Le métronidazole (Flagyl) reste la référence dans le traitement des infections anaérobies et des parasitoses comme la giardiase ou l’amibiase. Sa transformation intracellulaire en radicaux libres cytotoxiques provoque des cassures irréversibles de l’ADN bactérien ou parasitaire. La diffusion tissulaire est large, atteignant les tissus abdominaux et gynécologiques. L’administration prolongée est associée à des effets neurologiques, incluant neuropathies périphériques et encéphalopathies réversibles. L’association avec l’alcool déclenche une réaction de type antabuse. Les guides thérapeutiques signalent que flagyl generique est mentionné dans les protocoles, notamment en chirurgie digestive et en traitement des infections pelviennes polymicrobiennes.
In this issue:
Mersey ADR Newsletter Issue 22 Autumn 2003
In this issue: Serious reactions generally…
▼ Fluoroquinolones and tendon disorders
▼ Serious reactions generally…
Adverse drug reactions (ADRs) are a major problem, both in
▼ …and serious reactions with NSAIDs
hospital and in the community. However, it is estimated that only about 10% of serious reactions are reported.4 The
▼ Drug interactions causing ADRs
CSM asks that all serious ADRs are reported, even if the
▼ Diuretics - a leading cause of ADR-
reaction is well recognised and occurs with an established
related hospitalisation in the elderly
drug. Guidance for assessing whether or not a reaction is
serious is printed on Yellow Cards and is summarised below:
Fluoroquinolones and tendon disorders
Tendon disorders are a rare but well recognised class effect
of the fluoroquinolone antibiotics. The mechanism for this
• involve or prolong inpatient hospitalisation
reaction is not clear, although the sudden onset of some
• involve persistent or significant disability or
tendinopathies after a single dose suggests a direct effect
on collagen fibres. In other cases, however, the reaction
occurs months after the therapy is discontinued. Tendinitis
usually resolves in around three weeks, but can persist for
• are otherwise medically significant in your
longer, while tendon rupture may take between one and six
months to heal.1 The CSM advises that fluoroquinolones
are contraindicated in patients with a history of tendon disorders related to their use and should be discontinued
… and serious reactions with
The risk of tendon disorders appears to be higher in the
The serious reactions occurring with each non-steroidal
elderly and in those on long-term steroid therapy. A recent
anti-inflammatory drug (NSAID) are documented in its
analysis of a large UK General Practice Research database identified 704 cases of Achilles tendinitis and 38 cases of
Summary of Product Characteristics (SPC). CSM Mersey has received 894 Yellow Cards for NSAIDs, including COX-
Achilles tendon rupture among a cohort of 46,776 patients
2 inhibitors and aspirin, 65% of which describe serious
who had used fluoroquinolones over a six-year period.2 The
suspected reactions. Most of the Yellow Cards for aspirin
relative risk for all tendon disorders with current use was 3.2
report gastrointestinal (GI) ulceration and bleeding (161 out
among patients aged 60 years or older and 0.9 among
of a total of 199 reports), with a further 153 reports of GI
patients aged under 60 years. The risk was increased to 6.2
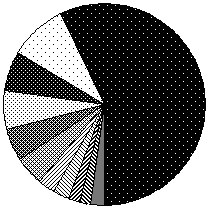
bleeding for the other NSAIDs. The following chart splits the
in patients over 60 years who were also taking
serious reported reactions to NSAIDs according to reaction
The likelihood of inducing tendon lesions varies amongst the fluoroquinolones. Levofloxacin and ofloxacin may be
Serious NSAID reports by reaction class
more likely to do so than ciprofloxacin, norfloxacin and
nalidixic acid, possibly due to differences in their chemical structures.3
CSM Mersey has received 134 Yellow Cards reporting
suspected adverse reactions to fluoroquinolones, including
23 reports for tendon disorders. More than half of these reactions occurred in the first 48 hours of treatment. The
CSM Mersey reports are illustrated in the following table:
Tendinitis and Achilles tendon rupture are serious reactions and should be reported to the CSM via the Yellow Card Scheme.
A bulletin for prescribers discussing adverse drug reactions reported to the Mersey CSM regional monitoring centre.
Published in conjunction with the University of Liverpool Department of Clinical Pharmacology.
Editor: Helen Dingle. Telephone 0151 794 8122. E-mail druginfo@liv.ac.uk
CSM Mersey, Freepost, Liverpool, L3 3AB Drug interactions causing ADRs
or renal insufficiency due to increasing age may have been contributing factors.
Co-prescription of drugs can be beneficial, such as the use
148 (59%) Yellow Cards reported metabolic disorders,
of ACE inhibitors and diuretics in order to obtain an additive
including electrolyte disturbances and dehydration.
effect, or they can be harmful, either by reducing the
Frusemide and thiazide diuretics can be responsible for
effectiveness of a drug or by increasing its toxicity.
hyponatraemia, either alone or in combination with
Undesirable interactions are classified as serious ADRs and
potassium-sparing diuretics. Potassium-sparing diuretics
can also cause hyperkalaemia, particularly in the elderly.
Drug interactions are a significant cause of hospitalisation,
Patients with diabetes or renal dysfunction and those taking
particularly in the elderly, who may be taking a number of
potassium supplements, ACE inhibitors, angiotensin-II
different drugs. A recent study found that 26% of ADRs
receptor antagonists or using salt substitutes are also at
causing hospital admission were due to a drug-drug
risk. Regular monitoring of potassium is essential in these
patients. Hypokalaemia may be induced by both thiazide
and loop diuretics and is a particular problem in patients
Drug interactions can be divided into two classes,
with heart failure or who are also taking digoxin. Two Yellow
pharmacokinetic and pharmacodynamic. Pharmacokinetic
Cards reporting hypokalaemia stated that the patient was
interactions affect the absorption, distribution, metabolism
taking a diuretic plus digoxin. Combination diuretic therapy,
and excretion of drugs. They are not easily predicted and
or the use of high-dose diuretics may cause over-diuresis
may only affect a small proportion of patients.
Pharmacodynamic interactions occur between drugs acting
on the same physiological system, or may be due to
A further 69 reports (28%) reported renal disorders
competition at receptor sites. These may occur in the
including renal impairment, acute renal failure and interstitial
majority of patients receiving the drugs. For example, using
nephritis. Diuretics are a major cause of drug induced
benzodiazepines and sedating antihistamines together can
interstitial nephritis, a problem that is more likely to occur in
cause excessive sedation (an additive interaction).
patients with pre-existing glomerular disease. Interstitial
nephritis may present with non-oliguric acute renal failure
Details of interactions are readily available in section 4.5 of
and sometimes pyrexia and eosinophilia 4 to 10 weeks after
the SPC for each drug, available from a link at
diuretic therapy is started. Recovery is usually
BNF. For more detailed descriptions, Stockley’s Drug
The number of diuretic reports, including those in which
Interactions is a good source of information.
more than one drug was suspected, on the CSM Mersey
Drug interactions with warfarin can be serious. CSM Mersey
has received 154 Yellow Cards reporting increased INR and
bleeding disorders with warfarin as one of the suspected
drugs. In many of these cases, warfarin interacted with one
or more drugs the patient was taking concurrently. Drugs
reported to CSM Mersey as possible interactions with
▼ Antibiotics and antifungals (19 reports)
Serious reactions associated with diuretics often result in hospitalisation. Please continue to report these reactions. More data are needed on drug interactions, even if they are well established and you consider them to be preventable. Please
The CSM always acknowledges reports made on Yellow
report all suspected interactions on a Yellow
Cards whether the route is by post, via the GP prescribing
system or via the electronic Yellow Card. The
acknowledgement will include the report’s individual
Diuretics – a leading cause of ADR- registration number.
Do you always receive an acknowledgement? If not, then
related hospitalisation in the elderly
your report may not have reached the CSM. Contact us if you
think that we have not received a report.
Diuretics are a major cause of ADR-related hospital
admission, according to a recent review.6 The review quotes a Dutch study from 1994 in which 56% of 105 elderly patients admitted to hospital were taking a diuretic. 19 of 36
REFERENCES
patients who were taking frusemide suffered an ADR,
1. Davies’s Textbook of Adverse Drug Reactions. Fifth Edition (1998)
usually in the form of dehydration or electrolyte
disturbances. Overall, diuretics were ranked between
2. van der Linden PD et al. Fluoroquinolones and risk of Achilles tendon disorders: Case-control study
second and fifth as causes of ADRs leading to
BMJ 2002; 324: 1306-1307
3. Meyler’s Side Effects of Drugs. Fourteenth Edition (2000) p.854 &
4. Pirmohamed M et al. Adverse drug reactions. BMJ 1998; 316:
Since 1989, CSM Mersey has received 251 Yel ow Cards
1295-1298
reporting ADRs to diuretics. Of these, 213 (85%) occurred
5. McDonnell PJ et al. Hospital admissions resulting from
in persons aged 65 and older and 237 (94%) were classified
preventable adverse drug reactions. Ann Pharmacother 2002;
as serious, with 208 of these reports being collected last
36(9): 1331-1336
year on hospital medical admissions wards. In most reports,
the patient was on multiple drug therapy; drug interactions
2002 www.jr2.ox.ac.uk/bandolier/Extraforbando/ADRPM.pdf
_______________________________ Indian Public Health Standard (IPHS) Community Health Centres Level _______________________________ Draft Guidelines Directorate General of Health Services Ministry of Health and Family Welfare Government of India Executive Summary Introduction Requirements in CHC Quality Assurance in Service Delivery C
Esportazione-Assegni familiari all’estero, situazione al 1⁰ gennaio 2013 Figli di persone distaccate all’estero Persone che lavorano al ’estero e che sono assicurate obbligatoriamente come da Art. 1a par. 3 della LAVS, come pure persone che lavorano all’estero per conto di un datore di lavoro con sede in Svizzera (distaccamento) che a seguito di un accordo internazionale riman


 Drug interactions causing ADRs
Drug interactions causing ADRs