any pain that they may be suffering and offer them therapeutic options.
Barriers to Effective Pain Management
• Fear of disease (heralding sign or progression)
• Aging blunts/reduces pain perception
• Cannot adequately assess (especially in impaired, for example if
• Lack of training in using narcotic prescriptions
• Concern about patient addiction/abuse
• Low priority to pain assessment and treatment
Adapted from Jacox A, Carr DB, Payne R, et al: Management of Cancer Pain. Clinical Practice
Guideline No. 9. AHCPR Publication No. 94-0592. Rockville, MD, Agency for Health Care
Policy and Research, US Department of Health and Human Services, Public Health Service,
Chronic pain Chronic pain perception may also be different in the elderly. Osteoarthritis in the elderly significantly limits their ability to function and to care for themselves. It is the leading cause of disability over the age of 65 years. In the United States of America alone it affects over 20 million adults. The joints become swollen, painful and stiff. When the hips and knees are affected their ability to conduct their activities of daily living, is impaired. Because of restricted joint mobility they lose muscle tone and strength. The
pain limits their ability to walk, restricts their social interaction and compromises their physical mobility thus reducing their independence. The Agency for Healthcare Research and Quality (AHRQ) has noted that the key to effectively manage osteoarthritis is by developing an effective physician-patient partnership. The partnership should:
Acetaminophen and nonsteroidal anti-inflammatory drugs (NSAID) including Cox-2 inhibitors are often used for pain relief in osteoarthritis. These drugs may provide only a modest analgesic effect. In the elderly NSAIDs have been associated with increased morbidity. NSAIDs may lead to peptic ulcers, gastrointestinal bleeding and affect joint cartilage metabolism.
2. Encourage patients to change their behavior to improve symptoms or
Encourage patients to understand their disease process and adjust their lifestyle accordingly. Regular exercise such as walking, aquatic therapy, and aerobics may help patients retain their mobility, prevent muscle loss, decrease depression and help regain their confidence.
3. Instruct patients on how to interpret and report symptoms accurately
4. Help patients adjust to new social and economic circumstances and
5. Support patients’ efforts to participate in treatment decisions and
Cancer pain Cancer pain in the elderly has always been challenging to manage. In addition to morbidity from the primary cancer elderly patients may have comorbid conditions as well as multiple associated symptoms. Management of these
symptoms results in polypharmacy making them more susceptible to adverse drug reactions because of age related changes in absorption, metabolism and excretion and increased drug-drug interactions. Inadequate treatment of pain is a major issue. These patients may experience both nociceptive and neuropathic pain at multiple sites by several different mechanisms:
1. Pain from cancer: Direct tumor involvement
Invasion of the bone by tumor accounts for 50% of the cases in patients with breast cancer, prostate cancer and multiple myeloma. Pain due to nerve compression, soft tissue infiltration or invasion of the gastrointestinal tract accounts for the other 50% cases.
2. Pain from Caner treatment: Painful neuropathy associated with
3. Pain unrelated to cancer or its treatment: Prevalence of pain due to
other comorbid conditions such as osteoarthritis accounts for a significant large number of elderly patients.
Common cancer-related pain syndromes Peripheral neuropathies Bone metastases Epidural metastases/spinal-cord compression Plexopathies Abdominal pain Mucositis Common cancer-related pain syndromes
Sutton LM, Demark-Wahnefried, Clipp E; Management of terminal cancer in the elderly patients; The Lancet Oncology, vol 4, No: 3, March 2003 Management of cancer pain in the elderly must be based on a regular schedule or round the clock administration of analgesics rather than on an as needed basis. This maintains a steady serum concentration. In addition to ‘maintenance analgesics’, they should also be given analgesics with rapid onset of action for breakthrough pain. The dose for the breakthrough analgesics is usually 15% to 20% of the baseline 24-hour dosing. It is vitally important to attempt to adopt the following principles when treating pain in the elderly:
1. Keep the analgesic regimen simple 2. Minimize the number of analgesics 3. Minimize the frequency of analgesic dosing (e.g. aim for once or twice
The World Health Organization has recommended the three-step ladder of analgesic therapy for cancer pain. The first step consists of starting with non-opioid analgesics such as acetaminophen, aspirin or nonsteroidal drugs for mild to moderate pain. If the pain continues to persist then patients are continued to be maintained on non-opioid analgesics together with opioids for moderate pain such as hydrocodone, codeine or combinations. Step three is considered when the patients continues to have unrelieved pain. In this step, ‘strong’ opioids (e.g. morphine, fentanyl) for severe pain are started. Adjuvant medications are drugs that although not labeled as analgesics, may
exhibit analgesic potential. Examples of adjuvant medications maybe anticonvulsants and antidepressants. Adjuvant medications may be started with step one and can be modified or tailored throughout the treatment.
Figure: The World Health Organization ladder is tailored to the needs of patients with pain. Pharmacologic management of pain in the elderly must maintain a delicate balance between the risks of cognitive impairment and other side effects versus the clinical benefit. Consideration should be given to medications taken for other co-existing conditions and the possibility of drug interaction. Table 2. Adjuvant medications for chronic pain management. Medication Indications/Comments Tricyclic antidepressants
sedation, cardiac arrhythmias orthostatic hypotension
Anti-seizure medications
300 mg/day on the third day;then titrate to effect
Steroids
improves appetite, mood, and energy level;
Other medications
From: Abrahm JL. A Physician's Guide to Pain and Symptom Management in Cancer Patients. Baltimore, Md: John Hopkins University Press; 2000.
Acetaminophen is a relatively safe drug of first choice for treating mild to moderate pain in the elderly. The maximum dose of acetaminophen per day should not exceed 4000mg. Acetaminophen in combination with other drugs such as hydrocodone helps potentate the effects thus allowing lower doses of both drugs and good pain control. All too often patients take over the counter acetaminophen or in combinations with cold medicines without realizing that they maybe exceeding the maximum dose. Reduced doses must be used in patients with liver disease.
Other analgesic agents used in the elderly include: anti-inflammatory agents (COX-2 inhibitors are associated with less gastrointestinal mucosal insult in the elderly), tramadol and opioids Step 2 and 3 of the WHO ladder is to either add an opioid or switch to a pure opioid for managing pain should the drugs in step 1 with or without adjuvants not work. The more commonly used drugs of this class are: Oxycodone, morphine, hydromorphone and fentanyl. Opioids such as Oxycodone and hydromorphone without significant active metabolites may exhibit advantages in the elderly, since renal function may be compromised In conclusion, chronic pain is the single most common complaint in the elderly and has the greatest impact on quality of life. A comprehensive assessment must be done, followed by a multidisciplinary approach to treating the pain. A rational pharmacotherapeutic approach should be adopted, with starting low and going slow at each dose level with frequent patient assessment and monitoring. The quality of life, prognosis, and frailty of the elderly population should be taken into considering the risk versus benefit of any therapy. Physical and behavioral medicine should be factored in when treating pain in the elderly.
References
1. Smith H, Chen G: Geriatric pain management issues. Progress in Anesthesiology:
Dannemiller Memorial Educational Foundation, December 2000.
2. Clinch D, Banjeree AK, Ostick G: Absence of abdominal pain in elderly patients with
3. Harkins SW, Chapman CR: The perception of induced dental pain in young and elderly
4. Helme RD, Gibson SJ: Pain in older people. In Crombie IK, Croft PR, Linton SJ, et al
(eds): Epidemiology of Pain. Seattle, WA, IASP Press, 2000, p 103
5. Helme RD, Gibson SJ: Pain in the elderly. In Jensen TS, Turner JA, Wiesenfeld-
Hallin Z (eds): Proceedings of the 8th World Congress on Pain, Progress in Pain Research and Management, Seattle, WA, IASP Press, 1997, p 919
6. Harkins SW, Price DD, Bush FM, et al: Geriatric pain. In Wall PD, Melzack M (eds):
Textbook of Pain, ed 3. New York, Churchill Livingstone, 1994, p 769
7. Gibson SJ, Gorman MM, Helme RD: Assessment of pain in the elderly using event-
related cerebral potentials. In Bond MR, Charlton JE, Woolf C (eds): Proceedings of the VIth World Congress on Pain, Amsterdam, Elsevier Science Publishers, 1990 p 523
8. James FR, Large RG, Bushnell JA, et al: Epidemiology of pain in New Zealand. Pain
9. Magni G, Schifano F, De Leo D: Pain as a symptom in elderly depressed patients. Eur
Arch Psychiatry Neurol Sci 235:143, 1985
10. McCracken LM: Learning to live with pain: Acceptance of pain predicts adjustment in
persons with chronic pain. Pain 74:21, 1998
11. Gibson SJ, Helme RD: Age differences in pain perception and report: A review of
physiological, psychological, laboratory and clinical studies. Pain Rev 2:111, 1995
12. Farrell MJ, Gibson SJ, Helme RD: Chronic non-malignant pain in older people. In
Ferrell B, Ferrell B (eds): Pain in the Elderly. Seattle, WA, IASP Press, 1996, p 81
13. Clark WC, Mehl L: Thermal pain: A sensory decision theory analysis of the effect of
age and sex on d', various response criteria, and 50% pain threshold. J Abnorm Psychol 78:202, 1971
14. Barberger-Gateau P, Chaslerie A, Dartigues J, et al: Health measures correlates in a
French elderly community population: The PAQUID study. J Gerontol 472:S88, 1992
15. Stein WM, Ferrell BA: Pain in the nursing home. Clin Geriatr Med 12(part 3):601,
16. Sengstaken EA, King SA: The problem of pain and its detection among geriatric
nursing home residents. J Am Geriatr Soc 41(part 5):541, 1993
17. Parmalee PA: Pain in cognitively impaired older persons. Clin Geriatric Med 12(part
18. Harkins SW: Pain perceptions in the old. Clin Geriatr Med 12(part 3):435, 1996 19. Gagliese L, Melzack R: Chronic pain in elderly people. Pain 70:3, 1997 20. AMDA: Chronic pain management in the long-term care setting. Clinical practice
21. AGS Panel on Chronic Pain in Older Persons: The management of chronic pain in older
22. National Institute of Arthritis and Musculoskeletal and Skin Diseases. Handout on
health: osteoarthritis. Web site: http://www.niams.nih.gov/hi/topics/arthritis/oahandout.htm
23. Hochberg MC, Altman RD, Brandt KD, et al. Guidelines for the medical management
of osteoarthritis. Part I. Osteoarthritis of the hip. Arthritis Rheum 1995;38(11):1535-40
24. Griffin MR, Brandt KE, Liang MH, et al. Practical management of osteoarthritis.
Integration of pharmacologic and nonpharmacologic measures. Arch Fam Med 1995;4(12):1049-55.
25. Sutton LM, Demark-Wahnefried, Clipp E; Management of terminal cancer in the
elderly patients; The Lancet Oncology, vol 4, No: 3, March 2003
26. Abrahm JL. A Physician's Guide to Pain and Symptom Management in Cancer
Patients. Baltimore, Md: John Hopkins University Press; 2000.
27. Portenoy RK, Hagen NA. Breakthrough pain: definition, prevalence and
28. Cherny NI, Portenoy RK. Cancer Pain Management. Cancer 1993;72:3393-415 29. Cherny NI, Foley KM. Current approaches to the management of cancer pain: a
review. Ann Acad Med Singapore. 1994;23:139-59.
30. Meyer BR, Reidenberg MM. Clinical pharmacology and ageing. In: EvansJG,
WilliamsTF, editors. Oxford textbook of geriatric medicine Oxford: Oxford University Press; 1992. p. 107-16.
31. Wynne CF, Ling S, Remsburg R. Comparison of pain assessment instruments in
cognitively intact and cognitively impaired nursing home residents. Ger Nursing 2000;21:20-3.
32. Mathe A, Hahn MB. Pain Management in the geriatric patient: overview and case
33. Ripmonti C, Liliana G, et al. Switching from morphine to oral methadone in treating
cancer pain: what is the equianalgesic dose ratio? J Clin Oncol. 1998;16:3216-3221
34. Foley,KM, Houde RW. Methadone in cancer pain management: individualize dose and
titrate to effect. J Clin Oncol. 1998;16:3213 -3215
Article 1 Le présent règlement est établi en application des dispositions des articles R. 3634-1 et R. 3634-2 du Code le la Santé Publique. Il remplacetoutes les dispositions réglementaires antérieures relatives à l’exercice du pouvoir disciplinaire en matière de lutte contre le dopage. Article 2 Aux termes de l’article L. 3631-1 du Code de la Santé publique : “Il est i
Instructions for use NAME OF THE MEDICINAL PRODUCT : 32P-Sodium orto-phosphate for injection. 2. QUALITATIVE AND QUANTITITATIVE COMPOSITION : 32P Acidum phosphoricum 74 -370 MBq (2 - 10 mCi) or Phosphorus in the form of sodium phosphate The product does not contain any antimicrobial additives. 3 . PHARMACEUTICAL FORM : Radiopharamceuticals - solution for injection. 4. CLINICAL P
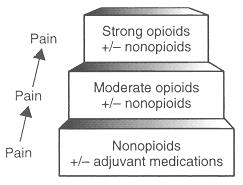 exhibit analgesic potential. Examples of adjuvant medications maybe anticonvulsants and antidepressants. Adjuvant medications may be started with step one and can be modified or tailored throughout the treatment.
exhibit analgesic potential. Examples of adjuvant medications maybe anticonvulsants and antidepressants. Adjuvant medications may be started with step one and can be modified or tailored throughout the treatment.