Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
Training.cdsafe.com.cn
E m e r g i n g T r e a t m e n t s a n d T e c h n o l o g i e s O R I G I N A L XENical in the Prevention of Diabetes in Obese Subjects (XENDOS) Study A randomized study of orlistat as an adjunct to lifestyle changes for the prevention of type 2 diabetes in obese patients ARL S. TORGERSON, MD, PHD MARK N. BOLDRIN, MS
with type 2 diabetes are either overweight
ONATHAN HAUPTMAN, MD LARS SJ ¨OSTR ¨OM MD, PHD
or obese (5). The World Health Organi-zation has estimated that the number ofadults with diabetes will more than dou-
OBJECTIVE — It is well established that the risk of developing type 2 diabetes is closely
ble from an estimated 143 million in 1997
linked to the presence and duration of overweight and obesity. A reduction in the incidence of
type 2 diabetes with lifestyle changes has previously been demonstrated. We hypothesized that
adding a weight-reducing agent to lifestyle changes may lead to an even greater decrease in body
weight, and thus the incidence of type 2 diabetes, in obese patients. RESEARCH DESIGN AND METHODS — In a 4-year, double-blind, prospective study,
with an 80% reduction in the 8-year inci-
we randomized 3,305 patients to lifestyle changes plus either orlistat 120 mg or placebo, three
dence of diabetes (6). The Finnish Diabe-
times daily. Participants had a BMI Ն30 kg/m2 and normal (79%) or impaired (21%) glucose
tolerance (IGT). Primary endpoints were time to onset of type 2 diabetes and change in body
weight. Analyses were by intention to treat.
also demonstrated that modest weightloss achieved by lifestyle changes (diet
RESULTS — Of orlistat-treated patients, 52% completed treatment compared with 34% of
and exercise) can significantly reduce the
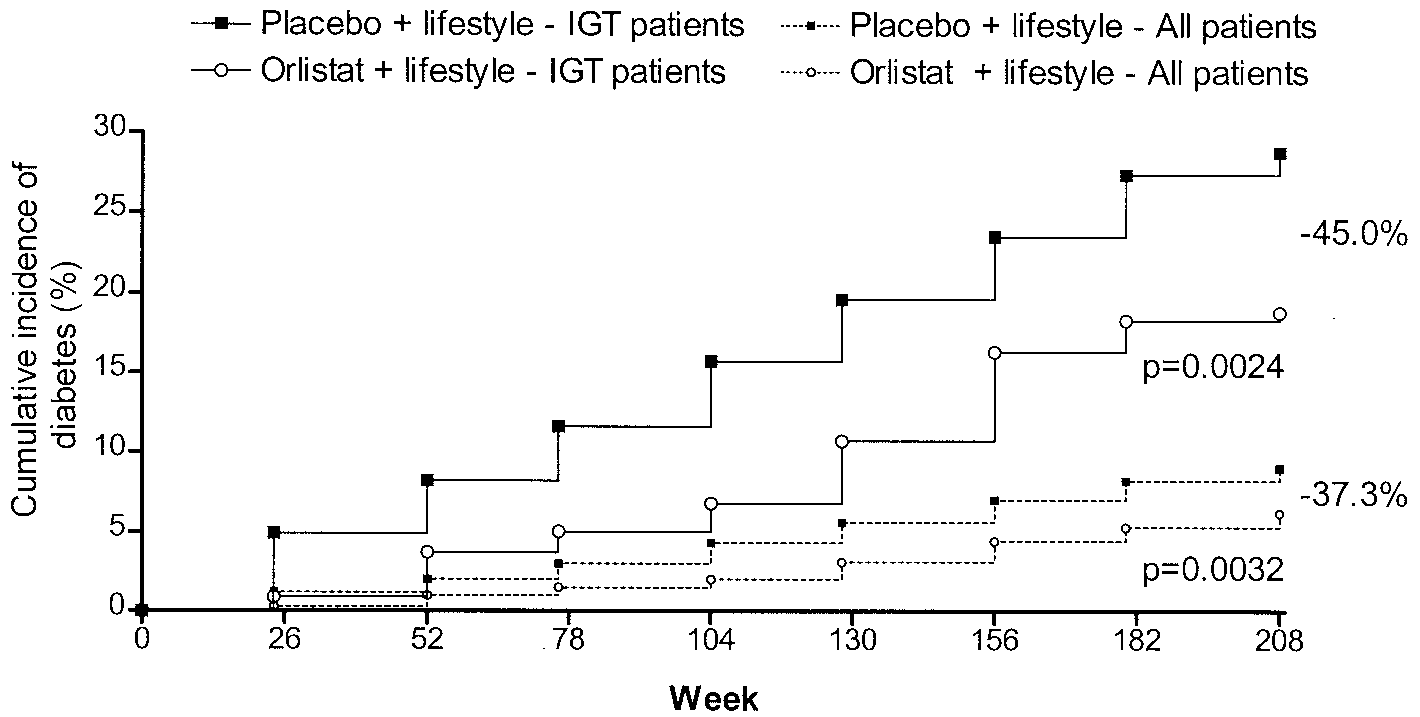
placebo recipients (P Ͻ 0.0001). After 4 years’ treatment, the cumulative incidence of diabetes
risk of developing type 2 diabetes in obese
was 9.0% with placebo and 6.2% with orlistat, corresponding to a risk reduction of 37.3% (P ϭ
0.0032). Exploratory analyses indicated that the preventive effect was explained by the differ-ence in subjects with IGT. Mean weight loss after 4 years was significantly greater with orlistat
(5.8 vs. 3.0 kg with placebo; P Ͻ 0.001) and similar between orlistat recipients with impaired
obese patients with IGT receiving orlistat
(5.7 kg) or normal glucose tolerance (NGT) (5.8 kg) at baseline. A second analysis in which the
treatment has shown that this weight loss
baseline weights of subjects who dropped out of the study was carried forward also demonstrated
agent may also be effective in reducing the
greater weight loss in the orlistat group (3.6 vs. 1.4 kg; P Ͻ 0.001). CONCLUSIONS — Compared with lifestyle changes alone, orlistat plus lifestyle changes
resulted in a greater reduction in the incidence of type 2 diabetes over 4 years and produced
greater weight loss in a clinically representative obese population. Difference in diabetes inci-
to determine the long-term effect of orl-
dence was detectable only in the IGT subgroup; weight loss was similar in subjects with IGT and
istat, a gastrointestinal lipase inhibitor, in
combination with lifestyle changes in re-
Diabetes Care 27:155–161, 2004
ducing progression to type 2 diabetes andbody weight over 4 years in obese, non-diabetic patients who had either normalglucose tolerance (NGT) or IGT. Second-
Obesity is a serious health concern studies(2–4)showthattheriskofdevel- aryaimsweretodeterminetheeffectof
oping type 2 diabetes is closely linked to
orlistat treatment on weight-related met-
and obesity. Indeed, ϳ90% of individuals
● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ●
and the safety and tolerability of orlistat
From the 1Department of Body Composition and Metabolism, Sahlgrenska University Hospital, Go¨teborg,
Sweden; and 2Hoffmann-La Roche, Nutley, New Jersey.
Address correspondence and reprint requests to Professor Lars Sjo¨stro¨m, Department of Body Composi-
tion and Metabolism, Vita Stråket 15, Sahlgrenska University Hospital, S-413 45 Go¨teborg, Sweden. E-mail:
RESEARCH DESIGN AND METHODS — XENDOS was a 4-year,
Received for publication 30 May 2003 and accepted in revised form 10 October 2003.
L.S. had full access to study data and is responsible for the decision to submit.
All authors participated in drafting the manuscript of this article. Abbreviations: BLCF, baseline observation carried forward; DPP, Diabetes Prevention Program; DPS,
Diabetes Prevention Study; IGT, impaired glucose tolerance; ITT, intention to treat; LOCF, last observation
carried forward; NGT, normal glucose tolerance; OGTT, oral glucose tolerance test; XENDOS, XENical in the
sign and the system for centralized patient
prevention of Diabetes in Obese Subjects.
A table elsewhere in this issue shows conventional and Syste`me International (SI) units and conversion
2004 by the American Diabetes Association.
scribed previously (10). The study proto-
DIABETES CARE, VOLUME 27, NUMBER 1, JANUARY 2004
Orlistat and diabetes prevention
centage used against that dispensed.
to have 90% power of detecting a signifi-
ration of Helsinki. All study subjects gave
type 2 diabetes was based on a single 2-h
Eligible patients were 30 – 60 years of age,
quired to have nondiabetic glucose toler-
used for the primary end point of time to
onset of type 2 diabetes, consisted of all
randomized patients who received at least
dence rates of type 2 diabetes were calcu-
mmol/l) (11). Patients with IGT were also
with type 2 diabetes remained in the study
eligible for inclusion, and the criteria for
and had fasting whole blood glucose levels
cose 6.7–10.0 mmol/l (11). (These crite-
week 24), fewer patients were included in
sisted of all patients who received at least
one dose of orlistat with a safety follow-up.
ters, as well as plasma levels of the fat-
results to receive either placebo or orlistat
end point of time to onset of diabetes were
in a one-to-one ratio, using a centralized
min D, vitamin E [␣-tocopherol], and vi-
randomization procedure and schedule.
placebo and orlistat capsules. The inves-
fore taking study medication and were an-
developing diabetes. The hazard ratio was
each patient that contained the identity of
factors of baseline glucose tolerance (IGT
of age and BMI on the relative risk of de-
subgroups were categorized at baseline as
change in body weight after 4 years’ treat-
lost during the preceding months. Partic-
patients with IGT or NGT at baseline.
ipants received dietary counseling every 2
baseline as the response variable and cen-
thereafter. Patients were also encouraged
to walk at least 1 extra kilometer a day in
baseline NGT subjects) time to onset of IGT.
interaction as the independent variables.
addition to their usual physical activity.
Baseline values were used as covariates.
All patients kept physical activity diaries.
Based on a literature survey and previous
experience, the hazard ratio for the onset
alyzed body weight changes categorically.
of type 2 diabetes was assumed to be two-
Descriptive statistics for all secondary pa-
to-one for placebo-to-orlistat. Therefore,
a two-sided log-rank test would require a
used observed data. Descriptive statistics
DIABETES CARE, VOLUME 27, NUMBER 1, JANUARY 2004
Torgerson and Associates Table 1—Demographic and clinical characteristics of the study participants at baseline ITT population
treatment (14 and 20%, respectively) andinsufficient therapeutic response (8 and19%, respectively).
baseline in age, weight, BMI, or the male-
For the ITT population, the actual calorie
deficit over the 4 study years was similar
Ϫ673 Ϯ 825 kcal/day in orlistat-treated
patients and Ϫ744 Ϯ 935 kcal/day in pla-
administration from first dose until treat-
patients and 92.8% for placebo patients. Incidence of type 2 diabetes. During 4
Data are means Ϯ SD, unless otherwise noted. AUC, area under the curve, BP, blood pressure.
years of treatment, orlistat plus lifestylechanges significantly decreased the pro-gression to type 2 diabetes compared with
for change in body weight and categorical
[52%] vs. 564 of 1,655 [34%]; P Ͻ
0.0001). For both the orlistat and placebo
P ϭ 0.0032). Cumulative incidence rates
after 4 years were 6.2 vs. 9.0% (Fig. 1).
otherwise noted. Observed, LOCF, andbaseline observation carried forward(BLCF) (13) methods were used for hy-pothesis testing of quantitative parameters. RESULTS — From August to Decem- ber 1997, 3,305 study participants were randomized to treatment with orlistat plus lifestyle changes (n ϭ 1,650) or pla- cebo plus lifestyle changes (n ϭ 1,655), of which 3,304 were treated. The last 4-year examination was completed in February 2002. The ITT population comprised 1,640 (orlistat group) and 1,637 (placebo group) patients. The baseline demo- graphic and clinical characteristics of the two treatment groups were similar (Table 1). The safety population comprised 1,649 and 1,655 patients, respectively. A
Figure 1—Cumulative incidence of diabetes by study group in all obese patients (IGT or NGT at
greater number of orlistat-treated patients
baseline) and only in obese patients with IGT at baseline. The decrease in the risk of developingdiabetes with orlistat plus lifestyle compared with placebo plus lifestyle is indicated. P values
DIABETES CARE, VOLUME 27, NUMBER 1, JANUARY 2004
Orlistat and diabetes prevention
treatment, the relative risk of developingtype 2 diabetes was greater in patientswith IGT than in those with NGT, in menthan in women, in older than in youngerindividuals, and in individuals with ahigher BMI (Table 2). Weight loss was sig-nificantly greater with orlistat than pla-cebo in both patients with IGT at baseline(5.7 kg with orlistat vs. 3.0 kg with pla-cebo; P Ͻ 0.01) and patients with NGT(5.8 vs. 3.0 kg, respectively; P Ͻ 0.001).
Secondary efficacy parametersTreatment with orlistat plus lifestyle
Figure 2—Weight loss (means Ϯ SEM) during 4 years of treatment with orlistat plus lifestyle
changes resulted in early and significant
changes or placebo plus lifestyle changes in obese patients (LOCF data).
improvements in cardiovascular risk fac-tors that were sustained throughout the
nificantly lower with orlistat plus lifestyle
treatment (log-rank P ϭ 0.028). The cu-
circumference, and lipids (Table 3). Total
in the risk of developing diabetes with or-
mulative incidence rate of type 2 diabetes
after 4 years was 2.9% with orlistat versus
cholesterol ratio decreased significantly
Weight change. Mean weight loss was
more with orlistat than placebo, at both 1
significantly greater with orlistat than pla-
41% risk reduction (hazard ratio 0.593).
cebo at 1 year (10.6 vs. 6.2 kg; P Ͻ 0.001)
cholesterol increased less with orlistat.
and remained significantly greater at the
istat plus lifestyle changes significantly
P Ͻ 0.001) (Fig. 2). The least-square
mean difference between orlistat and pla-
single test (log-rank P ϭ 0.0024). Cumu-
treated individuals (27.6 vs. 30.5%, P ϭ
cebo groups after 4 years of treatment was
lative incidence rates after 4 years were
Ϫ2.7 kg (P Ͻ 0.001) by LOCF analysis. A 18.8 vs. 28.8% (Fig. 1), corresponding tosecond analysis in which the baseline
0.551). In addition, orlistat plus lifestyle
suming these subjects lost no weight) also
groups, with the exception of a higher in-
orlistat group (3.6 vs. 1.4 kg; P Ͻ 0.001).
0.0171). Cumulative incidence rates after
gastrointestinal events were mild to mod-
of treatment (52% of the orlistat patients
erate in intensity and occurred during the
and 34% of the placebo patients initially
early phase of treatment. During the first
52% risk reduction (hazard ratio 0.482).
cantly greater with orlistat than placebo at
tients experiencing at least one gastroin-
year 1 (11.4 vs. 7.5 kg; P Ͻ 0.001) and
testinal event with orlistat or placebo was
year 4 (6.9 vs. 4.1 kg; P Ͻ 0.001).
and insufficient to detect a statistically sig-
nificant difference compared with orlistat
achieved weight loss Ն5% after 1 year of
treatment (P Ͻ 0.001). A similar signifi-cant difference was apparent for patientsachieving a weight loss Ն10% (41.0%
Table 2—The effect of baseline strata on the relative risk of developing type 2 diabetes over 4
with orlistat vs. 20.8% with placebo; P Ͻ
years in patients, irrespective of treatment
0.001). For those patients who completed4 full years of treatment, 52.8 and 37.3%,
respectively, lost Ն5% of baseline bodyweight (P Ͻ 0.001) and 26.2 and 15.6%,
respectively, lost Ն10% of baseline body
Glucose tolerance: impaired versus normal
Exploratory analyses. The cumulative
incidence of type 2 diabetes diagnosed on
the basis of a repeat positive test was sig-
DIABETES CARE, VOLUME 27, NUMBER 1, JANUARY 2004
Torgerson and Associates Table 3—Mean change from baseline of cardiovascular risk factors at years 1 and 4 in all patients (observed data)
*P values apply to analyses by LOCF ITT, BLCF ITT, and observed data, except where indicated; †LOCF and BLCF ϭ NS; ‡LOCF and observed ϭ NS; §BLCF P Ͻ0.05; ʈBLCF ϭ NS; ¶observed ϭ NS; #calculated by trapezoid rule, including all areas above the line y ϭ 0, from measurements immediately before and 30, 60, 90,and 120 min after dose. AUC, area under the curve; BP, blood pressure.
portion of placebo-treated patients had at
with sustained and significantly better im-
pared with orlistat-treated patients (13 vs.
15%). Similar proportions of serious gas-
values was similar in the orlistat and pla-
demonstrated the long-term safety of orl-
trointestinal events occurred in the pla-
istat. The adverse events profile for orl-
cebo (n ϭ 32; 2%) and orlistat (n ϭ 32;
istat in this 4-year study was consistent
for vitamin E (3.2 vs. 0.5%, respectively).
patients and 8% of orlistat patients with-
ther step forward in the evolution of dia-
difference was primarily due to gastroin-
CONCLUSIONS — XENDOS was a
style changes in addition to receiving ei-
ducted in a representative cohort of obese
ther a placebo or an active treatment, in
treatment for all assessed fat-soluble vita-
demonstrated that orlistat plus lifestyle
istat. Early studies that were not fully con-
mins (vitamin A Ϫ0.22 vs. Ϫ0.19 mol/l,
P Ͻ 0.05; 25-hydroxyvitamin D Ϫ17.2
dence of type 2 diabetes over 4 years and
might reduce the incidence of diabetes in
vs. Ϫ13.0 nmol/ml, P Ͻ 0.001; vitamin E
Ϫ2.8 vs. 0.4 mol/l, P Ͻ 0.001; and vi- with placebo plus lifestyle changes. The beneficial effects of intensive lifestyletamin K Ϫ
0.08 vs. 0.07 g/l, P Ͻ 0.001),
overall effect of orlistat in preventing dia-
betes in our study population was primar-
(7) and DPP (8). In parallel, the DPP (8),
dence of diabetes in patients with baseline
ence range at all times during the 4-year
(19), and the Troglitazone in the Preven-
ference was discernable in this subgroup.
DIABETES CARE, VOLUME 27, NUMBER 1, JANUARY 2004
Orlistat and diabetes prevention
sults were obtained from this subgroup.
Palme´r, Bengt Petterson, Stephan Ro¨ssner,
with an intensive lifestyle group (8), drug
Gunnar Stro¨mblad, Karl-Axel Svensson, Rachel
treatment was less effective. In the current
Tengel, Bengt Vessby, Olov Wålinder, and Ro-
study, the placebo group was treated with
group with NGT at baseline, for which the
progression rate to type 2 diabetes turned
This work was presented at the 9th Interna-
tional Congress of Obesity in Sa˜o Paolo, Brazil,
amount of weight over the 4 years; adding
more weight loss and led to a significantly
lower risk of developing type 2 diabetes. References
our study, retention rates of 52% with or-
1. World Health Organization: Controlling
treated with placebo plus lifestyle changes
listat and 34% with placebo after 4 years
line], 2002. Available from http://www.
obesity studies with up to 2 years’ dura-
the intensive lifestyle intervention arms of
the DPS (3.5 kg) (7) and DPP (3.5 kg) (8).
fewer withdrawals with orlistat, possibly
Manson JE: Weight gain as a risk factor for
clinical diabetes mellitus in women. Ann
changes resulted in a significantly greater
3. Must A, Spadano J, Coakley EH, Field AE,
with that of the orlistat group. Because of
associated with overweight and obesity.
the event-based study design, the discon-
tinuation rate did not affect the power of
4. Hu FB, Manson JE, Stampfer MJ, Colditz
lifestyle changes over 4 years is of greater
lifestyle, and the risk of type 2 diabetes
repeat testing of patients with a positive
mellitus in women. N Engl J Med 345:790 –797, 2001
provements in cardiovascular risk factors.
The difference in weight loss between or-
vention: the case for action. Int J Obes Relat
repeat positive tests were not captured.
6. Sjo¨stro¨m CD, Peltonen M, Wedel H, Sjo¨s-
tro¨m L: Differentiated long-term effects
plus lifestyle group for our baseline IGT
and hypertension. Hypertension 36:20 –25,
those patients with data available from a
tude to that of the intensive intervention
repeat positive test show similar results
7. Tuomilehto J, Lindstro¨m J, Eriksson JG,
studies (11–14.4%) (7,8). The addition of
Uusitupa M: Prevention of type 2 diabetes
lifestyle changes significantly reduces the
incidence of type 2 diabetes in obese sub-
subjects with impaired glucose tolerance. N Engl J Med 344:1343–1350, 2001
was only apparent in the IGT subgroup.
Adding orlistat also significantly increases
risk reduction for orlistat plus lifestyle
weight loss in obese patients with either
gram Research Group: Reduction in theincidence of type 2 diabetes with lifestyle
vascular risk factors. Orlistat treatment is
intervention or metformin. N Engl J Med
mulative incidence rates provided, our re-
sults suggest that treating 10 patients with
orlistat plus lifestyle (rather than lifestyle
ing JP, Sjo¨stro¨m L: Effects of weight loss
Acknowledgments — This study was sup-
with orlistat on glucose tolerance and pro-
gression to type 2 diabetes in obese adults.
We would like to thank the following inves-
Arch Intern Med 160:1321–1326, 2000
powered to detect differences in progres-
tigators for their contributions to this study:
10. Torgerson JS, Arlinger K, Ka¨ppi M, Sjo¨s-
sion to type 2 diabetes in the overall co-
Krister Arlinger, Marcus Ka¨ppi, Ulf Adamsson,
tro¨m L: Principles for enhanced recruit-
Bo Berger, Jens Bo¨rretzen, Kerstin Brostro¨m,
ment of subjects in a large clinical trial:
hort, which was a clinically representative
Jan Carlstro¨m, Viveca Engblom, Jan Eriksson,
Per Gylle´n, Stefan Håkansson, Peter Hallgren,
ther NGT or IGT. Because of the high pro-
Thomas Kjellstro¨m, Ibe Lager, Mona Landin-
perience. Control Clin Trials 22:515–525,
portion of emergent cases in subjects with
Olsson, Owe Larsson, Ulrik Mathiesen, Bengt
IGT at baseline, significant exploratory re-
Mo¨ller, Peter Nicol, Per-Olof Olsson, Mats
11. World Health Organization: Prevention of
DIABETES CARE, VOLUME 27, NUMBER 1, JANUARY 2004
Torgerson and Associates Diabetes Mellitus. Geneva, World Health
ized controlled trial. JAMA 281:235–242,
Org., 1994, p. 17–18 (Tech. Rep. Ser., no.
16. Ro¨ssner S, Sjo¨stro¨m L, Noack R, Meinders
12. Lindroos AK, Lissner L, Sjo¨stro¨m L: Va-
lidity and reproducibility of a self-admin-
trial. Lancet 359:2072–2077, 2002
istered dietary questionnaire in obese and
risk factors after 2 years’ treatment with
20. Buchanan T, Xiang AH, Peters RK, Kjos
non-obese subjects. Eur J Clin Nutr 47:
Obesity Study Group. Obes Res 8:49 – 61,
13. Ware JH: Interpreting incomplete data in
ervation of pancreatic -cell function and
studies of diet and weight loss. N Engl
cological treatment of insulin resistance in
14. Sjo¨stro¨m L, Rissanen A, Andersen T,
high-risk Hispanic women. Diabetes 51:
BV: Effects of diet and exercise in prevent-
trolled trial of orlistat for weight loss and
21. Safer DJ: Diet, behavior modification and
tients. Lancet 352:167–172, 1998
Diabetes Study. Diabetes Care 20:537–
from a longitudinal perspective. South
18. Eriksson KF, Lindga¨rde F: Prevention of
22. Glenny AM, O’Meara S, Melville A, Shel-
mellitus by diet and physical exercise: the
prevention of obesity: a systematic review
and risk factor reduction in obese subjects
6-year Malmo¨ feasibility study. Diabetolo-
of the literature. Int J Obes Relat Metab Dis-
treated for 2 years with orlistat: a random-
DIABETES CARE, VOLUME 27, NUMBER 1, JANUARY 2004
Münsteri napló Kedves Olvasó!Ez a naplórészlet azért született, hogy első kézből lehessen olvasni egy teljes hasadék zárásának örömteli részleteiről. Amikor valaki megtudja (remélhetőleg még az anyaméhben levő gyermekéről), hogy hasadéka lesz, kétségbeesve keres információk után. Ekkor előbb-utóbb megtalálja ezt a honlapot, töméntelen sok véleményen és be
Hedy und Urs Wolfer, Bahnhofstrasse 39, 4571 LüterkofenTel.: 032 677 16 42, E-Mail: info@fa-kontaktgruppe.ch www.fa-kontaktgruppe.ch euro -ATAXIA-Konferenz am 25./ 26. September 2009, im Olid Meliá Hotel, Valladolid, Spanien. Euro-ATAXIA ist die Vereinigung der europäischen Ataxie-Organisationen, bei der unter vielen anderen auch die Schweizerische Muskelgesellschaft Mitglied ist. D
 Torgerson and Associates
Torgerson and Associates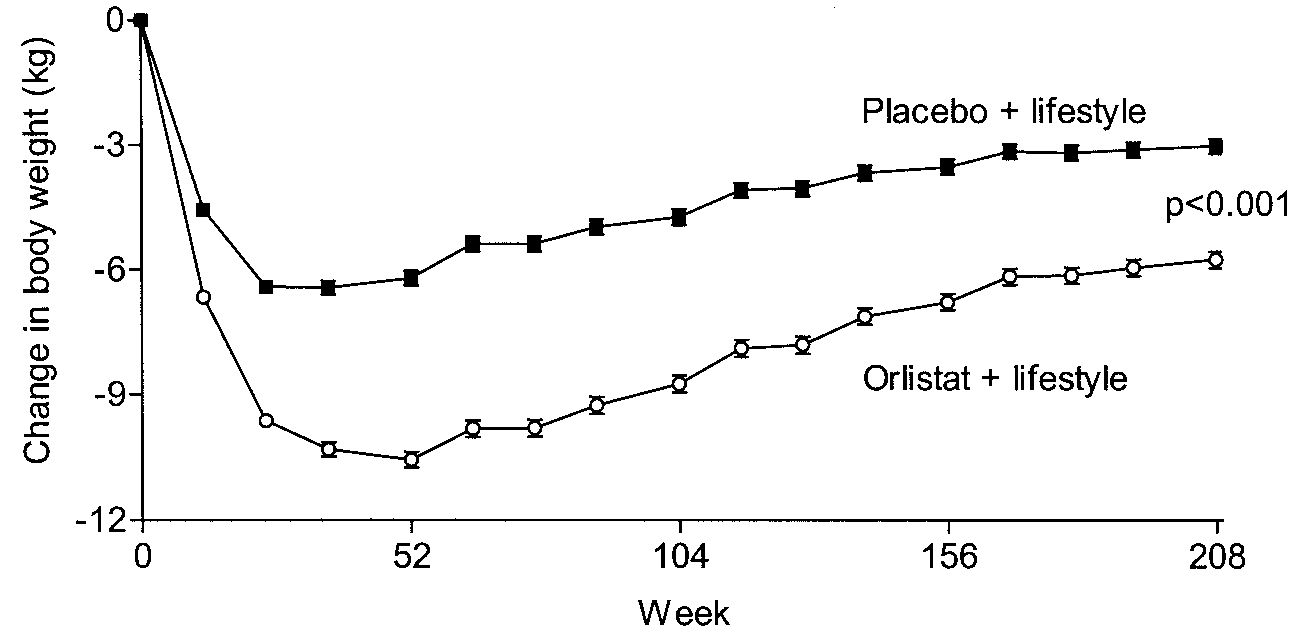 Orlistat and diabetes prevention
Orlistat and diabetes prevention