Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
University.asco.org
Antiandrogen Withdrawal Alone or in CombinationWith Ketoconazole in Androgen-Independent ProstateCancer Patients: A Phase III Trial (CALGB 9583)Eric J. Small, Susan Halabi, Nancy A. Dawson, Walter M. Stadler, Brian I. Rini, Joel Picus,Preston Gable, Frank M. Torti, Ellen Kaplan, and Nicholas J. Vogelzang
Antiandrogen withdrawal (AAWD) results in a prostate-specific antigen (PSA) response (decline in PSA
level of Ն 50%) in 15% to 30% of androgen-independent prostate cancer (AiPCa) patients. Thereafter,
adrenal androgen ablation with agents such as ketoconazole (K) is commonly utilized. The therapeutic
effect of AAWD alone was compared with simultaneous AAWD and K therapy. Patients and Methods
AiPCa patients were randomized to undergo AAWD alone (n ϭ 132), or together with K (400 mg orally
[po] tid) and hydrocortisone (30 mg po each morning, 10 mg po each evening; n ϭ 128). Patients who
developed progressive disease after AAWD alone were eligible for deferred treatment with K. Results Eleven percent of patients undergoing AAWD alone had a PSA response, compared to 27% of patients
who underwent AAWD and simultaneous K (P
ϭ .0002). Objective responses were observed in 2% of
patients treated with AAWD alone compared to 20% in patients treated with AAWD/K (P ϭ .02). There
was no difference in survival. PSA and objective responses were observed in 32% and 7%, respectively,
of patients receiving deferred K, and were more common in patients with prior AAWD response.
Treatment with K was well tolerated, and resulted in a decline in adrenal androgen levels, which rose at
Conclusion
K has modest activity in AiPCa patients, while AAWD alone has minimal activity. Adrenal androgen levels
fall with treatment with K and then climb at the time of progression, suggesting that progressive disease
while on K may be due to tachyphylaxis to the adrenolytic properties of K.
nadal androgen suppression at the time of
INTRODUCTION
initiating androgen deprivation (early use)
Prostate cancer is the most common cancer in
are modest at best [4]. The late addition of
men and will account for more than 30,000
an antiandrogen after initial failure of an-
deaths in 2003 [1]. The vast majority of deaths
drogen deprivation (late use) seems to result
are due to the development of metastatic dis-
in prostate-specific antigen (PSA) declines,
ease unresponsive to androgen deprivation.
and in some cases, objective responses [5].
flicts of interest are found at the end of
Androgen deprivation, with gonadal andro-
Thus, at one point or another, most patients
gen suppression with or without antiandro-
gen, has been the standard of care in pa-
treated with an antiandrogen. Despite an-
drogen deprivation, including the use of an
1940s [2] and is being increasingly utilized
antiandrogen, most patients will experience
in patients with less advanced disease [3].
disease progression. For patients with pro-
gressive disease, despite androgen depriva-
tion, withdrawal of antiandrogen has been
Information downloaded from jco.ascopubs.org and provided by at ASCO on April 5, 2011 from 206.205.123.242
Copyright 2004 American Society of Clinical Oncology. All rights reserved. Small et al
reported to result in a decline in PSA level of Ն 50% in 15%
PATIENTS AND METHODS
to 30% of patients [6-8]. The mechanism of this phenome-non has been attributed to alterations in the androgen sig-
Patients
naling cascade, including mutations in the androgen recep-
Eligible patients had histologically confirmed adeno-
tor (AR), resulting in the antiandrogen behaving as an
carcinoma of the prostate with progressive metastatic dis-
activator, not inhibitor, of the AR [9].
ease, as defined below, despite anorchid testosterone levels
The duration of decline in PSA observed with antian-
(Ͻ 50 ng/mL). Androgen deprivation therapy was required
drogen withdrawal (AAWD) is brief, with a median dura-
to include at least 4 weeks of ongoing therapy with an
tion of 3.5 to 5.0 months [6-8], after which further therapy
antiandrogen (flutamide, bicalutamide, or nilutamide).
is generally required. The mechanism by which prostate
Ongoing gonadal androgen ablation with a luteinizing
cancer patients develop disease progression after AAWD is
hormone-releasing hormone analog or orchiectomy was
not understood, but it has been postulated that persistence
required. For patients with measurable disease, progression
of a clone of cells with partial or full sensitivity to testoster-
was defined as a greater than 25% increase in the sum of the
one might be provided a growth advantage by androgen
products of the perpendicular diameters of all measurable
produced by the adrenal glands. If this were the case, it could be
lesions. For patients with “bone only” disease, a PSA greater
anticipated that adrenal androgen suppression would demon-
than 5 ng/mL, which had risen from baseline on at least two
strate some anticancer activity in this setting. An early report
successive occasions at least 4 weeks apart was required.
suggested that the addition of aminoglutethimide (an adrenal
Patients were required to have had metastatic disease dem-
steroid synthesis inhibitor) at the time of AAWD increased the
onstrated on imaging at some point during their history,
percentage of patients with a decline in PSA over that which
but were not required to have demonstrated metastases on
would be expected with antiandrogen alone [10].
imaging at the time of enrollment. Patients were excluded ifthey had received prior chemotherapy, immunotherapy,
Ketoconazole is an azole antifungal agent which exerts
experimental therapy, or prior treatment with ketocon-
its clinical effect through the inhibition of cytochrome P450
azole, aminoglutethimide, or corticosteroids if they had a
14a-demethylase, a catalyst of the conversion of lanosterol
Cancer and Leukemia Group B (CALGB) performance
to cholesterol. Ketoconazole has been in clinical use as an
status of more than 2, total bilirubin level greater than 1.5ϫ
antifungal agent for more than 20 years. In its initial use as
the upper levels of normal (ULN), or serum glutamic-
an antifungal agent, it was discovered that a proportion of
oxaloacetic transaminase level greater than 3ϫ ULN. Be-
men who used ketoconazole developed painful gynecomas-
cause of potential interactions with ketoconazole, no ongo-
tia, which was later found to be due to the suppression of
ing or concurrent use of terfenadine, astemizole, or
testicular and adrenal androgen production, and it was
cisapride was allowed. All participants signed an institu-
postulated that this adverse effect could be useful for pros-
tional review board–approved, protocol-specific, informed
tate cancer therapy. Several trials have evaluated the use of
consent form in accordance with federal and institutional
ketoconazole in patients with androgen-independent pros-
tate cancer (AiPCa), though most predated the use of PSAor an understanding of the AAWD syndrome [11-14]. Most
Treatment
recently, the use of ketoconazole after AAWD was reported
After registration, patients were randomized to AAWD
alone or AAWD ϩ ketoconazole by the CALGB Statistical
in a trial of 48 patients, 30 (63%) of whom demonstrated aՆ
Center. This study was neither blinded nor placebo con-
50% decline in PSA response. The decline of Ն 50% in
trolled. A conventional stratified random blocks design was
PSA was comparable in patients who had initially re-
used [16]. That is, within each stratum, patients were as-
sponded to AAWD and in those who had not initially re-
signed to the available two treatments in blocks of treatment
sponded to AAWD at 65% v 40%, respectively. Toxicity was
assignments so that an equal number of patients was as-
largely mild in these patients, consisting of grade 1 or 2
signed to each of the two treatment arms within each block.
nausea, fatigue, edema, hepatoxicity, and rash [15].
Randomization was stratified by four features that could
It was hypothesized that the simultaneous addition of
potentially affect the likelihood of response, both to AAWD
ketoconazole to AAWD would have additive anticancer
and/or ketoconazole therapy: (1) prior therapy with flut-
activity, simultaneously targeting the stimulating effects of
amide, bicalutamide, or nilutamide; (2) continuous or in-
antiandrogen and adrenal androgens. Hence, the principal
termittent treatment; (3) initial or delayed antiandrogen
goals of this study were to prospectively evaluate and com-
therapy; and (4) imaging studies positive or negative for
pare the effect of AAWD alone on PSA levels, compared
with simultaneous AAWD and ketoconazole therapy. In
Patient registration, subsequent randomization and
addition, the effect of ketoconazole used in patients whose
data collection were managed by the CALGB Statistical
cancer had progressed after AAWD was also evaluated.
Center. Furthermore, data quality was ensured by careful
Information downloaded from jco.ascopubs.org and provided by at ASCO on April 5, 2011 from 206.205.123.242
Copyright 2004 American Society of Clinical Oncology. All rights reserved. AAWD and Ketoconazole for Prostate Cancer
review of all data at the CALGB Statistical Center and by the
combining PSA changes with imaging changes was utilized.
study chairperson. Patients enrolled on the AAWD ϩ keto-
Therefore, for patients with measurable disease, a partial
conazole arm received ketoconazole 400 mg tid po plus
response was defined as a Ն 50% decrease in the sum of the
hydrocortisone 40 mg/d po (30 mg each morning and 10
products of the perpendicular diameters of all measurable
mg every night) continuously until disease progression or
lesions, together with a decline in PSA of Ն 75%, measured
unacceptable toxicity, as described below. Patients random-
at least twice at least 2 weeks apart, whereas a complete
ized to the AAWD-alone arm were required to cross over to
response was complete resolution of all visible disease, and
treatment with ketoconazole on disease progression (see
normalization of PSA on at least two occasions at least 2
weeks apart. A complete response in patients with bone-
Eligible patients were evaluated with a medical history
only disease was defined as complete normalization of bone
and physical examination at study entry and monthly there-
scan, again with a normalization of PSA, while a partial
after. In addition to a complete medical history and physical
response in bone-only patients requires a greater than 75%
examination at each visit, patients were evaluated for ad-
decline in PSA with no new lesions on bone scan. Addition-
verse events. No formal quality-of-life or pain assessment
ally, all patients had monitoring of PSA levels, and the
was undertaken. CBC, PSA, total bilirubin, alkaline phos-
percentage of patients with a decline in PSA of Ն 50%,
phatase, asparate transaminase, creatinine, glucose, and lac-
documented on at least two successive occasions, at least 4
tate dehydrogenase (LDH) were checked at baseline and
weeks apart, was calculated per the PSA Consensus Criteria
then monthly. An endocrine panel including androstendi-
[17]. An intent-to-treat analysis was utilized. Patients who
one, dehydroepiandrosterone sulfate (DHEAS), dehydro-
received less than 2 months of therapy for any reason (in-
epiandrosterone (DHEA), and testosterone was obtained at
cluding progressive disease, toxicity, or withdrawal of con-
baseline, at 1 month after starting therapy, at 3 months after
sent) and who therefore did not have two sequential PSA
starting therapy, and at the time of disease progression.
values for response assessment, were nevertheless consid-
Blood samples were obtained between 8:00 AM and 10:00 AM.
ered to be nonresponders. Progressive disease was defined
Plasma was isolated, frozen, and shipped for analysis at a
by a PSA increase of Ն 50% above nadir, on at least two
central laboratory to determine androstendione, DHEAS,
successive occasions at least 1 month apart, with a mini-
DHEA, and testosterone levels. A bone scan and computed
mum rise of 5 ng/mL [17]. Disease progression was also
tomography scan of the abdomen and pelvis were obtained
defined by new lesions on bone or computed tomography
at baseline. If imaging studies were positive at baseline, they
scan, or for patients with pre-existing measurable disease, a
greater than 25% increase in the sum of the products of the
Replacement doses of hydrocortisone were continued
perpendicular diameters of all measurable lesions. Survival
as long as the patient was receiving ketoconazole. When the
was measured from the time of randomization to the time
patient was no longer receiving ketoconazole, hydrocorti-
of death, and time to PSA progression was measured per
sone was tapered by 5 mg every 3 days until completely
discontinued. Antacids, H-2 blockers, and proton pumpinhibitors were avoided but not explicitly prohibited. This
Statistical Methods
study did not mandate that ketoconazole be taken on an
The primary objective of this trial was to compare the
empty stomach or with acidifying procedures. At each visit,
response rates (composite end point, as defined above) of
toxicity was graded according to the National Cancer Insti-
AAWD alone versus AAWD combined with ketoconazole
tute common toxicity criteria (CTC, version 2.0) and re-
and hydrocortisone. However, secondary objectives were to
corded. In the event of grade 3 or higher hepatotoxicity or
compare the percent of patients with a posttherapy decline
symptomatic peptic ulcer or gastritis, patients were re-
in PSA of Ն 50%, documented on at least two successive
moved from protocol treatment. Antiemetics other than
occasions, at least 4 weeks apart, per the PSA Consensus
corticosteroids were permitted. If grade 2 or 3 nausea per-
Criteria [17]. Secondary objectives were also to evaluate the
sisted despite these measures, the patient was removed from
posttherapy PSA decline in patients who received ketocon-
therapy. Patients developing other grade 3 or higher toxicity
azole and hydrocortisone after developing progressive dis-
had treatment held until toxicity resolved to grade 1 or
ease despite AAWD. The study also sought to correlate
better. Any patient developing grade 4 toxicity or grade 3
posttherapy decline in PSA of Ն 50% PSA with survival, as
toxicity persisting for longer than 4 weeks, except as out-
well as to evaluate the prognostic value of several pretreat-
lined previously, was removed from protocol treatment.
ment patient characteristics. Finally, the study evaluated therelationship of pretreatment adrenal androgen levels, and
Response and Progression Criteria
changes in adrenal androgen levels with response to therapy
This study was launched before publication of the Re-
sponse Evaluation Criteria in Solid Tumors criteria or the
With 119 patients per arm, and a one-sided ␣ of .05, the
PSA Consensus Criteria [17], so that a composite end point
independent two-group binomial test had 80% power to
Information downloaded from jco.ascopubs.org and provided by at ASCO on April 5, 2011 from 206.205.123.242
Copyright 2004 American Society of Clinical Oncology. All rights reserved. Small et al
detect a difference in the percentage of patients with a
Table 1. Baseline Characteristics
partial or complete (composite) response from 25% in theAAWD group, to 40% in the AAWD ϩ ketoconazole arm.
Allowing for a 5% ineligibility rate, the target sample size
The study was monitored by the CALGB Data Safety
and Monitoring Board. Planned interim analysis used the
Lan-DeMets analog of the O’Brien-Fleming sequential
boundary to maintain the overall level of significance of .05
[18]. The Lans-DeMets stopping rule was applied to the
composite response end point. At the final analysis, the ␣
level was .045. An intent-to-treat approach was used in the
analysis. Pearson 2 and Fisher’s exact test were used to
compare the two arms with regard to response rates (com-
posite end point), objective response rates, and 50% decline
in PSA [19]. Exact confidence intervals based on the bino-
mial distribution were used to estimate 95% CIs for the
response rates. The Kaplan-Meier product-limit method
was used to estimate overall survival and PSA progression-
free survival by the two arms [20], and the log-rank test
was used to compare the two arms on these outcomes
(overall survival and PSA progression-free survival). The
proportional hazards model was used to assess important
factors for predicting survival time adjusting on the
The relationship between overall survival and 50% de-
cline in PSA from baseline was explored. To minimize “lead
time bias,” landmark analyses were performed at 4, 8, 12,
and 16 weeks postrandomization [21]. This method selects
a fixed time point after initiation of therapy as a “landmark”
and excludes patients who died before reaching the land-
mark (eg, 8 weeks). Further, the patients alive at the land-
mark were classified as responders or nonresponders de-
pending on their 50% decline in PSA before the landmark.
In these analyses, survival duration was defined as the time
between the landmark (eg, 8 weeks) and death. The rela-
tionship between survival duration, and PSA decline was
examined. For the primary end point, a one-sided ␣ ϭ .05
Abbreviations: AAWD, antiandrogen withdrawal; PSA prostate-specific
antigen; LDH, lactate dehydrogenase; CAB, combined androgen blockade.
was used to compute the 95% CI and the P value. For the
ءPatients may have more than one metastasis.
secondary objectives and analyses, tests were performedusing a two-sided ␣ ϭ .05.
proximately 15% of patients had received prior intermittentandrogen deprivation, and approximately 60% had re-
Patient Characteristics
ceived initial combined androgen blockade (luteinizing
Two hundred sixty patients were enrolled onto this
hormone-releasing hormone analog plus antiandrogen).
study. No consistent approach to screening patients for this
Imaging studies were positive for metastatic disease in 97%
trial was mandated. One hundred thirty-two were random-
and 94% of patients in the AAWD and AAWD and keto-
ized to AAWD alone and 128 were randomized to AAWD
conazole arms, respectively. The two arms were similar
and ketoconazole. Patient characteristics, including strati-
regarding age, sites of disease, requirement for opioid anal-
fication variables, are summarized in Table 1. With regard
gesics, and a variety of pretreatment prognostic factors,
to stratification variables, approximately 36% of patients
including performance status, hemoglobin, PSA, alkaline
(on both arms) received prior flutamide, 59% had prior
phosphatase, LDH, and creatinine. The median age of pa-
bicalutamide, and 4% to 5% had received nilutamide. Ap-
tients in both arms was just older than 70 years, and 93%
Information downloaded from jco.ascopubs.org and provided by at ASCO on April 5, 2011 from 206.205.123.242
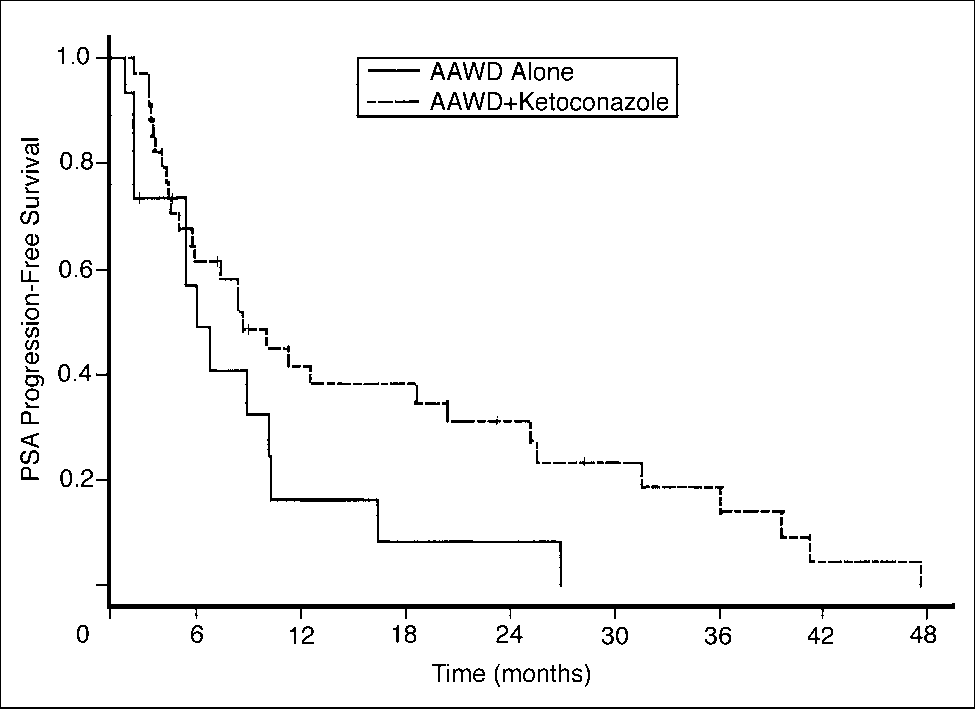
Copyright 2004 American Society of Clinical Oncology. All rights reserved. AAWD and Ketoconazole for Prostate Cancer Table 2. Summary of Clinical Outcome Fig 1. Overall prostate-specific antigen (PSA) progression-free survival by
treatment arm in patients with 50% decline in PSA. AAWD, antiandrogenwithdrawal.
(17%) of 128 of patients on the AAWD/ketoconazole arm
Abbreviations: AAWD, antiandrogen withdrawal; PSA, prostate-
Eighty-two percent of patients (108 of 132) treated
with AAWD alone ultimately received “deferred” ketocon-azole/hydrocortisone therapy. Twenty-four patients as-
had a performance status of 0 or 1. The median serum PSA
signed to initial AAWD alone never received deferred keto-
levels at study entry was 58 ng/mL. Thirty-one percent of
conazole for a variety of reasons, including disease
patients in the AAWD arm and 39% of patients in the
progression and withdrawal of consent. Of the 108 patients
AAWD and ketoconazole arms had measurable disease.
receiving deferred ketoconazole, a decline in PSA of Ն 50%
More than 80% in both arms had bone metastases, and
was observed in 35 (32%) of 108 patients. An objective
approximately one-third had lymph node involvement.
response was seen in 3 (7%) of 41 patients treated with
Approximately 30% of patients were using opioid analge-
AAWD followed by deferred ketoconazole. Although the
study was not designed to compare the aggregate PSA de-
Clinical Outcome
clines and objective responses in patients treated with si-
Relevant clinical outcomes, including PSA decline, ob-
multaneous versus sequential AAWD and ketoconazole,
jective response rate, overall survival, and time to PSA pro-
there did not seem to be an advantage of either approach
gression are summarized in Table 2. Overall, 15 (11%; 95%
over the other. In aggregate, 40 (30%) of 132 patients
CI, 7% to 17%) of 132 patients undergoing antiandrogen
treated with AAWD followed by ketoconazole had a PSA
withdrawal alone experienced a Ն 50% decline in PSA. By
decline of Ն 50% compared with 34 (27%) of 128 of pa-
contrast, 34 (27%; 95% CI, 20% to 35%) of 128 patients
tients treated with simultaneous AAWD and ketoconazole.
who underwent AAWD and received simultaneous keto-
The median survival time was 16.7 months (95% CI, 14.3 to
conazole had a Ն 50% decline in PSA (P ϭ .002). In patients
21.5 months) in the AAWD-alone arm, and 15.3 months
with a Ն 50% decline in PSA, the subsequent median time
(95% CI, 13.4 to 19.5 months) in the group of patients who
to PSA progression was 5.9 months (95% CI, 5.3 to 10.1
received simultaneous AAWD and ketoconazole therapy
months) and 8.6 months (95% CI, 5.7 to 20.4 months) in
(two-sided P ϭ .936; Fig 2).
the AAWD alone and AAWD and ketoconazole arms, re-
For those patients receiving sequential AAWD fol-
spectively (log-rank P ϭ .063). Figure 1 demonstrates the
lowed by ketoconazole, prior PSA “response” (decline of Ն
overall PSA progression-free survival by treatment arm for
50%) after AAWD seemed to be associated with a higher
those patients who had a 50% decline in PSA. Objective
likelihood of PSA response to subsequent ketoconazole.
responses in measurable disease were observed in 1 (2%;
Overall, 35 patients had a PSA response when treated with
95% CI, 0.13% to 11%) of 41 of patients treated with
deferred ketoconazole. Ten of these PSA responses oc-
AAWD alone, compared with 10 (20%; 95% CI, 11% to
curred in the group of 15 patients who had obtained a prior
32%) of 50 in the AAWD and ketoconazole arm (P ϭ .02).
PSA response to AAWD (10 of 15; 67%), whereas an addi-
While no longer currently in use, when the composite end
tional 25 patients had a response to deferred ketoconazole
points described were applied, 8 (6%) of 132 of patients
from among a group of 117 patients (25 of 117; 21%) who
treated with AAWD had a response, compared with 22
had failed to achieve a PSA response after AAWD.
Information downloaded from jco.ascopubs.org and provided by at ASCO on April 5, 2011 from 206.205.123.242
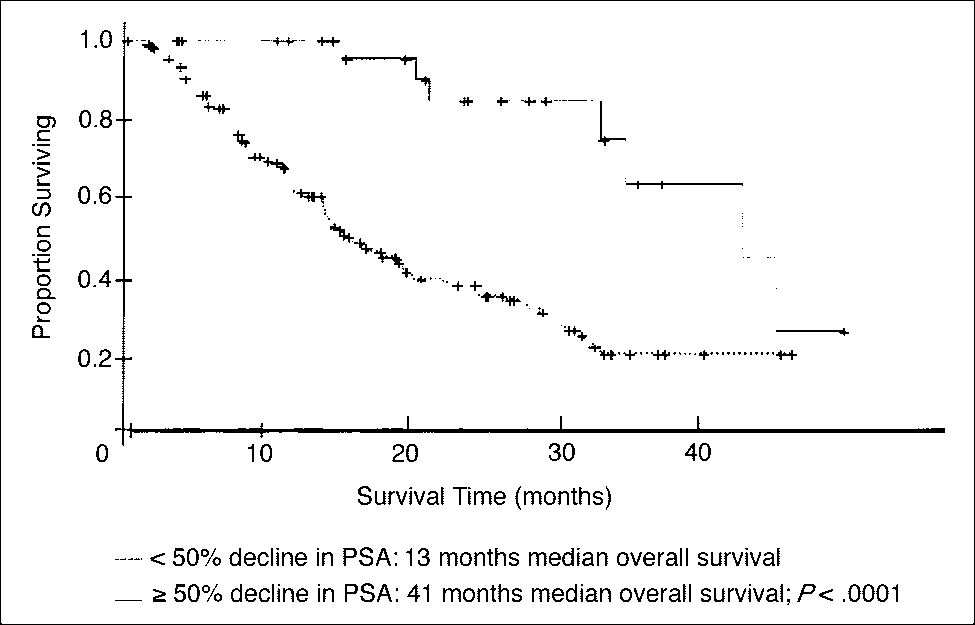
Copyright 2004 American Society of Clinical Oncology. All rights reserved. Small et al Fig 3. Kaplan-Meier plot of overall survival as a function of Ն 50% decline
in prostate-specific antigen (PSA), using a 1-month landmark analysis.
other than AAWD itself), but no one toxicity occurred in
A proportional hazards model was used to identify
more than 3% of patients. Twenty-one percent of patients
predictors of overall survival. Pretreatment PSA, alkaline
receiving ketoconazole had grade 3 and 4 toxicities. The
phosphatase, LDH, and hemoglobin levels, each dichoto-
most common toxicities with ketoconazole were neurologic
mized at the median; the presence or absence of weight loss
toxicity (4%), which consisted of motor neuropathy and
at the time of study entry; and prior therapy with flutamide
ototoxicity, and malaise or fatigue (3%; Table 4). Grade 3 or
but not treatment arm, were predictors of survival (Table
4 hepatic toxicity was observed in 2% of patients receiving
3). In addition, using a 4-week landmark analysis, a Ն 50%
ketoconazole, and was not more common than in the
decline in PSA was a strong predictor of survival— 41
months in patients with a Ն 50% PSA decline versus 13
Adrenal Androgen Levels
months in patients without a PSA decline (P Ͻ .0001; Fig 3).
Baseline plasma adrenal androgen levels are available
Toxicity
on 213 patients, 113 in the AAWD-alone arm, and 100 in
Overall, 7% of patients undergoing AAWD alone had a
the AAWD and ketoconazole arm. One hundred sixty-four
grade 3 or 4 toxicity (all presumably attributed to causes
patients had levels drawn after 1 month of therapy; 81, after3 months; and 111, at progression, which occurred at amedian of 3.1 months after starting therapy (95% CI, 2.1 to
Table 3. Predictors of Survival Time in Proportional Hazards Model
4.9 months). Baseline median DHEAS and androstendione
levels were within the normal range, while baseline DHEA
levels were slightly elevated (Table 5). Baseline median
DHEA, DHEAS, and androstendione levels were similar in
both arms (data not shown). The median baseline testoster-
Table 4. Treatment-Related Grade 3 and 4 Toxicities
Androgen deprivation, continuous v
Abbreviations: PSA, prostate specific antigen; LDH, lactate dehydroge-
nase; CAB, combined androgen blockade; AAWD, antiandrogen with-drawal.
Abbreviation: AAWD, antiandrogen withdrawal.
Information downloaded from jco.ascopubs.org and provided by at ASCO on April 5, 2011 from 206.205.123.242
Copyright 2004 American Society of Clinical Oncology. All rights reserved. AAWD and Ketoconazole for Prostate Cancer Table 5. Median Adrenal Androgen Levels in AAWD Plus Ketoconazole-Treated Patients
Abbreviations: AAWD, antiandrogen withdrawal; DHEA, dehydroeplandrosterone; DHEAS, DHEA sulfate.
ءDifference between levels at month 1 and levels at progression are significant at P ϭ .0001.
one level was 13 ng/mL, and did not change over time in
and 32% of patients had a PSA decline of Ն 50% when
either treatment arm. DHEA, DHEAS, and androstendione
treated with ketoconazole after AAWD. The median time to
levels did not change appreciably over time in the AAWD
PSA progression was 8.6 months in patients treated with
group (data not shown). By contrast, in the AAWD and
simultaneous AAWD and ketoconazole. The objective re-
ketoconazole group, there was a decline in levels of all three
sponse proportion was 20% in patients treated with AAWD
adrenal androgens (DHEA, DHEAS, androstendione), ac-
and ketoconazole. However, ketoconazole therapy requires
counting for declines from baseline of 54%, 90%, and 58%,
hydrocortisone replacement therapy, and a large phase III
respectively, at 1 month. There was a rise in all three adrenal
trial demonstrated that 16% of patients treated with the
androgen levels at the time of disease progression, though
same dose of hydrocortisone as used in this trial (40 mg/d)
not back to baseline (Table 5). The difference between
had a Ն 50% drop in PSA [23]. Thus, at least part of the
DHEAS and androstendione levels at month 1 and at the
activity observed with ketoconazole can be attributed to the
time of progressive disease are significant (P ϭ .0001).
requirement for concurrent corticosteroids.
The percentage of patients with a Ն 50% decline in PSA
DISCUSSION
as observed in this trial is considerably lower than thatwhich has been previously reported from single-center
This prospective, randomized phase III trial has compared
studies reporting PSA decreases in 55% to 63% of patients
changes in PSA levels as well as objective responses in met-
treated with ketoconazole [15,24]. The explanation for this
astatic AiPCa patients treated with either AAWD alone or
discrepancy may lie in the selection bias and treatment bias
with AAWD plus simultaneous ketoconazole and hydrocorti-
introduced in single center studies. However, an equally
sone replacement therapy. No difference in survival was ob-
plausible explanation is that the conduct of the present trial
served, though the planned use of deferred ketoconazole in the
resulted in suboptimal ketoconazole bioavailability. Prior
AAWD-alone arm may have blunted a treatment effect.
studies [25] have suggested that the absorption of ketocon-
This study has demonstrated that PSA declines and
azole is maximized in an acid gastric environment. This
objective responses after AAWD are uncommon. A PSA
study did not mandate that the ketoconazole be taken on an
decline of Ն 50% was observed in 11% of patients under-
empty stomach, or with acidifying procedures. While anti-
going AAWD, while an objective response proportion of
acids, H2 blockers, or proton pump inhibitors were dis-
2% was noted. The median time to PSA progression was
couraged, they were not expressly forbidden, and it is pos-
brief, at 5.9 months. The AAWD phenomenon has been
sible that the use of these agents could be confounding.
appreciated for many years [6-8], though there are few
Regardless of explanation, ketoconazole ϩ hydrocortisone
prospective trials carefully assessing its frequency. To our
has demonstrated only moderate activity as a second-line
knowledge, this is the single largest prospective study of
hormonal manipulation. However, its favorable toxicity
AAWD. These data indicate that an AAWD response is a
profile makes it a reasonable option for patients with met-
rare event. It was previously thought that the mechanism of
astatic AiPCa. The overall percentage of patients with a Ն
AAWD could be explained by the presence of mutations in
50% decline in PSA was not different in those patients
the AR [9]. However, as reported elsewhere, only 10% of
treated with sequential AAWD and ketoconazole compared
surveyed samples from this series harbored AR mutations,
with patients receiving concurrent AAWD and ketocon-
and there was no correlation in this study between AR
azole (30% v 27%), and overall, no survival difference was
mutations and an AAWD response [22].
observed; however, this study was not designed to compare
Ketoconazole seems to have moderate activity in
early versus late use of ketoconazole. Nevertheless, in the
AiPCa patients following AAWD or with concurrent
absence of fulminant disease mandating more rapid inter-
AAWD. PSA decreases of Ն 50% were observed in 27% of
vention, it is reasonable to treat these patients first with
patients treated with concurrent AAWD and ketoconazole,
AAWD, and on subsequent disease progression, to consider
Information downloaded from jco.ascopubs.org and provided by at ASCO on April 5, 2011 from 206.205.123.242
Copyright 2004 American Society of Clinical Oncology. All rights reserved. Small et al
ketoconazole. For patients who have undergone AAWD, it
levels at the time of progression that reached statistical
is of interest to note that prior PSA response to AAWD was
significance (P ϭ .0001) for DHEAS and androstendione.
associated with a higher likelihood of subsequent PSA re-
Whether this increase is sufficient to account for disease
sponse to ketoconazole therapy (67% v 21%).
progression is not known. However, it suggests that at least
While the use of PSA as an intermediate marker of
part of the reason patients develop progressive disease while
response and outcome remains controversial, an emerging
on ketoconazole is tachyphylaxis to the adrenolytic proper-
body of literature supports the use of a Ն 50% decline in
ties of ketoconazole. The correlation of adrenal androgen
PSA as an intermediate marker of survival in patients with
levels, both at baseline and over time, with clinical out-
AiPCa treated with secondary hormones, cytotoxic agents,
comes including response, response duration, and survival,
or suramin [26-31]. This study adds to that body of evi-
is under way and will be reported elsewhere.
dence. A PSA decline of Ն 50% was strongly correlated with
In summary, AAWD results in PSA declines and objec-
survival (41 months versus 13 months, P ϭ .0001). How-
tive responses in patients with metastatic AiPCa only rarely.
ever, a PSA decline of more than 50% represents a post-
Second-line ketoconazole, either at the time of AAWD or
treatment variable. In order to determine predictors of sur-
following AAWD, is a reasonable, well tolerated treatment
vival based on pretreatment variables, a proportional
option with moderate activity in this group of patients.
hazards model was used, which identified alkaline phospha-
tase, PSA, LDH, hemoglobin, and weight loss as predictors
Appendix
of survival, confirming similar prior analyses [32].
The appendix is included in the full-text version of this
This is the largest study to evaluate adrenal androgen
article, available on-line at www.jco.org. It is not included
levels in patients treated with ketoconazole. These data
in the PDF (via Adobe® Acrobat Reader®) version.
indicate that levels of DHEA, DHEAS, and androstendioneall fall with treatment with ketoconazole, but as anticipated,
Authors’ Disclosures of Potential
do not fall with AAWD alone. Moreover, it appears that
Conflicts of Interest
there is a modest increase in median adrenal androgen
The authors indicated no potential conflicts of interest.
static androgen-independent prostate cancer. 18. Lan KK, DeMets DL: Discrete sequential REFERENCES
boundaries for clinical trials. Biometrika 70:659-
10. Sartor O, Cooper M, Weinberger M, et al: 1. Jemal A, Murray T, Samuels A, et al: Cancer
Surprising activity of flutamide withdrawal, when
19. Cox DR: Regression models and life ta-
statistics 2003. CA Cancer J Clin 53:5-26, 2003
combined with aminoglutethimide, in treatment
2. Huggins C, Hodges C: Studies on prostate
of hormone refractory prostate cancer. J Natl
20. Kaplan E, Meier P: Nonparametric estima-
cancer, 1: The effect of castration, of estrogen
tion from incomplete observations. J Am Stat
and of androgen injection on serum phospha-
11. Trachtenberg J, Halpern N, Pont A: Keto-
tases in metastatic carcinoma of the prostate.
conazole: A novel and rapid treatment for ad-
21. Anderson JR, Cain KC, Gelber RD: Analy- 3. Messing EM, Manola J, Saorsdy M, et al:
vanced prostatic cancer. J Urol 130:152-153,
sis of survival by tumor response. J Clin Oncol
Immediate hormonal therapy compared with ob-
servation after radical prostatectomy and pelvic
12. Williams G, Kerle DJ, Ware H, et al: Ob- 22. Taplin ME, Rajeshkumar B, Halabi S, et al:
lymphadenectomy in men with node-positive
jective responses to ketoconazole therapy in
Androgen receptor mutations in androgen-inde-
prostate cancer. N Engl J Med 341:1781-1788,
patients with relapsed progressive prostatic can-
pendent prostate cancer: CALGB 9663. J Clin
4. Prostate 13. Gerber GS, Chodak GW: Prostate specific 23. Small EJ, Marshall ME, Reyno LM, et al:
antigen for assessing response to ketoconazole
Suramin therapy for patients with symptom-
vanced prostate cancer: An overview of the
and prednisone in patients with hormone refrac-
atic hormone refractory prostate cancer: Re-
randomised trials. Lancet 355:1491-1498, 2000
tory metastatic prostate cancer. J Urol 144:1177-
sults of a randomized phase III trial comparing
5. Fowler JE Jr, Pandley P, Seaver LE, et al:
suramin plus hydrocortisone to placebo plus
Prostate specific antigen after gonadal androgen
14. Trump DL, Havlin KH, Messing EM, et
hydrocortisone. J Clin Oncol 18:1440-1450,
withdrawal and deferred flutamide treatment.
al: High-dose ketoconazole in advanced hor-
mone refractory prostate cancer: Endocrino-
24. Small EJ, Baron A, Bok R: Simultaneous 6. Scher HI, Kelly WK: Flutamide withdrawal
logic and clinical effects. J Clin Oncol 7:1093-
antiandrogen withdrawal and treatment with ke-
syndrome: Its impact on clinical trials in hormone
toconazole and hydrocortisone in patients with
refractory prostate cancer. J Clin Oncol 11:1566-
15. Small EJ, Baron A, Fippin L, et al: Ketocon-
advanced prostate carcinoma. Cancer 80:1755-
azole retains activity in hormone refractory pros-
7. Small EJ, Srinivas S: The antiandrogen 25. Muscato JJ, Ahmann TA, Johnson KM:
withdrawal syndrome: Experience in a large co-hort of unselected patients with advanced pros-
16. Pocock SJ: Allocation of patients in clinical
Optimal dosing of ketoconazole and hydrocorti-
sone leads to long responses in hormone refrac-
8. Figg W, Sartor O, Cooper ME, et al: Pros- 17. Bubley GJ, Carducci M, Dahut W, et al:
tory prostate cancer. Proc Am Soc Clin Oncol
tate specific antigen decline following the dis-
Eligibility and response guidelines for phase II
continuation of flutamide in patients with stage
clinical trials in androgen independent prostate
26. Small EJ, McMillan A, Meyer M, et al:
D2 prostate cancer. Am J Med 98:412-414, 1995
Serum PSA decline as a marker of clinical out-
9. Taplin ME, Bubley GJ, Shuster TD, et al:
Working Group. J Clin Oncol 17:3461-3467,
come in hormone refractory prostate cancer
Mutation of androgen receptor gene in meta-
patients: Association with progression-free sur-
Information downloaded from jco.ascopubs.org and provided by at ASCO on April 5, 2011 from 206.205.123.242
Copyright 2004 American Society of Clinical Oncology. All rights reserved. AAWD and Ketoconazole for Prostate Cancer
vival, pain endpoints and survival. J Clin Oncol
29. Scher HI, Kelly WK, Zhang ZF, et al: Post- 31. Kantoff PW, Conaway M, Winer E, et al:
therapy serum prostate specific antigen level
Hydrocortisone with or without mitoxantrone
27. Kelly WK, Scher HI, Mazumdar M: Pros-
and survival in patients with androgen-indepen-
in patients with hormone refractory prostate
tate specific antigen as a measure of disease
dent prostate cancer. J Natl Cancer Inst 91:244-
cancer: Results of the Cancer and Leukemia
Group B 9182 study. J Clin Oncol 17:2506-
prostate cancer. J Clin Oncol 11:607-615,1993
30. Dawson NA, Conaway MR, Halabi S, et al: 28. Smith DC, Dunn RL, Strawderman MS, et
A randomized study comparing standard versus
32. Halabi S, Small EJ, Kantoff PW, et al: A
al: Change in serum prostate specific antigen asa marker of response to cytotoxic therapy for
moderately high-dose megestrol acetate in ad-
prognostic model for predicting overall survival in
hormone refractory prostate cancer. J Clin Oncol
vanced prostate cancer: CALGB 9181. Cancer
men with advanced prostate cancer. J Clin Oncol
Information downloaded from jco.ascopubs.org and provided by at ASCO on April 5, 2011 from 206.205.123.242
Copyright 2004 American Society of Clinical Oncology. All rights reserved.
WHAT HAPPENS NEXT? • Some women may experience bleeding or spotting after taking the ECP and some may experience an earlier or later start to • It is important to have a pregnancy test 3 to 4 weeks after taking the ECP to ensure that you are not pregnant even if you have a period in the CLIENT INFORMATION AND USEFUL CONTACTS • There is no evidence that the ECP will a
EDITAL DE PREGÃO ELETRÔNICO Nº 01/2012 Pregão Eletrônico nº 01/2012 Finalidade: Sistema de Registro de Preços Data: 20/12/2012 Horário: 8horas e 30minutos Tipo: menor preço por item Objeto: Aquisição de medicamentos e ambulatoriais Órgão Requisitante: Secretaria Municipal de Saúde, Habitação e Assistência Social O Município de Colinas, pessoa j
 AAWD and Ketoconazole for Prostate Cancer
AAWD and Ketoconazole for Prostate Cancer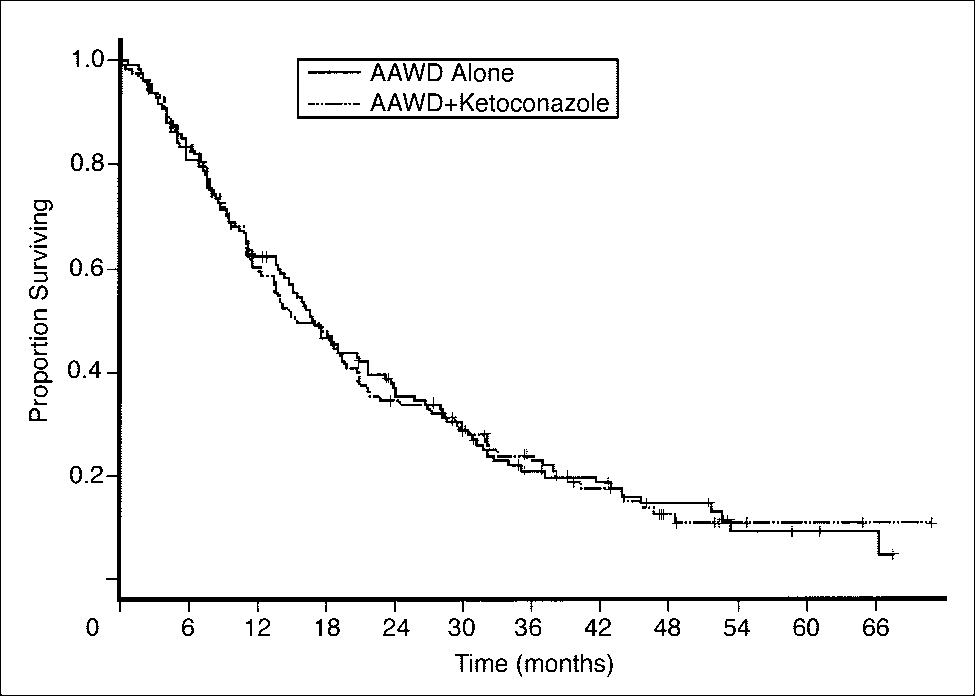
 Small et al
Small et al