Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
Ritcare.com
Rehabilitation Institute of Texas RIT Patient Initial Visit Information Sheet
Patient Name: ____________________________ Age: _______ Gender: M F
Referring Physician: _______________________ Primary Care Physician: ___________________
Reason for the visit: _______________________________________________________________
1. When did your present problem start? _____________________________________________
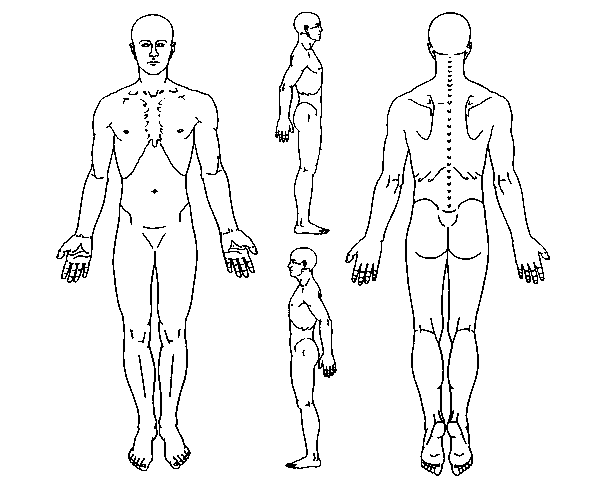
2. How did this problem start? 3. Pain Diagram ___________________________________ On the picture below, please mark all the area of your pain: ___________________________________
4. Pain level: (no pain: 0, worst pain: 10)
Pain right this moment: ________________
Average pain over last 24 hours: _________ 5. Pain quality: (Check below that best describe what you pain feels like)
-Throbbing -Shooting -Stabbing -Sharp -Cramping -Burning -Tingling -Aching
6. Pain pattern: -Continuous -Rhythmic -Comes and goes
7. What can make your pain worse?
-Sitting -Standing -Walking -Lifting -Cough/Sneeze -Lying flat on back -Others:
8. What can make your pain better?
9. Do you have any of following symptoms when you have pain?
-Nausea -Vomiting -Visual disturbance -Weakness -Incontinence -Shortness of breath -Others:
10. Do you have difficulty sleeping because of pain? -Yes -No How many hours a day on average can you sleep recently? ___________________________
11. Have you ever been treated for a different pain condition? -Yes -No If yes, please describe where and when: ___________________________________________________________________________
12. Previous treatment for your current pain -Yes -No Have you ever been to another pain clinic? If yes, Name of the clinic______________ Dr.’s name ________________ Name of the clinic______________ Dr.’s name ________________ Name of the clinic______________ Dr.’s name ________________
-Yes -No Have you had previous injection for your pain? If yes, what kind of injection? ________________________________ Did they help? _________________________________________ -Yes -No Have you had previous surgery for pain? If yes, please explain: _____________________________________
-Yes -No Have you had physical or occupational therapy for pain?
-Yes -No Have you tried acupuncture for pain relief? If yes, was this helpful? _____________
-Yes -No Have you seen a chiropractor for pain relief? If yes, was this helpful? ____________
13. Pain medications Please list all the pain medications you are taking currently (including any nonprescription Medications such as Tylenol, Bengay, etc.)
Please list all the pain medications you took before but for some reasons you have stopped taking these Medications (e.g. Ibuprofen, Naproxen, Motrin, Advil, Predinison, Medrol-dose pack, Vioxx, Celebrex, Bextra, Valium, Flexeril, Baclofen, Neurontin, Tegretol, Elavil, Celexa, Darvon, Darvocet, Roxicet, Percocet, Oxycodone, Oxycontin, Kadian, Ultram, Ultracet etc.).
14. Other medications Are you currently taking other medications for other non-pain health conditions? -Yes -No If yes, please list (be sure to include nonprescription, eye drops, topical drugs such as vitamins
How do you take (example: one tablet twice daily)
15. Please list any drug allergy
16. Past medical history (Please check any of the following problems that you have had)
___ High blood pressure ___ Tuberculosis ___ Diabetes/Hypoglycemia ___ Stomach ulcers
___ Heart Murmur ___ Hepatitis ___ Arrhythmia ___ HIV infection ___ Heart attack ___ Seizure ___ Chest pain ___ Stroke ___ Asthma ___ Fainting ___ Cancer ___ Bleeding disorders ___ Kindney infection/stone ___ Depression ___ Swelling of toe or finger joints ___ Psychosis ___ Thyroid disease ___ Others:
17. Past surgical History (Please list all previous surgeries)
Date (Month/Year) Procedures _______________ __________________________________________________________ _____________ __________________________________________________ _____________ __________________________________________________ _____________ __________________________________________________
18. Social History Are you currently: Single Married Widowed Divorced Separated -Yes -No Do you smoke cigarettes? If yes, ____ packs per day for ____ years? Quit____ -Yes -No Do you drink alcohol beverages? If yes, how much per day? ____ -Yes -No Do you use street drugs? -Yes -No Are you working? How many hours a day? 0 1 2 3 4 5 6 7 8 more If not, when was your last work? Date: _______________ -Yes -No Is this a worker’s compensation case? -Yes -No Are you involved in a lawsuit related to your pain condition? -Yes -No Are you interested to return to work soon, if you are not working currently?
19. Family History Do you have a family history of (Circle all that applies)? -Diabetes -Tuberculosis -Heart attacks -Rheumatoid arthritis -back problems -Others: ______________
20. Review of System Do you have any of the following symptoms recently? Constitutional: -Fever -Weight loss -Sleep difficulty Cardiovascular: -Chest pain -Shortness of breath Respiratory: -Cough -Wheezing -Asthma -Breathing difficulty Gastrointestinal: -Nausea -Vomiting -Abdominal pain -Constipation Genitourinary: -Urine incontinence -Urinary frequency -Pain on urination -Impotence Female reproduction: -Pregnant -Abnormal bleeding Skeletal muscle: -Back pain -Neck pain -Joint pain -Joint swelling Neurological: -Headache -Arm weakness -Hand/leg numbness -Leg weakness -Gait unsteadiness Vision: -Visual difficulty -Glaucoma -Eye pain ENT: -Ear infection -Ear pain Skin: -Rash -Ulcer -Skin cancer -Infection -Hypersensitivity -Color change -Temperature change Immunology: -Rheumatoid arthritis -SLE Psychological: -Depression -Anxiety -Pain attach -Suicidal ideation
SURGERY HOURS GRANGETOWN OUT OF HOURS SERVICE Our surgery is closed between 6pm and 9am, but you can still receive advice or information. Please telephone NHS Direct on 0845 4647. For urgent medical care please telephone 0845 603 3131. Middlesbrough Primary Care Trust is commissioning our out of hours service and can also be contacted on www.nhsdirect.nhs.ukDetails of all pri
Arab British Academy for Higher Education Event Day It’s finally here! The big day! After all the planning, prodding and producing, you’re probably feeling a range of emotions from excitement to nervousness to sheer terror . Use those feelings to keep your energy up (you’re going to need every ounce of it today!) but don’t give in to the jitters. To ensure the day
 Rehabilitation Institute of Texas
Rehabilitation Institute of Texas