Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
Canine hypothyroidism – diagnostic dilemma but judicious diagnostic testing
Canine hypothyroidism – can we diagnose it?
Roger Powell MA VetMB DipRCPath Diplomate AVCP MRCVS
Powell Torrance Diagnostic Services, Unit 2a, Manor Farm Business Park, Higham
Hypothyroidism is generally accepted to be the most common endocrine
disorder in dogs. Yet the diagnostic tests available for this disease remain varied and debated, confirmation and definitive diagnosis of the disease therefore requiring a detailed knowledge not only of available tests, but also the pathophysiology of canine hypothyroidism and the many non thyroidal diseases that have a significant impact on the thyroid axis. This article will comprehensively but briefly review essential pathophysiology, outline potential testing and summarise possible ways of diagnosing this problematic lifelong but treatable condition. Pathophysiology:
The production, regulation and effects of thyroid hormones are very complex
and remain incompletely understood. An overview is provided below and in figure 1.
The hypothalamus produces Thyrotropin Releasing Hormone (TRH) that
permissively stimulates the anterior pituitary to produce and secrete Thyroid Stimulating Hormone (TSH- thyrotropin). TSH stimulates the production and release mainly of 3,5,3’,5’ tetraiodothyronine/thyroxine (T4) and 3,5,3’ triiodothyronine (T3) from the thyroid gland. Whilst T4 is the dominant product, T3 is the most metabolically active, T4 being variably deiodinised (by selenium dependent deiodinases) in many tissues, including the central nervous system and skin but especially the liver and kidney, to T3. T4 can also be deiodinised to 3,3’,5’ triodothyronine/reverse T3 (rT3) which is metabolically inactive, more so during illness or stress, both acutely and chronically. As they are lipophilic, only a fraction (≤ 1%) of thyroid hormones are free and active for conversion, cell entry and functioning, the majority being protein bound as a buffer for transportation to target tissues. In the dog this is primarily bound to thyroxine binding globulin (TBG), but also to prealbumin (transthyretin), albumin, high density lipoprotein 2 and a very low density lipoprotein. This protein carrier system (“Pr”, figure 1) appears species specific. Generally domestic animals seem to have relatively lower protein bound levels, higher free hormone levels and more rapid hormone metabolism relative to humans. Hence replacement supplementation can typically require higher and often more frequent (twice daily) dosing. Both T4 indirectly (via intracellular conversion to
T3 in the pituitary) and T3 directly have a negative feedback effect, reducing the production and secretion of TSH from the pituitary gland.
T4 & T3 -
The canine thyroid gland has two discrete lobes, typically found either side of
the cranial trachea, although (ectopic) thyroid tissue can be found anywhere from the oral to thoracic cavities. It has numerous follicles that produce and store colloid which contains mainly thyroglobulin, a glycoprotein that acts as an iodine ‘storage trap’ and where iodine is enzymatically converted (by thyroid peroxidase primarily) to T4 and T3.
Canine hypothyroidism is most commonly (>95%) primary, involving
destruction/loss of the thyroid gland itself by immune mediated destruction (lymphocytic thyroiditis) or idiopathic atrophy. Much rarer primary aetiologies are neoplasia, iatrogenic or juvenile/congenital disease (cretinism). Secondary (pituitary) or tertiary (hypothalamic) hypothyroidism is much rarer, accounting for less than 5% of cases, tertiary disease not being reported in the literature.
The loss of thyroid hormones has wide ranging effects, clinical signs being
non specific and seen in one or more body systems, typically arising gradually and insidiously. Signs include
• Skin: alopecia (especially bilateral and tail/neck areas), seborrhoea sicca or
oleosa, hyperpigmentation, recurrent/chronic secondary infections, rarely myxoedema (skin thickening due to abnormal deposits).
• Neuromuscular: exercise intolerance, weakness, unilateral/bilateral facial
nerve paralysis, vestibular disease, lower motor neuron disorders, behavioural, rarely coma.
• Cardiac: bradycardia, reduced contractility and dysrhythmias
• Reproductive: primarily female, irregular or prolonged oestrus or anoestrus
• Ocular: corneal ulceration & lipid dystrophy, uveitis
• Gastrointestinal: constipation or diarrhoea
Clinicopathological findings include: elevated cholesterol & elevated triglyceride primarily, elevated creatine kinase & liver enzymes and/or a mild normocytic normochromic anaemia being less commonly seen.
These are all non specific findings but the presence of more than one
consistent clinical sign in different body systems, especially with supportive clinicopathological data, certainly warrants further specific thyroid testing. Thyroid testing:
Serum samples are universally used and appropriate for all possible thyroid
tests, but plasma, such as heparin or EDTA, can be used with some methods and tests. Testing methods include radioimmunoassay (RIA) and various enzyme immunoassays (EIAs), the latter using chemiluminescence and various spectrophotometric reactions for automation and speed. RIA remains the gold standard and is generally the most precise, accurate and sensitive. However, it is only available in a limited number of (commercial) laboratories and has associated health and disposal factors. For measuring total thyroxine it has largely been replaced by EIA technology. EIAs can have comparable and acceptable performance but suffer from more variable characteristics and interference, often being designed initially for humans and then adapted or validated to varying degrees for veterinary usage. This can be fine for certain species and methods, but one such assay is very unlikely to perform reliably and accurately in all species and situations, such as dogs versus cats. This is in part also due to the clinical situations in which they are being used. Dogs have (relative to humans) lower total thyroid hormone levels, and we are most commonly testing for very low levels in suspected hypothyroid cases. We therefore require a test that will ‘work well’ at low levels (<10-15 nmol/l). Conversely in cats we are looking more at diagnosing hyperthyroidism, and therefore the test must ‘work well’ at much higher levels (60-300 nmol/l). A single (human) EIA is very unlikely to do this. A combination of methods and tests can therefore be required to test appropriately in all situations. These are significant factors that are too often overlooked or forgotten, resulting in erroneous results, diagnoses and even inappropriate therapy. A few studies have looked at certain EIAs compared to a standard RIA, in dogs and cats respectively finding that 62% and 50% would have been inappropriately treated and investigated based upon the EIA result. However, other studies have found very good agreement, with only 5% of cat and dog samples being erroneously interpreted. Each test methodology must be critically evaluated and used especially if being used for many species.
• Total Thyroxine (TT4): Reduced levels are expected in hypothyroidism, and therefore a result that is normal means hypothyroidism is much less likely but not excluded. However there are many other diseases, such as chronic renal failure or infections, which also lower
TT4 – so called ‘euthyroid sick syndrome’. A sole low TT4 is not therefore diagnostic of hypothyroidism. Other factors, such as strenuous exercise, can increase TT4 levels. Many exogenous drugs can have dramatic effects, the exact mechanism(s) being unclear but likely related to reduced production, a reduced protein bound fraction and/or altered peripheral metabolism. Common examples include (potentiated) sulphonamides, (immunosuppressive) glucocorticoids and (long term) phenobarbitone. Sulphonamides, especially at higher doses, can cause a genuine but reversible hypothyroid state. Other common drugs evaluated, including many NSAIDs and propanolol, can have minor effects but these are unlikely to be clinically significant. Exogenous drug effects should always be considered if being administered when testing, or ideally withdrawn if possible for at least 3-4 weeks before thyroid testing.
Breed can have a significant influence. Greyhounds are exemplified, but
‘sight and sled hounds’ in general seem to be similar. These breeds typically have a low-normal to (very) low TT4 level relative to most reference intervals (approximately 90% young greyhounds having below reference interval levels). Circulating autoantibodies against T4 (T4AAs) are estimated to be present
in 15% of hypothyroid dogs and these will falsely elevate TT4 levels in most methods, but in some will artificially reduce it. In terms of all samples tested for TT4 levels, estimates for significant T4AA effects are <1%.
• TSH/Thyrotropin: Elevated levels are expected in hypothyroidism. Whilst this is a diagnostic screening test in humans, the canine specific TSH assay is not sufficiently sensitive, accurate or precise. This is compounded by the fact that up to 38% of hypothyroid dogs do not show an elevation, whilst more rarely non thyroidal disease and drug effects can also elevate TSH. Breed does not appear to be significant, sight hounds studied to date having unremarkable levels relative to quoted reference intervals. Certain drugs, primarily gluocorticoids, probably reduce TSH levels in dogs as they do in humans, although current canine assays cannot reliably distinguish very small changes and low levels of TSH.
• Free T4 (fT4): fT4 levels should be low in hypothyroidism. This measures only the free non protein bound fraction of T4 in the serum/plasma. It can be measured either by equilibrium dialysis (ed) or solid phase radioimmunoassay (also known as analog assays). Only the former is recommended as the latter underestimates the fT4 levels in dogs. This test though takes more time as the method requires diffusion of T4 through a membrane that prevents protein movement, the amount of T4 (fT4ed) then being measured in the dialysate. It is much less widely available and more expensive than TT4.
This test is not affected by autoantibodies and levels are less commonly
reduced by non thyroidal illness or exogenous drug effects; examples that do though include sulphonamides, glucocorticoids, clomipramine and phenobarbitone. Conversely, levels can be artificially elevated by certain drugs and factors, principally thought to be by altered protein binding, examples including furosemide and free fatty acid supplements. Greyhounds (and probably sled / sight hounds) also have much lower fT4 levels, similar to TT4 but less commonly – estimated at 20% in greyhounds.
• Total triiodothyronine (TT3): TT3 levels should be low in hypothyroidism. Test methods are similar to TT4 and suffer from similar technical factors such as circulating autoantibodies (T3AAs). However, TT3 levels are more commonly affected for various reasons. T3AAs are seen more frequently, estimated at 34% in hypothyroid dogs or approximately 4- 5% of all serum samples tested. TT3 is also derived from peripheral deiodinisation of T4, regulation of which varies significantly and differently (compared to TT4) with non thyroidal illness/diseases (sick euthyroid syndrome), as well as by exogenous drug effects. TT3 levels are unremarkable in many hypothyroid dogs (up to 90%), decreased similar to TT4 in non thyroidal illness, and variably affected by drugs: phenobarbitone had no effects whilst anti-inflammatory glucocorticoids reduced TT3, sulphonamides also reducing levels. Greyhounds and sled hounds (and probably sight hounds) have very variable levels of TT3, but these are typically unremarkable to high-normal, although one study has reported low TT3 levels.
• Free T3 (fT3):
Assays are principally the same as the fT4, with similar limitations. Detailed studies though on fT3 levels in health alongside drug effects and non thyroidal diseases are lacking, but are likely to be similar to fT4 as well as affected by peripheral deiodinisation rates and metabolism.
• Reverse T3 (rT3):
This is measured by RIA but is very rarely performed, only being available in very few (research) laboratories. Whilst in theory hypothyroid dogs would have low levels compared to normal or elevated levels in non thyroidal illness and possibly with drug effects, the situation in humans is that there is considerable overlap between hypothyroid and euthyroid states. The situation in dogs is unknown.
• Anti-thyroglobulin autoantibodies (TgAA):
Much (50-80%) of primary canine hypothyroidism is due to thyroid destruction via immune mediated lymphocytic thyroiditis, resulting in detectable levels of autoantibody against thyroglobulin. They are more commonly seen in females and there appears to be a genetic predisposition with certain breeds being over-represented. TgAA can be detected in a variety of ways, including complement fixation, immunoprecipitation and EIAs, the last being the most common and widely utilised today, results being reported as positive, inconclusive or negative. Initially these had variably high false positive rates, but newer methods are much better, evaluation of an EIA compared to histopathologically confirmed thyroid disease giving a sensitivity and specificity of > 90%. A positive TgAA result supports thyroid disease but does not assess thyroid function and dogs with confirmed hypothyroidism can be negative. Euthyroid dogs (estimated prevalence 2-3%) can also be positive, recent vaccination apparently producing a false positive result. Long term studies are lacking but 20% of dogs with positive TgAA developed changes in fT4 and/or TSH consistent with hypothyroidism in 1 year, 15% seroconverted with no change in fT4 and TSH levels, the remaining 65% staying positive or inconclusive with no change in fT4 and TSH. One could extrapolate that most TgAA positive dogs
become hypothyroid in 4 years, but this assumes similar progressive disease and information to support this is lacking or unknown.
• Anti-T4 (T4AA) & anti-T3 (T3AA) autoantibodies:
These are found in a proportion of lymphocytic thyroiditis hypothyroid cases, but much less so TgAA. One study found 6% of samples from hypothyroid cases had circulating T4AA and/or T3AAs, typically also having TgAA although the converse is not evident. Their presence will falsely elevate most TT4 and TT3 assays as described previously, but clinically significant effects are estimated at <1% for TT4.
• Dynamic Stimulation Tests:
Stimulation testing of a gland’s hormonal production arguably remains the ‘gold
standard’ for diagnosing any hypofunction including hypothyroidism. Previously the TSH response to exogenous pharmaceutical (bovine) TSH was widely used. With this no longer available, alongside the development and improvement in testing basal levels of TT4, fT4 and TSH, some argue stimulation tests are no longer routinely required. The validation of recombinant human TSH as an alternative has allowed this test to be used once more. It is though substantially more expensive than bovine TSH and is less widely available. Compared to basal tests, its use may therefore be confined to cases where they are equivocal or there is a significant non thyroidal disease/drug effects. Even when stimulated, there remains a significant overlap in a euthyroid axis’ response and that of a hypothyroid axis, evident previously with bovine TSH, especially early in the disease. Whilst each response should be interpreted relative to their own laboratory’s reference values pre and post, as a general rule, in (sick) euthyroid cases, TT4 levels after stimulation are 1.5-2 times basal and often in the upper half of the reference interval. Hypothyroid cases typically do not stimulate significantly, pre and post levels being essentially unchanged.
TRH stimulation response has been similarly used in the past and also in theory to
diagnose rarer secondary hypothyroidism, looking at changes in the expected increase of TSH and TT4 levels. Studies have shown little to no improvement in accuracy (sensitivity and specificity) compared to a combination of basal tests such as TT4, TSH and fT4, and several studies have shown many false positives. Current canine TSH assays are not sensitive enough for discrimination of secondary hypothyroidism based upon TSH levels and primary canine hypothyroid cases also seem to have reduced responses.
Other diagnostic methods:
Nuclear scintigraphy using radioiodine or technetium has been proposed but
carries associated radioactive risks, has very limited availability and is expensive.
Thyroid gland biopsy will confirm lymphocytic thyroiditis, but early follicular
changes can be subtle and missed with idiopathic atrophy, the biopsy carrying inherent general anaesthetic risks and possibly damage to adjacent tissue such as the parathyroid glands or laryngeal nerve.
Thyroid gland ultrasonography has been used and one study showed
significant differences between hypothyroid glands and sick euthyroid or normal healthy glands. No difference was evident in TgAA positive versus TgAA negative hypothyroid cases. However, grouping into diagnostic categories was controversial and biased so the distinction may be less clear cut. There also seems to be breed or
size related changes in the thyroid gland size that will have to taken into account. This modality though may offer future testing when more fully evaluated.
Trial supplementation therapy is often anecdotally used. Whilst response to
therapy is certainly part of the diagnostic confirmation, taking a period of weeks to months dependent on the presenting signs, its use as a ‘screening test’ cannot be recommended. This is in part due to a variety of possible non specific signs ‘responding’ to increased thyroid levels whatever the underlying cause, as well as the inherent possibility of inappropriately medicating a dog for life with an associated albeit uncommon risk of thyrotoxicosis. Trying to diagnose/confirm hypothyroidism later after any such supplementation is very difficult if not impossible and probably more problematic than initially performing a variety of tests to confirm disease before supplementation. What test(s) should we use?
No single test, be it TT4, fT4 or TSH, is sensitive and specific enough to
advocate its use as a sole diagnostic screen to confirm hypothyroidism. Therefore ‘stepwise’ testing starting with one specific and/or sensitive test and then using others to provide diagnostic information cannot be recommended.
Frequently now, clinicians are offered a panel of thyroid tests, ranging from
TT4 with TSH to an extensive panel that may include TT4, TT3, fT4, fT3, T4AA & T3AA or TT4, fT4, TSH and TgAA. Using such extensive panels of more than four tests to diagnose or screen for hypothyroidism cannot seemingly be justified when detailed understanding of the individual hormone levels and fractions are incomplete at best and where assessed, offer no greater accuracy or diagnostic capability over more conventional and ‘minimal test panels’. This is especially true if there are financial or practical constraints.
The following are general guidelines that may be advised in some of the more
common situations to diagnose hypothyroidism from a single sample. They are by no means absolute, with serial testing, further testing and possibly dynamic stimulation testing potentially being required in certain situations. In some situations there is too little information to propose a ‘best’ approach. Supporting clinical signs, history and routine clinicopathological data should always be present.
1. Initial presentation of a hypothyroid case:
TT4 and TSH
2. Suspected hypothyroid with non thyroidal disease evident:
fT4 and/or TT4 with TSH +/- TgAA
3. Suspected hypothyroid with recent significant drug administration:
Stop drugs for 4-6 weeks, then fT4, TT4 and TSH +/- TgAA
4. Genetic screening and possibly monitoring certain breed individuals:
TgAA, followed by periodic TT4 or fT4 if positive
5. Suspected hypothyroid sight hounds and greyhounds:
fT4 and TSH, +/- TT3, +/- TSH stimulation? Each individual case must be assessed for supporting clinical signs and findings and, taking into account the drug history, specific testing then performed that will maximise the ‘diagnostic potential’ cost effectively and practically. No single test or single panel of tests appropriately covers all situations and presentations.
Das Noonan-Syndrom Gregor Schlüter1, Malte Rossius1, Armin Wessel2, Barbara Zoll1 Zusammenfassung tyrosin-Phosphorylase, die eine zentrale Regu- that are set low and rotated posteriorly, steno- latorfunktion in fast allen Signaltransduktions- sis of the pulmonal valve and short stature. Das Noonan-Syndrom ist ein Dysmorphie-Syn- wegen von Wachstumsfaktoren ausübt. Diese
 Canine hypothyroidism – can we diagnose it?
Canine hypothyroidism – can we diagnose it?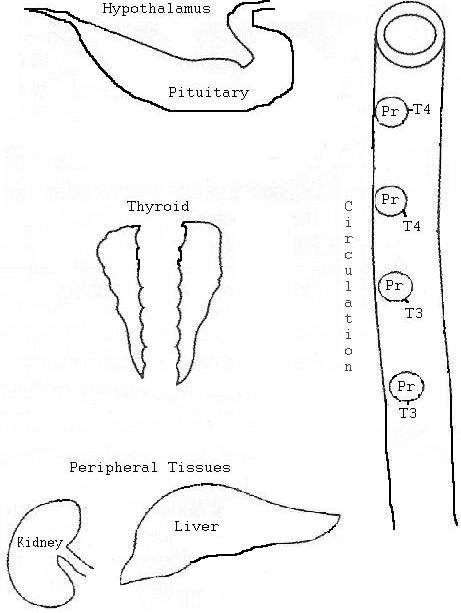 T3 in the pituitary) and T3 directly have a negative feedback effect, reducing the production and secretion of TSH from the pituitary gland.
T4 & T3 -
T3 in the pituitary) and T3 directly have a negative feedback effect, reducing the production and secretion of TSH from the pituitary gland.
T4 & T3 -